Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 1
Spiegel hernias are process of low incidence that represents less than 2% of abdominal hernias. Diagnosis is often complex and in some cases is purely casual discovery. In cases in which these are symptomatic is postural abdominal pain located it´s first expression. After the anamnesis facing possible predisposing factors such as trauma or the concurrence of processes involving increased abdominal pressure and palpation is the main diagnostic instrument. Ultrasound or tomographies are useful to diagnose when tenderness is not enough. The request for additional tests without a diagnosis or suspicion can result in false negatives that slow down the diagnostic process. Strangulation and subsequent surgical intervention was the reason that changes the diagnostic process after months of study and high direct and indirect costs. In recent years the approach by laparoscopic way has shown comparable performance and shorter hospital stay. Successful diagnostic and therapeutic action, by doctor the emergency room, helped the patient returning to work in just two weeks; recovering completely the quality of life that had before trauma. All pitting the immediate cessation of the frequentation of the health system and the removal of the stigma sometimes unavoidable in some of these cases be regarded as a “hyperfrequenter” both patient the urgent field as in primary care.
<Woman of thirty-two years old, unknown allergies. Uterine fibroids and two Caesarean sections, ask for abdominal pain in infraumbilical region, from 5 days of subsequent developments to trauma of moderate intensity and intermittent painful pace. Physical examination, stable constants, was evidence of abdominal defense so it refers to the emergency room. Diagnosed with urinary tract infection, antibiotic treatment is scheduled and proceeded to discharge. Two days later and despite treatment, continue the inconvenience partnering new symptoms: diarrhea, urinary frequency, urgency and bladder fullness. So she was sent again to the emergency room. Ultrasound was performed without further findings that uterine fibroid. Almost a week later, it was attended by the urologist’s guard who decided to high with ciprofloxacin, buscapina, metamizol and control in external consultation Urology in three weeks. Emergency empty bladder ultrasound, without alterations, impressed bladder pressure caused by fibroid uterus. Per month, picture continued, so that in emergencies was valued by the gynecologist who consults Urology by possible intravesical lesion after ultrasound. After uretrocistocopia without findings proceeded to discharge guideline anticholinergic (solifenacin succinate) and cranberry extract. A week later she turns to Urology who diagnosed possibly secondary neurogenic bladder problems from bone marrow and/or lumbar spine which derive to Neurology.
Two months later she joined in neurology, the electroneurograma and the bone scan of pelvis, hips and lumbar spine were normal; deriving to Rheumatology where was diagnosed with sacroiliitis grade II and dyssynergia vesico-sphincter of etiology unknown after eight days of hospital stay.
Three months later, her family doctor continued the study requesting stool culture, barium enema and computed tomography abdomino-pelvic resulting findings (Figure 1). Four months later, in the service of digestive was diagnosed of “peritoneal suffering caused by fibroid uterus”.
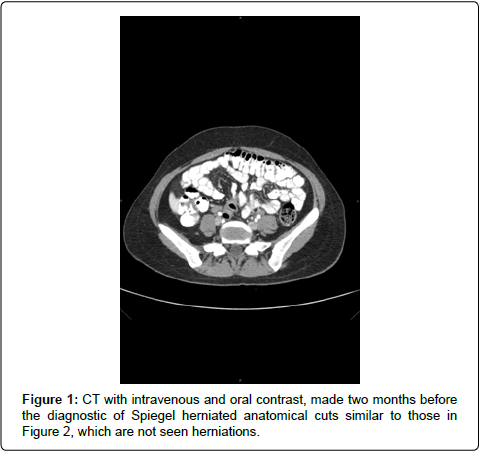
Figure 1: CT with intravenous and oral contrast, made two months before the diagnostic of Spiegel herniated anatomical cuts similar to those in Figure 2, which are not seen herniations.
Rheumatology service is called complementary tests whose results were negative. Although the picture didn’t end improve the patient requested high job within four months of the onset of symptoms, while continued with more outpatient complementary tests. With ten and a half months of evolution of their discomfort, pictures that are repeated, with short periods of temporary improvement it was decided to raise income for study. During her entry into internal medicine, are you practicing radiographs of thorax and abdomen, simple ultrasound and doppler abdomino-pelvic, gastroscopy, colonoscopy and abdominal CT without pathological findings. Requested consultation service of psychosomatic is found no where clinical to match a disorder chronic pain somatoform.
A year later, and persisting discomfort in new TAC requested by your primary care physician a Tarlov cyst met casually in S2 which subsequently by MRI was reported as cystic formation of the terminal cone without sacred impact as anatomical variant not pathological. In neurology after realization of potentials evoked no alterations were really pregabalin and indomethacin.
One year and one month after the onset of pain, and after a long journey by the various services the patient said new emergency assistance by increasing abdominal pain of hours of evolution. The presence of signs of peritoneal irritation by the ER doctor motivated was requested collaboration surgery diagnosed where simple manual examination of abdomen, with the presence of a possible Spigelian Hernia painful and care what motivated the realization of a hernioplasty laparoscopic emergency without application of any further evidence beyond of preoperative. Three days of the intervention was tomography control that target the correct implementation of the mesh (Figure 2) for which the patient was given high. Currently and after more than one year of evolution without recurrence, the patient has not raised any new consultation and is monitoring and control by your primary care physician. The patient was currently working; makes normal life and episodes of anxiety suffered by the variegated case have disappeared.
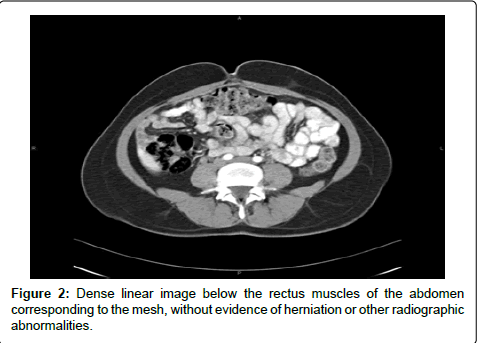
Figure 2: Dense linear image below the rectus muscles of the abdomen corresponding to the mesh, without evidence of herniation or other radiographic abnormalities.
Spiegel hernia is a rare disorder of the abdominal wall with risk of strangulation as the case described. Predisposing factors include trauma as the referred by the patient in your first query, or any increase in intra-abdominal pressure. They are more frequent from the 40 years, affect both sexes equally, and are often difficult to diagnosis by its location back to the muscle aponeurosis more oblique, which hinders its palpation in the hands little expert both its low frequency.
The base to support the diagnosis is starting from a clinical suspicion by performing a thorough anamnesis that orient toward the predisposing factors. The physical exam by abdominal palpation is not always easy on the basis of the sheer size of the hernia. In cases where tenderness is not clear is where the ultrasound and CT can help, proposing the ultrasound as gold Server [1], although both may be false-negative test.
Diagnostic of low clinical suspicion which indicates the test and the experience of the radiologist in the diagnosis of this type of pathologies may decrease the false negatives. In our case were nine ultrasounds, two CT scans, three resonances and a scan and none of the reports described the hernia. After review of the case, as a fundamental cause that has led us to explain this event noted that none of the applications of Imaging tests described nor reason for consultation, or background of the case, not even the location of the pain being only in the reason for request in nine requests “diffuse abdominal pain” to study.
It is therefore that this work intends to emphasize that although the complementary tests are necessary in many cases, should bear in mind, that your application not based on any kind of diagnostic suspicion can decrease significantly their diagnostic performance; and may finally provide false security of absence of pathology in the case of rare diseases, whose diagnosis requires certain clinical suspicion.
Treatment of Spigelian Hernia is surgical risk of complications that arouse these hernias. As it was the case in our patient, it is estimated that you between 21 and 33% involved emergency by strangulation or incarceracion [2] in part motivated by the previous diagnostic failure. There is no consensus on what is the best technique for repair of Spiegel [3] hernia surgery.
They can be repaired using techniques with voltage (without mesh) Although the majority of the authors perform techniques without tension, with mesh placed in the preperitoneal level, between the oblique muscles, or preformed meshes that allow the repair in two planes (preperitoneal and muscle). Typically the approach has been through the open, but in recent years, the technique was developed by via laparoscopic with comparable results and shorter hospital stay. Laparoscopic surgery appears as an alternative that requires experienced surgeons and a higher cost [4]. The repair of these hernias can be performed with local anesthesia, local and general and there are even multiple cases of outpatient surgery with a low rate of morbimortalidad [5]. It is therefore of vital importance to tackling the diseases of difficult diagnosis, beyond delve into the use of evidence diagnostic, is based on a multidisciplinary approach that coordinates the area of primary health care as the rest of hospital medical and surgical disciplines.