Journal of Depression and Anxiety
Open Access
ISSN: 2167-1044
ISSN: 2167-1044
Research Article - (2018) Volume 7, Issue 4
Background: Based on our observations, as physicians in a Referral Hospital, we have been noticing the association between history of enteric fever and somatic disorders associated with low mood. At our hospital, Al- Hussein University Hospital, Cairo, Egypt, we are receiving patients from all over Egypt, including rural areas where enteric fever is endemic. Here we report this series for 15 patients referred to us for evaluation of different somatic disorders.
Clinical presentation: After extensive evaluations, the patients’ symptoms were proved to be functional, their typhoid carrier states were documented, they were evaluated for depression using Hamilton-D questionnaire and the severity of depression was recorded. All patients were treated by ceftriaxone, 2 g, IV, daily for 15 days. Clinical evaluation and Hamilton score were reassessed at the end of treatment and 6 weeks thereafter. The patients did not receive any anti-depressant nor anti-anxiety treatment during their course. Typhoid carrier was defined by documenting the history of typhoid fever that was diagnosed by culturing the Salmonella species not by serology, plus at least one occasion of Salmonella isolates from stool culture while afebrile, plus absence of fever in the past 3 weeks. The Widal test wasn’t accepted as a criterion for enrolment.
Results: Patients showed clinically significant improvement in term of the presenting somatic complaints as well as their Hamilton-D score immediately post-treatment and consolidate for 6 weeks post-treatment completion.
Conclusion: Typhoid carrier in our series was associated with psychosomatic depression that improved on antibiotic therapy.
Keywords: Typhoid carrier; Depression; Psychosomatic
Typhoid fever is a global health problem, with approximately 21 million new cases infection by Salmonella typhi (S. typhi ) each year [1]. The mortality from typhoid fever increased by 39% between 1990 and 2010, with more than 190,000 persons die each year [2]. In South East Asia and Sub-Saharan Africa, it was estimated that the effect of typhoid fever in mortality is comparable to prostate, breast and leukaemia in western societies [2].
Approximately 2-5% of typhoid fever patients will turn to be chronic carriers [3], these carriers are asymptomatic, yet continue to excrete the organism for prolonged, ill-defined period and act as reservoirs for the organism [4]. Depression and low mood is associated with considerable morbidity and mortality [5] and it is expected to represent the second leading cause of disability worldwide by 2020, only after ischemic heart disease [6].
Chronic inflammatory disorders are associated with depression [7-10]. Excess levels of inflammatory cytokines; interleukin-1 (IL-1), interleukin-6 (IL-6), and interferon gamma (IFN-g), are associated with major depressive disorders [11]. Elevated level of Serum high sensitivity C-reactive protein was associated with increased risk of major depressive disorder [12]. The most striking observation, for the association between inflammatory cytokines and depression, comes from following hepatitis C patients, treated by interferon-α, which is an inflammatory cytokine. It was found that up to 50% of patients treated by interferon-α, developed clinically significant depression [13,14].
This inflammatory model of depression provides a possible link between the infection and depression. The association between typhoid fever and neuropsychiatric illness is documented in previous studies [15-17]. Through increasing inflammatory cytokines, typhoid vaccine was associated with significant short-term depression together with increased activity within the anterior cingulate cortex [18,19]. Our report is based mainly on our clinical observations as physicians in referral hospital in endemic country, Egypt.
Enrolment
This prospective cohort study describing 15 patients treated at Al- Hussein university hospital, Cairo, Egypt. The study time was from May 2015-September 2017. All patients were >18 years. Patients were refereed to us for evaluation of different somatic complaints. All patients were Egyptians and were coming from rural areas. They presented with combination of different somatic complaints. Table 1 shows the frequency of somatic complaints at presentation and 6 weeks after the end of treatment, see later.
| Characteristics | Cases number (%) |
|---|---|
| Sex | |
| Male | 8 (53%) |
| Female | 7 (47%) |
| Age, years, median (range) | 47 (19-63) |
| Rural destinations | 15 (100%) |
| Chronic diseases | |
| No | 10 (66%) |
| DM | 3 (20%) |
| HTN | 4 (26%) |
| Asthma | 1 (6%) |
| Smoking | |
| Yes | 6 (40%) |
| No | 9 (60%) |
| Positive examination findings at presentations, at 6th week point | |
| Pallor | 12 (80%), 3 (20%) |
| White coated tongue | 12 (80%), 2 (13%) |
| Right iliac fossa tenderness by deep palpations | 13 (86%), 1 (6%) |
| Imaging finding at presentations, at 6th week point | |
| Splenomegaly | |
| 12-15 cm | 8 (53%), 4 (26%) |
| >15 cm | 0 (0%), 0 (0%) |
| Hepatomegaly | 6 (40%), 6 (40%) |
| Thick wall gall bladder | 12 (80%), 12 (80%) |
| Gall bladder stone | 3 (20%), 3 (20%) |
| Laboratory finding | |
| Leukocytes (× 103/μL), mean, (SD) | 6.9 (3.6) |
| Hemoglobin (gm/dl), mean, (SD) | 12.4 (1) |
| Platelets (× 103/μL), mean, (SD) | 329.1 (159) |
| ALT (IU/L), mean, (SD) | 46 (19.5) |
| AST (IU/L), mean, (SD) | 42.5 (14.1) |
| Creatinine (mg/dL), mean (SD) | 1.1 (0.2) |
| CRP (mg/L), mean (SD) | 4 (1.3) |
| ESR (ml/hr), mean (SD) | 16.1 (8.6) |
| Widal test positivity cutoff 1/160 | 13 (86%) |
| Bacteria isolated from stool culture | |
| S. typhi | 10 (66%) |
| S. para-typhi A | 5 (33%) |
| S. para-typhi B/C | 0 (0%) |
| Time since the diagnosis of typhoid fever | |
| Chronic > 1 year | 5 (33%) |
| Temporarily 3 months-1 year | 8 (53%) |
| Convalescent 3 weeks-3 months | 1 (6%) |
Table 1: Basic, clinical, laboratory, radiological and microbiological data.
Exclusion criteria
• Past or family history of any psychiatric illness.
• Any form of drug addiction.
• Patients taking any psychotropic medications, including steroids (except for inhaled steroid), anti-depressant, anxiolytics and interferon treatment.
• Hypothyroidism, hypopituitarism, Cushing syndrome and hypocorticolism.
• Chronic kidney disease, liver failure, heart failure and respiratory failure.
• Active infections.
• Inflammatory collagen diseases.
• Malignancies.
• Pregnancy.
Clinical and investigational workup don for exclusion of organic diseases
Patients were subjected to full clinical assessment including history taking and thorough clinical examinations, supplemented by targeted laboratory, radiological and endoscopic assessment. Routine laboratory investigations were done supplemented as appropriate by more targeted investigations including complete blood count (CBC), liver functions, urinalysis, renal functions, blood sugar, electrolytes, thyroid function, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), anti-nuclear antibodies (ANA), calcium (Ca), serum protein electrophoresis, abdominal ultrasound, chest X-ray, echocardiography, resting and stress electrocardiography (ECG), computerized tomography (CT) abdomen and pelvis, upper and lower gastrointestinal (GIT) endoscopy. Clinical evaluation was done at the relevant specialized clinics at Al-Hussein university hospital, Cairo, Egypt and it was a routine work done while the evaluating physicians were not aware about the on-going study. Only after exclusion of organic causes were the patients enrolled. The medical records of the patients were reviewed, and the basic laboratory and radiological data were extracted and the positive clinical findings were recorded.
Case definition for typhoid carrier
• Typhoid carrier was defined as follow:
• No history of fever in the past 3 weeks and the body temperature was documented to be <37.5°C for >48 hours without antipyretics and the recoding done after inpatient admission.
• The history of enteric fever, diagnosed by appropriate culturing from blood, urine, stool or bone marrow was documented by reviewing the Patients’ medical records.
• At least one occasion of isolation of Salmonella typhi or Salmonella Para-typhi A, B or C from the stool of patients without fever.
• Throughout this article we did not differentiate between carriage of Salmonella typhi or Salmonella Para-typhi A, B or C, and we refer to all as typhoid carrier.
• All patients fulfilled all the above criteria.
Case identification of depression
The patients were evaluated using the standard clinical interview. The interview was conducted by an expert physician, under standard condition of optimum doctor-patient relationships. We used Hamilton Rating Scale for Depression (HAM-D) [20], which is a well validated questionnaire designed for assessing depression in adults. It uses some probing questions to assess the severity of depression; mood, guilty sensation, anxiety, weight loss, agitation, insomnia, somatic symptoms and suicidal ideation. The assessment is based on 17 items and each item is scored on 3 or 5 points. It is interpreted as follow:
• 0 - 7 = Normal
• 8 - 13 = Mild Depression
• 14-18 = Moderate Depression
• 19 - 22 = Severe Depression
• > 23 = Very severe depression
The score was recorded, for every patient, 3 times; on first assessment, at the end of antibiotics and 6 weeks after completion of antibiotics.
Consent and ethics
The study was approved by our local ethical committee. We obtained an informed, written consents from all patients.
Microbiological tests
Bacterial isolates from stool cultures were identified using the API 20E system (bioMérieux, Marcy l’Etoile, France).
Treatment and follow-up
After enrolment, we treated all patients empirically with intravenous ceftriaxone, 2 gram every 24 hours, for 14 days. No psychotropic drugs were given, only ceftriaxone. We adopted this protocol for all patients due to the high prevalence of ciprofloxacin resistant strains in Egypt (based on our clinical experiences).
Documenting recovery of carrier states
We documented clearance of carriage state through obtaining culture negative stool in 3 consecutive samples, taken 1 month after completion of antibiotic course, interestingly all patients showed stool culture negativity in the three samples.
Statistical analyses
All results were analysed using the Statistical Package for the Social Sciences (SPSS) program, version 23. Numerical data was expressed as mean ± standard deviation (SD) while categorical data was expressed as percentages. The Kolmogorov-Smirnov test was used to assess the normality of numerical data. Differences between two groups were compared using the Student's t-test for continuous variables, and the χ2 test or Fisher's exact test for categorical variables, as appropriate. Two pair t-test was applied to determine the mean differences and the significance of the HAM-D scale at different points of assessment. A pvalue of <0.05 was considered a statistically significant difference and p-value of <0.01 was considered highly a statistically significant difference
Basic characteristics of the cases
Typhoid carrier status was diagnosed in 15 patients, 8 males (53%) and 7 females (47%), the median age was 47 and the age range was 19-63 years. All patients were Egyptians and were referred to us from rural/villages area. Ten patients (66%) were not complaining of any chronic diseases while 3 (20%) were having DM, 4 (26%) were having HTN and 1 (6%) was suffering from bronchial asthma. As regarding smoking, six patients were smoker (40%) while 60% were not.
Clinical examination and imaging findings
Pallor and white coated tongue (Figure 1) were present in 12 patients (80%); right iliac fossa tenderness by deep palpation, using more than average pressure by overlapping hands was present in 13 (86%); mild splenomegaly (12-15 cm) in 8 (53%); hepatomegaly in 6 (40%); thick wall gall bladder in 12 (80%) and calculary gall bladder in 3 (20%). Repeated assessment at 6th week post antibiotic completion showed that pallor was present in 3 patients (20%); white coated tongue (Figure 1) in 2 (13%); right iliac fossa tenderness in 1 patient (6%); mild splenomegaly in 4 (26%); hepatomegaly in 6 (40%); thick wall gall bladder in 12 (80%) and calculary gall bladder in 3 (20%).
Figure 1: White coated tongue.
Laboratory findings
The mean of leukocyte was 6.9 × 103/μL) and the standard deviation (SD) was (3.6). The mean of haemoglobin was 12.4 gm/dl and the SD was (1). The mean platelet count was 329.1× 103/μL) and the SD was (159). The mean of ALT was 46 (IU/ml) and the SD was (19.5). The mean of AST was 42.5 (IU/ml) and the SD was (14.1). The mean of serum creatinine was 1.1 (mg/dL) and the SD was (0.2). The mean of CRP was 4 mg/L and the SD was 1.3. The mean of ESR was 16.1 ml/hr. and the SD was 8.6. Widal test was positive in 13 patients (86%). We used a cut-off value of 1/160 for either “O” or “H” antigen as positive Widal test.
Bacterial isolates
This was the most time-consuming factor in our study, as the excretion of Salmonella in typhoid carriers are intermittent and accordingly the possibility of catching it from one sample is considerably low, accordingly this limits the number of patients enrolled and prolong the study time to > 2 years. However, in our routine practice we decided to depend on clinical assessment supplemented by Widal test positivity to initiate antibiotic treatment, even in stool culture negative patients, yet without reporting our finding for reliability issue, see discussion section. Salmonella typhi was isolated in 10 patients (66%) and Salmonella Para-typhi A in 5 patients (33%). No isolate for S. para-typhi B/C was found.
Duration of carriage
We didn’t classify our patients based on carriage time (see discussion section), however our series was composed of 5 patients (33%) with chronic carriage > 1 year; 8 patients (53%) with temporarily, 3 months-1 year and 1 patient (6%) with Convalescent, 3 weeks-3 months. Table 1 shows basic, clinical, laboratory, radiological and microbiological data.
Presenting somatic complaints
Table 2 shows the frequency of somatic complaints at presentation and at 6th week post antibiotic completion. The changes in the presenting somatic complaints were highly statistically significant pvalue< 0.01. It shows that fatigue and myalgia were present in 15 (100%) patient, anorexia in 12 (80%), chronic abdominal pain in 11 (73%), change in bowel habits in 13 (86%), vomiting in 6 (40%), myalgia in 7 (46%), atypical chest pain in 4 (26), palpitations in 9 (60%), dyspnea in 8 (53%),urinary frequency in 6 (40%), erectile dysfunction in 4 out of 8 males (50%), while menstrual disturbance was present in 3 out of 7 females (42%). At the 6th week point the figures and percentages were 1 (6%), 3 (20%), 4 (26%), 7 (46%), 6 (40%), 0 (0%), 0 (0%), 1 (6%), 2 (13%), 1 (6%), 3 (20%), 1 (6%) and unapplicable, respectively. By un-applicability we mean that we reevaluated the patients after 6 weeks which is too short time for assessing menstruation.
| Symptoms | Before | At 6th week point | p-value |
|---|---|---|---|
| Fatigue | 15 (100%) | 1 (6%) | <0.001* |
| Headache | 15 (100%) | 3 (20%) | <0.001* |
| Anorexia | 12 (80%) | 4 (26%) | <0.001* |
| Change in bowel habits | 13 (86%) | 7 (46%) | <0.001* |
| Chronic/recurrent abdominal pain | 11 (73%) | 6 (40%) | <0.001* |
| Vomiting | 6 (40%) | 0 (0%) | <0.001* |
| Myalgia | 7 (46%) | 0 (0%) | <0.001* |
| Atypical chest pain | 4 (26%) | 1 (6%) | <0.001* |
| Palpitations | 9 (60%) | 2 (13%) | <0.001* |
| Dyspnea | 8 (53%) | 1 (6%) | <0.001* |
| Urinary frequency/dysuria | 6 (40%) | 3 (20%) | <0.001* |
| Erectile dysfunctions | 4 (50%) | 1 (6%) | <0.01* |
| Menstrual disturbances | 3 (42%) | UA | - |
Table 2: Frequency of somatic complaints at presentation and 6 weeks post-treatment. p-value <0.01* is considered as statistically highly significant.
Hamilton-D (HAM-D) scale changes with antibiotic treatment
Figure 2 shows the classification of depression, based on Ham-D scale at the presentation, 2 weeks and 6th week points.
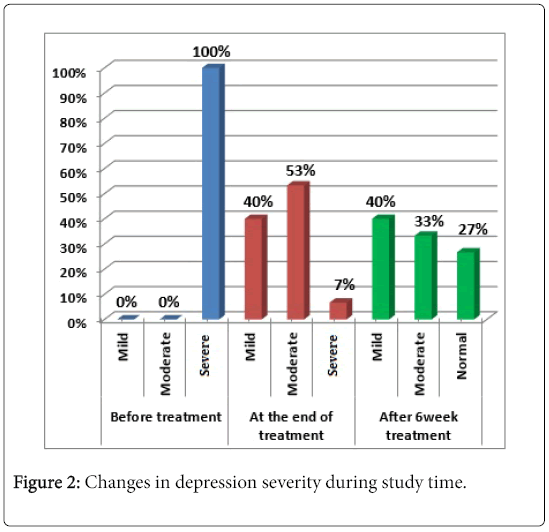
Figure 2: Changes in depression severity during study time.
At presentation, all patients were having severe depression; while at the end of antibiotic treatment only 1 patient (7%) still was having severe depression, 8 patients (53%) were having moderate depression and mild depression was present in 6 patients (40%). By the 6th week post treatment completion, no patients were having severe depression, 5 patients (33%) showed moderate depression, 6 patients (40%) exhibited mild depression and 4 patients (27%) were normal.
Table 3 and Figure 3 shows the changes in the means of HAM-D scale with treatment; which signified statistically significant differences of the mean of HAM-D scale at the 3 points of evaluations, pvalue< 0.01 for each pair.
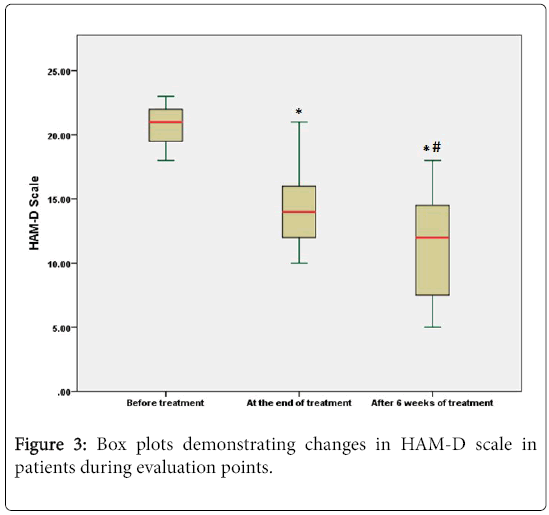
Figure 3: Box plots demonstrating changes in HAM-D scale in patients during evaluation points.
| Variables | Minimum | Maximum | Mean | Std. Deviation | Paired Samples t-test | p-value | |
|---|---|---|---|---|---|---|---|
| t | df | ||||||
| HAM-D before treatment | 18 | 23 | 20.8 | 1.61245 | 7.267 | 14 | <0.001* |
| HAM-D at end of treatment | 10 | 21 | 14.2667 | 3.08143 | 8.119 | 14 | <0.001** |
| HAM-D at 6th week post treatment completion | 5 | 18 | 11.2 | 4.00357 | 4.258 | 14 | <0.001*** |
| * for comparing HAM-D before treatment and at the end of treatment; ** for comparing HAM-D before treatment and at the end of treatment; *** for comparing HAM-D at the end of treatment and at 6th week post treatment completion. | |||||||
Table 3: Changes in HAM-D scale with treatment.
To the best of our knowledge, this is the first report about the association between typhoid carriage and low mood. Our report showed that all cases with typhoid carrier states were presented by severe depression, based on HAM-D scale, with very statistically significant improvement in their depression scale, solely after antibiotic treatment. The improvement in depression scale was evident immediately after completion of antibiotic courses and consolidates at the 6th-week post antibiotic completion point of evaluation. It also shows that the improvement of the presenting somatic complaints was statistically very significant (Table 2).
This series reporting is inconsistent with most of the previous reports, which acknowledge that most of typhoid carriers in endemic areas are asymptomatic and up to 25% of them have no history of typhoid fever [21,22].
Previous studies dealing with typhoid carrier tried to separate between convalescent, temporary and chronic carriers. Convalescent carriers excrete the bacterium in feces for three weeks to three months post-infection, temporary excrete for between three and twelve months, and chronic for more than one year [22]. This separation is mainly for epidemiological interest; however, we didn’t think that this distinction would be of clinical interest in term of depression, as all categories in our series presented and responded similarly.
We didn’t include Widal test in our criteria for enrolment, because of the unreliability and non-validity of it; however it still represents a very important clinical tool in diagnosis of acute typhoid fever in developing countries, like Egypt [23]. If we had included it, the number of cases reported in this series would be multiplied many times, because it is widely used in diagnosis of typhoid fever in our country, and we faced many patients with clinical history of typhoid fever, yet their diagnosis was based only on the positivity of Widal test, without confirmation by culturing the bacterium. Also, many patients were having a clear history of typhoid fever that was diagnosed by culturing, yet we failed to find Salmonella organisms in stool culture at the enrolment time, accordingly failed to prove their carrier states. Those patients were excluded from reporting, however we treated them in the same manner, and they responded in same way.
Many typhoid carriers are excretory only of S. typhi [24], however the bacteria isolated in our series was S. typhi in 10 patients and paratyphi- A in 5 patients, representing about 66% and 33%, respectively. This isn’t a real paradox, because S. para-typhi was also isolated from the gall bladder of Nepali patients [25]. Abnormal gall bladder in imaging was prevalent in our series with thick wall gall bladder present in 12 (80%) and calcular gall bladder in 3 (20%). This is consistent with previous reports [26-28]. White coated tongue was found to be highly specific for acute enteric fever in a study by Haq et al. [29] in our study it was found in 80% of patients in spite of being afebrile. Right iliac fossa tenderness and mesenteric adenitis or even appendicitis, are known to be a presenting feature of enteric fever [30-33].
In our series, right iliac fossa tenderness by deep palpation using more than average pressure by overlapping hands was found in 13 (86%) of patients. The tenderness elicited wasn’t associated with any peritoneal irritation signs. We incriminate the ileum as a site for carriage which results in local inflammation and tenderness. Likewise, the mild splenomegaly (12-15 cm) presented in 53% of our patients, best explained by the local chronic inflammation in terminal ileum. Depression is a heterogenous disorder with multiple psychosocial, immunological, infectious and biological risk factors.
The role of inflammation in depression has been extensively studied over the past decades. Peripheral blood and cerebrospinal fluid (CSF) of patients with major depressive illness, were found to have increasing expression of inflammatory cytokines, their receptors, acute phase reactants and soluble cell adhesion molecules [10,34,35]. There are clear evidences from meta-analysis about the association of peripheral blood level of IL-1β, IL-6, TNF and C-reactive protein (CRP) with depression [10]. Polymorphisms in the genes of the inflammatory cytokines; IL-1β, TNF and CRP were associated with depression and its response to treatment [36]. Patients treated with the inflammatory cytokine; interferon-α, developed clinically significant depression [13,14]. Likewise, patients treated anti-TNF, including rheumatoid arthritis, psoriasis and cancer showed improvement in their depression symptoms [37-39]. Patients with treatment-resistant depression whom were having high levels of inflammatory markers responded to anti- TNF with improvement in their depression severity [40]. Also, uncontrolled inflammation has been associated in many studies, with poor response to anti-depressants [41-43].
One model explaining the association between inflammation and depression is the “Pathogen host defense theory”, according to it the strong selective pressure by microbial exposure, promoted selection of pro-inflammatory alleles, which in turn are associated with initiation of depressive behaviors. The negative depressive behaviors; the social avoidance and anhedonia characteristic of depression, aren’t considered bystanders, rather protective through shunting energy sources towards combating infections [42,44].
Many infectious agents have been suspected as risk factors for depression, including enterovirus, human immunodeficiency virus, hepatitis C virus, varicella-zoster virus, human T-cell lymphotropic virus, herpes simplex 1, Epstein-Barr virus, Borna disease virus, Brucellosis and Chlamydophila trachomatis [45-52]. Typhoid fever is well known to be associated with depression and this was documented in previous reports [15-17].
Recently, typhoid vaccine was used in experimental models for induction of inflammatory states associated with low mood [18,19]. This evolving association between typhoid vaccine using only a single subcutaneous polysaccharide antigen, puts strong criticisms in the asymptomatic model of Salmonella carriers, when the subjects excrete Salmonella intermittently for prolonged ill-defined period. Our series criticize this asymptomatic model. We showed that all 15 patients with documented typhoid carrier states were suffering from low mood associated with somatic complaints, and this improved after documenting the clearance of carrier states. One can look to our results as a support for the growing theory of approaching depression; “the leaky gut hypothesis” which assumes that infection of intestinal epithelium by gram negative bacteria makes the intestinal epithelium leaky to the inflammatory cytokines that promote depression. In supporting of this, is the finding of an elevated serum IgM and IgA against lipopolysaccharides (LPS) of the gram negative enterobacteria in depressed patients [52,53].
Likewise, the leaky gut was implicated in pathogenesis and clinical severity of schizophrenia, and this was thought to be mediated by the inflammatory cytokines [54-57].
We postulate that the intermittent excretion of Salmonella bacteria by the typhoid carrier patients result local intestinal inflammatory reactions that damage the epithelium allowing the inflammatory cytokines to translocate. It is the inflammatory cytokines that results in depression. However, we didn’t measure the inflammatory cytokines in our series, and this is a limiting factor in our finding. We recommend further studies measuring the inflammatory cytokines in typhoid carriers and correlating it with low mood before and after clearance of the carrier states.
Instead of the traditional asymptomatic view for typhoid carrier state, we present “the chronic infection model”; the patients are chronically infected, yet afebrile and the chronic infection is reflected as “psycho-somatic depression”. Other limitations of our study are the relatively small number of the patients and the relatively short time of follow-up. We recommend further studies using large number and following the patients for prolonged durations. We acknowledge that our results are inconsistent with the traditional view for typhoid carriers as asymptomatic populations, and we don’t expect this view to be changed based on a series of 15 patients; however, we encourage physicians in endemic countries to report similar associations.
Finally, during our work we were faced by the fact that diagnosis of Salmonella carriers is difficult due to the intermittent nature of excretions and especially in developing countries where the accessibility for accurate stool cultures is restrained and the unreliability of the widely available Widal test. We encourage further tests development for detections of Salmonella carriers.
The authors declare that there is no conflict of interest regarding the publication of this paper
We did not receive any fund.
All data are available upon request.