Journal of Depression and Anxiety
Open Access
ISSN: 2167-1044
ISSN: 2167-1044
Research Article - (2016) Volume 5, Issue 1
Background: To investigate the comorbidity of functional gastrointestinal disorders (FGIDs) in current major depressive disorder (MDD) patients.
Method: The prevalence of gastrointestinal symptoms and the comorbidity of FGIDs were studied in a set of consecutively enrolled current MDD patients in a general hospital psychiatric outpatient clinic from Mar, 17th, 2011 to Dec, 31st, 2011. A total of consenting 62 patients were included. MDD diagnosis was made by experienced psychiatrists according to Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria. FGIDs diagnosis was based on Rome III diagnostic questionnaire and approved by gastroenterologists.
Result: In this group, 58 (93.5%) reported gastrointestinal symptom, the most prevalent symptom is abdominal pain or bloating or discomfort (87.1%), followed by diarrhea or constipation (85.5%), decreased or increased appetite (83.9%), reduced or increased food intake (83.9%), burp or belching (77.4%), nausea or vomiting (46.8%). Forty-six of the total 62 patients (74.2%) met the criteria of one or more FGIDs. In these 46 patients, 30 (65.2%) patients have overlap syndrome (two or more FGIDs). Functional dyspepsia (FD) is the most prevalent (54.8%), then belching disorder (29.0%), functional heartburn (16.1%), unspecified functional bowel disorder (16.1%) and irritable bowel syndrome (12.9%).
Conclusion: In current MDD patients, gastrointestinal symptoms are common and a large percentage of them can already be diagnosed as FGIDs comorbidity, which demands clinical attention and future research.
Keywords: Functional gastrointestinal disorders; Comorbidity; Major depressive disorder; Rome criteria
Depression is commonly associated with physical symptoms involving many body systems, such as sexual symptoms, fatigue, insomnia, changes in appetite (which are included in diagnostic criteria) and many other symptoms [1]. These symptoms also cause great burden to patients and sometimes may be the presenting symptom to clinic [2]. Gastrointestinal symptoms other than appetite change are also very common in depressive patients [3]. In psychiatric tradition, these gastrointestinal symptoms are often seen as functional symptoms caused by depression.
In gastroenterology, chronic and recurrent gastrointestinal symptoms without organic causes are diagnosed as FGIDs by Rome classification. They are also very common in general population [4]. A study in health examination Chinese subjects found that the prevalence of functional dyspepsia (FD), irritable bowel syndrome (IBS), functional bloating and functional constipation were 19.8%, 8.3%, 11.0% and 10.1% respectively [5]. FGIDs have been extensively researched in gastroenterology. Psychological factors are thought to play a role in FGIDs through “brain-gut interactions”. Previous studies found a high depression level in FGID patients, and depression is considered an important predictor of FD and IBS [6-8]. In a hospital based study in outpatient with IBS and FD in comprehensive hospitals in big cities in China, the prevalence of depressive symptom in FD and IBS were 13.5% and 13.8% respectively, less than 12% of depressive subjects had been recognized and treated [9]. The depression in FGID patients was obviously overlooked.
How is the situation in psychiatry specialty? A case-control study compared MDD patients seeking treatment in an outpatient setting to a control group of patients seeking treatment in a general physician’s office for other medical illnesses. Twenty-seven percent of MDD patients met criteria for IBS in contrast to 2.5% of the control group [10]. In the limited studies seeing these gastrointestinal symptoms as FGIDs, most studies focused on IBS and FD [6-10]. But gastrointestinal symptoms are much wider than these. This study will assess the FGIDs comorbidity and its distribution pattern in current MDD patients, as this narrower set of depressive patients should be more homogenous.
Study population
This consecutive study was carried out in the outpatient clinic of psychological medicine department, Peking Union Medical College Hospital (PUMCH) from March, 17th, 2011 to December, 31st, 2011. Current MDD patients who sought help for the first time were referred by psychiatrists of Psychological Medicine Department to this study. Among these patients, some may have been to other department first for complaints of bodily discomforts and then came to psychological medicine clinic. Those then who provided formal consent are included.
Inclusion criteria: (1) 18 years old or above; (2) clinically diagnosed by experienced psychiatrists as MDD currently in a depressive episode according to DSM-IV; (3) formal consent.
Exclusion criteria: (1) malignant cancer history; (2) current pregnancy; (3) current comorbidity of serious medical conditions; (4) unable to cooperate; (5) organic diseases that can explain the gastrointestinal symptoms (done by referral to gastroenterologists).
Study procedure
Ninety-six were referred and 73 of them agreed to participate in study, with a response rate of 76.0% (73/96). Those who didn’t participate are with following reasons: no time (7), lost contact (6), not willing to receive gastrointestinal evaluation tests (4), deny depression diagnosis (2), hearing or communicating difficulty (2), objection from family members (2). Sixty-two patients completed the study; 11 patients dropped out for reason of “time inconvenience”, with a drop-out rate of 15.1% (11/73). Flowchart of participants is shown in Figure 1.
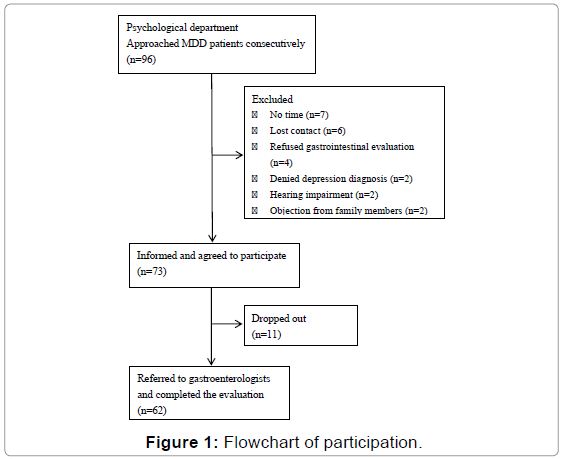
Figure 1: Flowchart of participation.
Trained investigators made a face to face interview with patients to collect demographic data and physical symptom information and help patient complete Rome III diagnostic questionnaire. One qualified clinical psychologist made Hamilton Depression Scale (HAMD- 17), Montgomery–Asberg Depression Rating Scale (MADRS) and the Hamilton Anxiety Scale (HAMA) evaluations. Then patients were referred to gastroenterologists. Generally it is in 3 days to 1 week. Gastroenterologists may arrange further diagnostic tests or examinations based on their clinical judgment. Thirty-six patients finished necessary gastrointestinal laboratory test, although 1 of them was diagnosed as inflammatory bowel disease and 3 was diagnosed as gastroesophageal reflux disease, the gastrointestinal symptoms could not be explained by those diseases. The medical records of the other 26 patients were reviewed by gastroenterologist to rule out organic problems. All the FGIDs diagnosis were finally reviewed and approved by gastroenterologists.
The procedure and consent are approved by Peking Union Medical College Hospital ethic committee.
Adult FGID Rome III diagnostic questionnaire
Rome III diagnostic questionnaire is designed for research by Rome committee based on FGID Rome III criteria. It covers all major domains of adult functional gastrointestinal disorders from Category A to Category F in Rome III. Category A is Functional esophageal disorders, B is Functional gastroduodenal disorders, C is Functional bowel disorders, D is Functional abdominal pain syndrome, E is Functional gallbladder disorder, and F is Functional anorectal disorders. This questionnaire is designed for research, it can also be used to help make clinical diagnosis [11]. The questions were designed to be read by the patients themselves, but read by investigators in this study to make sure the patients can understand and answer every question.
Physical symptoms list
This list covers 5 aspects: sleep (8 symptoms), fatigue (4 symptoms), gastrointestinal function (6 symptoms), pain (3 symptoms), sexual function (5 symptoms). Gastrointestinal function symptoms are: decrease or increase in appetite, decrease or increase in food intake, abdominal discomfort or pain or bloat, burp or belching, nausea or vomiting, diarrhea or constipation. The respective aspect would be considered as positive when any one symptom exists.
Hamilton Depression Scale (HAMD-17), Montgomery– Asberg Depression Rating Scale (MADRS) and the Hamilton Anxiety Scale (HAMA)
The severity of depression and anxiety of all the patients was assessed based on a semi-structured clinical interview, the Hamilton Depression Scale (HAMD-17), Montgomery–Asberg Depression Rating Scale (MADRS) and the Hamilton Anxiety Scale (HAMA) [12,14,16]. The Chinese versions of these questionnaires have been proved of having good reliability and validity in China [13,15,17].
Inter-rater-reliability
Hamilton Depression Scale (HAMD-17), Hamilton Anxiety Scale (HAMA) and Montgomery–Asberg Depression Rating Scale (MADRS) were done by one single qualified clinical psychologist in this study.
Data analysis
The EpiData 3.1 software was used to input data, SAS (version 9.2) to perform the diagnostic analysis of the diagnostic questionnaire of Rome III for FGIDs, SPSS for Windows (version 17.0) to finish statistical analysis. The statistical description: continuous variables conforming to the normal distribution are described in the form of mean ± standard deviation (SD); the categorical variables are described in rate.
Definition of overlap syndrome in this study is: meeting diagnoses from more than two different categories (Category A to Category F) in Rome III.
Of the total 62 patients, 64.5% (40/62) were female. The mean age was 42.9 years old (Table 1). It should be noted that 16 patients came to psychiatric clinic after they went to see gastroenterologists first, 15 of these patients were also enrolled in a clinical study of functional dyspepsia and mental disorder co-morbidity [7]. There was no significant difference between these 16 patients and other patients regarding their demographic characteristics, even though patients referred from the gastroenterologists had lower BMI and MADRS score than the rest (Supplementary Table 1) (Table 1).
| Total (n=62) | |
|---|---|
| Gender n(%) | |
| Male | 22(35.5) |
| Female | 40(64.5) |
| Marriage status n(%) | |
| Married | 41(66.1) |
| No spouse | 21(33.9) |
| Educational Level n(%) | |
| Primary school or below | 7(11.3) |
| High school | 41(66.1) |
| College degree and above | 14 (22.6) |
| Occupationn(%) | |
| Inoccupation | 15(24.2) |
| Have the occupation | 40(64.5) |
| Lack of information | 7(11.3) |
| Living Placen(%) | |
| Urban | 42(67.7) |
| Small town | 12(19.4) |
| Rural area | 8(12.9) |
| Income per family membern(%) | |
| Lower than RMB 2000 | 14(23.0) |
| Higher than RMB 2000 | 47(77.0) |
| Age(mean±SD) | 42.9 ±14.3 |
| BMI(mean±SD) | 22.4±3.9 |
| HAMD(mean±SD) | 23.6 ±6.8 |
| MADRS(mean±SD) | 23.9 ±8.6 |
| HAMA(mean±SD) | 22.8 ±7.7 |
Note: BMI, body mass index; HAMD-17,the Hamilton Depression Scale-17 items; MADRS, Montgomery–Asberg Depression Rating Scale; HAMA, the Hamilton Anxiety Scale (HAMA).
Table 1: Demographic and clinical characteristics.
Physical symptoms
In the total of 62 current MDD patients, 58 (93.5%) of them reported at least one gastrointestinal symptom. The most prevalent gastrointestinal symptom is abdominal pain or bloating or discomfort (87.1%), followed by diarrhea or constipation (85.5%), decreased or increased appetite (83.9%), reduced or increased food intake (83.9%), burp or belching (77.4%), nausea or vomiting (46.8%). Physical symptoms of these MDD patients are shown in Table 2.
| Yes/N | % | |
|---|---|---|
| Sleep | 58/62 | 93.5 |
| Fatigue | 56/62 | 90.3 |
| Sexual function | 50/62 | 80.6 |
| Pain | 46/62 | 74.2 |
| Gastrointestinal symptoms | 58/62 | 93.5 |
| Decreased or increased appetite | 48/58 | 83.9 |
| Reduced or increased food | 48/58 | 83.9 |
| Abdominal pain or bloating or discomfort | 50/58 | 87.1 |
| Burp or belching | 44/58 | 77.4 |
| Nausea or vomiting | 25/58 | 46.8 |
| Diarrhea or constipation | 49/49 | 85.5 |
Table 2: Somatic symptoms in MDD patients.
FGIDs diagnosis
Forty-six out of 62 (74.2%) patients met at least one FGID diagnosis. The prevalence of FGIDs in MDD patients are: FD (54.8%), Belching disorder (29.0%), Functional heartburn (16.1%), unspecified functional bowel disorder (16.1%) and IBS (12.9%).
Thirty of them (65.2%) met 2 or more FGID diagnoses from different categories, which defined as overlap syndrome. The spectra of FGIDs are displayed in Table 3.
| FGID | Yes | % | Overlap with other FGID(s) | % in Subgroup of FGID |
|---|---|---|---|---|
| A.Functional esophageal disorders | 14 | 22.6 | 12 | 85.7 |
| A1.Functional heartburn | 10 | 16.1 | ||
| A2.Functional chest pain of presumed esophageal origin | 4 | 6.5 | ||
| A3.Functional dysphagia | 1 | 1.6 | ||
| A4.Globus | 1 | 1.6 | ||
| B.Functional gastroduodenal disorders | 37 | 59.7 | 27 | 73.0 |
| B1.Functional dyspepsia | 34 | 54.8 | ||
| B1a.Postprandial Distress Syndrome | 29 | 46.8 | ||
| B1b.Epigastric Pain Syndrome | 1 | 1.6 | ||
| B2. Belching | 18 | 29.0 | ||
| B2a.Aeropgagia | NA | NA | ||
| B2b.Unspecified Excessive Belching | NA | NA | ||
| B3.Nausea and vomiting disorders | 6 | 9.7 | ||
| B3a.Chronic Idiopathic Nausea | 3 | 4.8 | ||
| B3b.Functional vomiting | 3 | 4.8 | ||
| B3c. Cyclic Vomiting Syndrome | 2 | 3.2 | ||
| B4.Rumination Syndrome | 0 | 0 | ||
| C.Functional bowel disorders | 27 | 43.5 | 23 | 85.2 |
| C1.Irritable bowel syndrome | 8 | 12.9 | ||
| C2.Functional Bloating | 3 | 4.8 | ||
| C3.Functional Constipation | 4 | 6.5 | ||
| C4.Functional Diarrhea | 2 | 3.2 | ||
| C5.Unspecified Functional Bowel Disorder | 10 | 16.1 | ||
| D.Functional Abdominal Pain Syndrome | 1 | 1.6 | 1 | 100 |
| E.Functional Gallbladder Disorder | 0 | 0 | 0 | - |
| F.Functional anorectal disorders | 10 | 16.1 | 10 | 100 |
| F1.Functional Fecal Incontinence contingen | 2 | 3.2 | ||
| F2. Functional anorectal pain | 5 | 8.1 | ||
| F2a.Chronic proctalgia | 2 | 3.2 | ||
| F2b.ProctalgiaFugax | 3 | 4.8 | ||
| F3.Functional Defecation Disorders | 4 | 6.5 |
Note: NA, not available according to Rome III questionnaire
Table 3: FGIDs diagnosis in MDD patients.
The brain-gut bi-direction modulation hypothesis has been more and more recognized in past few years. Most studies were done by gastroenterologists from the gut-brain direction showing that in FGID patients there is high prevalence of depression and anxiety [5-9,18]. There are also studies from the other direction showing that gastrointestinal symptoms are very frequent and variant in depressive and anxious patients [1-3]. Most of them were descriptive studies in which depressive and gastrointestinal symptoms were analyzed in terms of severity or frequency based on questionnaire scores [1-3,5-9,19]. Depressive symptoms may indicate but do not mean depressive disorder. If the target population is defined at disorder level, a better homogeneity can be achieved. Our study is the first study as we know to use Rome III diagnostic questionnaire to study FGID distribution in clinically diagnosed current MDD patients.
Gastrointestinal symptom was reported by over 90% MDD patients in this study. It is shown that, clinical meaningful or not, gastrointestinal symptoms are extraordinarily common and have a wide spectrum in this group of MDD patients.
Based on Rome III diagnostic questionnaire, 74.2% of the current MDD patients can be diagnosed with at least one functional gastrointestinal disorder. FGIDs are often recurrent or chronic and cause significant impairment to health quality of life (HQOL) of patients [4,20-22]. Our result indicates that FGID are very common in MDD patients, so it is important for clinical psychiatrist to recognize FGID in MDD patients and make proper further evaluation, explanation and treatment if necessary.
In those who are diagnosed with FGID, 65.2% have overlap syndrome which means more than one FGID. Previous studies found that overlap syndrome is often associated with worse HQOL and high depression and anxiety level than those having a single FGID [6,21]. The prevalence of overlap in FGIDs based on Rome criteria was 42.6% - 51.4% in hospital samples [23,24]. Rate of overlap is even higher in this study. This phenomenon could be understood theoretically in two ways: on one hand, depressive disorder as a psychological stress raise the brain-gut action resulting in more gastrointestinal dysfunctions; on the other hand, overlap syndrome enhances the gut-brain effect to increase MDD. Further longitudinal studies of overlap syndrome are necessary to answer this question.
In gastroenterological studies, the most frequent FGIDs were reported as following: FD (46.0%), IBS (40.2%), Belching disorder (30.7%), Functional heartburn (14.6%) [23]. In our study, the prevalence of FD is higher and that of IBS is lower than in gastroenterological clinic. FD and IBS were the most intensively studied entities among FGIDs. In general Chinese population, FD (5.3%-19.8%) is more frequent than IBS (4.1%-8.3%). In our study, FD prevalence (54.8%) is significantly higher than IBS (12.9%) [5,25,26]. It is different from the result in other population. A Korean study also showed a stronger relevance of FD than IBS to depressive symptoms [6]. In another cohort study, higher levels of anxiety and depression at baseline were predictive of IBS at follow-up, while only depression was predictive of FD at follow-up [8]. All these results support that there might be an inner mechanism connecting FD and MDD. Further studies, especially neurobiological studies are needed to explore this matter. Of course, selection bias could also be a reason for higher FD prevalence.
There are several limitations in this study. Firstly, the sample size is relatively small. Secondly, there is selection bias, as patients with gastrointestinal symptoms referred by Gastroenterologist or Traditional Chinese Medicine doctor or other physicians to psychiatric clinic are included in study design. These patients may have more frequent somatic symptoms, including gastrointestinal symptoms, with unknown organic origin. It has to be taken into consideration that this study is done in one center. PUMC hospital is a most renowned general hospital in China. Many patients came often because their health conditions are difficult or complex and were referred from all over China. The possibility of comorbidity in this group is supposedly higher. Moreover, the MDD patients without digestive symptoms seemed more likely to refuse our investigation. Thirdly, some patients (26/62) did not receive systemic gastrointestinal evaluation, although based on clinical history and basic examinations and tests, it was confident to rule out significant organic disease, but still there could potentially be organic causes. Another limitation is that in this study design the effect of medication was not considered. It is known in clinical practice that certain drugs, such as antidepressants, can cause constipation or bloating feelings in some patients. Although in most situations, it is not the main source of patients’ bodily discomfort in FGID.
In our explorative study, it is found that gastrointestinal symptoms are very prevalent in current MDD patients and a large percentage of them can be diagnosed as FGIDs. A unique pattern of FGID is also shown. FD prevalence is much higher than IBS. Could this indicate a closer relationship of depression with FD? Could this lead us to a better understanding of the brain-gut bi-direction mechanism? Many following questions could be asked, but no definite can be provided for now. We call for more clinical and scientific attention of psychiatrists to this important topic in the future.
This study is supported by the Capital Health Research and Development of Special (Grant No.2009-3003).