Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2014) Volume 1, Issue 3
Objectives: To describe trends in the use of a medicine information (MI) service located within a large teaching university hospital in order to enable a workload model to be developed.
Method: All MI enquiries within one large teaching hospital received in the same two months from 2006 to 2010 were reviewed to collect enquiry category, complexity level, origin, enquirer and time taken to process enquiry. Level 1 complexity enquiries required one reference source for completion, level 2 required the use of multiple and more specialist sources whilst level 3 require multiple sources and the evaluation of primary literature. Data was analysed descriptively to enable trends in MI queries to be identified. Multiple linear regression analysis was used to predict time taken to complete enquiries.
Results: 1605 MI enquiries were analysed. The total number of enquiries received during the 2 months from 2006 was 238 compared to 343 in 2010. 583(36.3%) of enquiries were due to administration of medicines, 211(13.1%) therapy choice and 204(12.7%) related to supply
Keywords: Medicines information; Drug information; Pharmacy; Evaluation; Workload
Medicines information (MI) services, first appearing in the USA in the 1960s and introduced in the UK in the 1970s, were set up with the primary objective of providing comprehensive, unbiased information regarding medicines to health care professionals and other users [1,2]. The driver for their development being the need to use evidence based medicine when making complex prescribing decisions in clinical settings where appropriate reference sources were not immediately available. Research repeatedly demonstrates high levels of user satisfaction with MI services [1-8] and the potential for providing positive patient outcomes as a result of information provided [7-9].
In addition to answering individual medicines-related enquiries MI centres have evolved to support local pharmacy and therapeutics committees, preparing medicines-related bulletins and newsletters, training pharmacists in MI skills and undertaking research which focusses on service evaluation [10]. The main element within this is however is responding to individual enquiries [9-16]. The most common types of enquiry are related to administration, appropriate dosing, choice of therapy, medicines, identification and medicines availability [9-16]. Traditionally, many of these enquiries would have been answered using tertiary reference sources and bespoke MI databases. With the development of IT systems and their availability in the clinical setting, tertiary references resources have become more accessible and consequently simple MI enquiries can now be more readily answered by practitioners themselves. Furthermore as the clinical role of the pharmacist has developed their availability to respond to medicines related enquiries in the clinical setting has increased further obviating the need for MI services [17-21]. It may therefore be unsurprising that more recently the extent of MI service provision in the USA has contracted [20,22,23]. A similar pattern has not yet been reported in the UK.
Possible reasons for this contraction in the USA MI service provision may include a reduction in demand due to the increasing ease of obtaining medicines based information from the internet [22,24] or the provision of better local medicines information support by pharmacists as they assume more clinical roles. Alternatively, contraction may be due to a rationalisation of funding in cost constrained health systems where robust evidence for the cost-effectiveness of MI services based on randomised controlled trial does not exist [25,26].
Currently, there is no research which describes how the nature of MI enquiries have changed over time in the UK or which identifies the workload associated with different types of MI enquiry. Therefore, it was decided to identify any historical trends in demand for the service and estimate the time required to deliver different types of enquiry. Such information will then enable managers of MI services to plan their future service provision. The aim of this study was therefore to describe how the nature of MI enquiries has changed over time and to use this to predict how this may affect future demand for the service.
Study design
A retrospective, single-centre analysis of MI enquiries received by one large teaching hospital trust in the UK. All medicines information enquiries within the trust are archived on MI Databank (CoAcS) and this was interrogated for data collection purposes after honorary registration was approved by Addenbrookes hospital.
Study period
Following a one month pilot data collection period, all individual patient based enquiries registered on electronic database MI databank 2™ in May and October from 2006 to 2010 were included in the analysis. These two months were selected as they did not include staff changeover periods in junior doctor rotations, nor were they common months for newly-qualified pharmacist or nurse recruitment.
Data collection
The following data was extracted from each enquiry:
• Enquiry origin (e.g. base organisation (Cambridge University hospital NHS Trust)
• Enquirer status (e.g. doctor)
• Enquirer level of expertise e.g. consultant
• Contact method e.g. letter
• Enquiry category e.g. pregnancy and breast feeding
• Time taken to complete response
• Reply route e.g. telephone
• Complexity of enquiry (e.g. level 1)
Medicine information enquiries are categorised based on the main focus of the question using the UKMi categories. Table 1 outlines the definitions for the different categories.
| Category | Enquiry related to |
|---|---|
| Administration/dosage | As enquiry related to suitable formulation , preparation, dose, choice of administration route of medicines |
| Adverse effects | Enquiry related to adverse drug reactions result from using medicines. |
| Availability/supply/formulary | Availability, supply of medicine(s). |
| Choice of therapy/indication/contraindication | Drug of choice in management, indication or contraindication of medicine(s) use. |
| Drugs in breast milk | Any enquiry related to use of Medicines & their safety whilst breast feeding. |
| Drugs in pregnancy | Enquiry related to use of medicines & safety during pregnancy. |
| Interaction | Related to drug-drug, drug-food, drug-test or drug-disease. |
| Pharmaceutical | Any enquiry related to pharmaceutical excipients as sometimes patients experiencing intolerance to certain product or related to stability of refrigerated products at room temperature |
| Pharmacology/pharmacokinetics | Enquiry related to pharmacokinetic/ pharmacodynamics of medicines or related to study of medicine action. |
Table 1: Categories used for received medicines Information queries.
Enquiry complexity was classified by the recipient of the enquiry using a national system as either:
Level 1 Simple enquiry: Answered using data from one or two standard resources
Level 2 Complex enquiry: Requiring the use of multiple and more specialist sources where the available evidence provides a reasonably clear answer or course of actions
Level 3 Complex enquiry: In the absence of a clear answer or course of action from available sources, professional judgement is used to provide advice to the enquirer; this may require the specialist evaluation of multiple sources and the evaluation of primary literature
Data analysis
All data was analysed using Microsoft Excel and Statistical Package for Social Scientists (SPSS) Windows version 18.
Appropriate descriptive statistics, number (percent) for discrete variables, mean (Standard Deviation) for parametric data and median (Inter quartiles) for non-parametric data were used to describe the data. Historical trends of enquiries (categories, enquiry status, and complexity) were determined graphically.
Multiple regression analysis was used to estimate time spent answering different types of enquiry. All recorded variables were investigated to identify any factors related to time spent answering MI enquiries using multiple regression analysis. Time spent answering MI queries were logarithmically transformed to provide a Gaussian normal distribution. All independent variables within the three sub-headings of origin of enquiry, enquirer status and complexity were dichotomised to yes and no and coded as 1 and 0 respectively. Initially three models were built on the three sub-headings (origin, status, complexity) were developed to identify the individual factors related to log time taken. All independent factors with p<0.05 were included in the final model. Interaction factors were taken into account and the General Linear Model used to determine which independent factors were related to time taken to answer MI queries.
Two months per year over the study period (2006 to 2010) the MI centre at a large teaching hospital received 1605 enquiries.
Figure 1 shows the complexity levels of enquiries received by medicines information over the five year review period. As the proportion of level 1, 676 (42%), enquiries has decreased the proportion of level 2, 752 (47%), enquiries has increased. Mean (SD) time to complete enquiries of complexity level 1, 2 and 3 was 32 (36.1), 83 (88.1), 157 (132) minutes respectively.
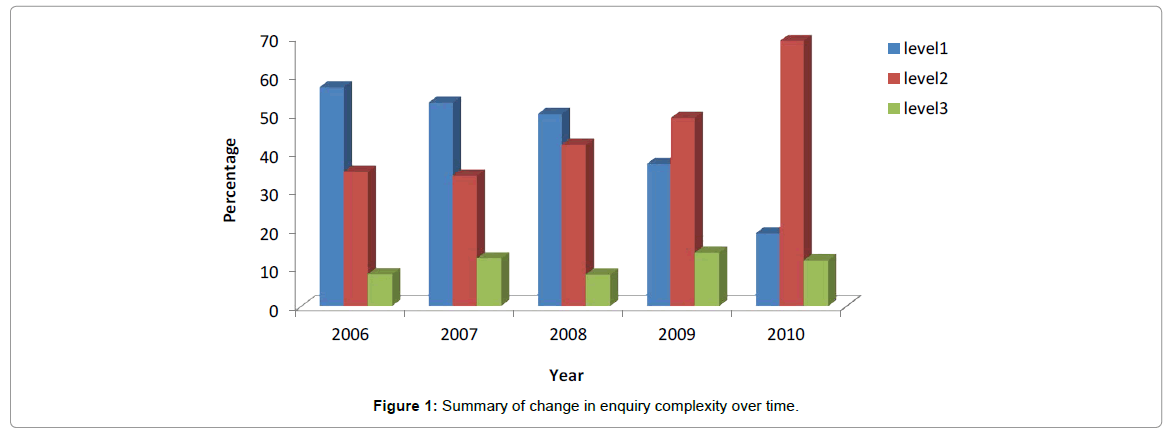
Figure 1: Summary of change in enquiry complexity over time.
Table 2, which summarises the enquiries by different service users, shows that this has not changed significantly over time, with hospital pharmacy staff as the main service users. Over two thirds of enquiries are from hospital pharmacy staff or others and these take the shortest period of time. Enquiries from consultants and general practitioners take the greatest amount of time to complete.
| Enquirer | No. (%) of MI enquiries per year / Median time per minute | Median (IQ) Time (minutes) | |||||
|---|---|---|---|---|---|---|---|
| 2006 | 2007 | 2008 | 2009 | 2010 | Total | ||
| Consultant | 14 (6) 129 |
22(7) 63.0 |
32 (9) 64.5 |
30 (9) 85.0 |
29 (8) 96.0 |
127(8) | 84 (40,175) |
| Registrar | 8 (3) 52.0 |
14(5) 60.0 |
18 (5) 52.5 |
20 (6) 75.5 |
20(8) 49.0 |
80 (5) | 59 (28,117) |
| Junior hospital doctor | 19 (8) 49.0 |
17 (6) 33.0 |
21 (6) 51.0 |
26 (7) 23.5 |
28 (8) 39.0 |
111(7) | 37 (20,76) |
| General practitioner | 13 (5) 45.0 |
11(4) 109 |
10 (3) 113 |
12 (3) 55.5 |
25 (7) 38.0 |
71 (4) | 59 (23,120) |
| Hospital pharmacy staff | 75 (32) 40.0 |
132 (44) 30.0 |
181 (48) 30.0 |
154 (44) 39.5 |
112 (33) 37.5 |
654 (40.7) | 35 (18,175) |
| Community pharmacy staff | 4 (2) 28.0 |
5 (2) 24.0 |
9 (2) 48.0 |
3 (1) 45.0 |
9 (3) 66.0 |
30 (2) | 40 (20,81) |
| Others1 | 105 (44) 38.0 |
93 (31) 36.5 |
104 (28) 26.5 |
107 (30) 29.0 |
120 (35) 24.0 |
532 (33) | 33 (34,75) |
| Total | 238 (15) 41.0 (20,84) |
297 (19) 34.0 (21,62) |
375(23) 35.0 (17,77) |
352 (22) 46.0 (20,90) |
343 (21) 45.0 (22,107) |
1605 (100) | 40 (22,79) |
Table 2: MI enquiries received from different service users and time taken to complete.
Table 3 provides a summary of the trends in the categories of MI enquiries, it can be seen that the number of MI enquiries increased by 50% over the study period and that although the pattern of enquiries was different in 2006 compared to the following four years, the pattern during the following period was relatively static. Administration and pharmaceutical (e.g. enquiry related to medicines stability, formulation and compatibility) based enquiries were the quickest to complete, whereas questions regarding potential adverse events, drugs in breast milk and drugs in pregnancy took the longest.
| MI enquiry categorisation | No. (%)/median Time (Minute) enquiries per year | Median (IQ) Time (minutes) | |||||
|---|---|---|---|---|---|---|---|
| 2006 | 2007 | 2008 | 2009 | 2010 | Total | ||
| Administration/dosage | 66(29) (30.0) |
103(34) (30.0) |
134(36) (27.0) |
128(34) (35.0) |
152(41) (38.0) |
583 (36) | 31(17,133) |
| Adverse effects | 36(16) (67.0) |
31(10) (45.0) |
37(10) (79.0) |
32(9) (103) |
27(7) (145) |
163 (10) | 80 (40,233) |
| Availability/supply/formulary | 14(6) (26.0) |
34(11) (42.5) |
61(16) (35.0) |
46(12) (50.5) |
49(13) (57.0) |
204 (12) | 45 (22,75) |
| Choice of therapy/indication/contraindication | 26(12) (49.0) |
47(15) (38.0) |
36(10) (75.0) |
63(17) (67.0) |
39(12) (79.0) |
211 (13) | 61(29,121) |
| Drugs in breast milk | 7(3) (63.0) |
6(2) (81.0) |
11(3) (60.0) |
7(2) (90.0) |
9(2) (89.0) |
40 (2) | 76(34,179) |
| Drugs in pregnancy | 7(3) (108) |
16(5) (90.0) |
11(3) (70.0) |
14(4) (82.0) |
10(3) (115) |
58 (4) | 90(40,150) |
| Interaction | 35(16) (45.0) |
29(9) (45.0) |
28(8) (49.0) |
31(8) (64.0) |
17(5) (45.0) |
140 (9) | 47(25,88) |
| Pharmaceutical1 | 22(10) (31.0) |
33(11) (28.0) |
39(11) (28.0) |
47(13) (34.0) |
62(17) (41.0) |
203 (12) | 32 (20,59) |
| Pharmacology/pharmacokinetics | 11(5) (49.0) |
8(3) (51.0) |
11(3) (133) |
5(1) (45.0) |
4(1) (58.0) |
39 (2) | 56(28,146) |
| Total number (classified enquiries) | 224 (14) | 307 (19) | 368 (22) | 373 (23) | 369 (22) | 1641(100) | - |
| Total number (unclassified enquiries) | 238 (15) | 297 (19) | 375 (23) | 352 (23) | 343(21) | 1605(100) | - |
Table 3: Categories of medicines information enquiry received and time taken to complete.
Table 4 provides a summary of the final model to predict log time. Adjusted R squared for this model was equal 0.35. It can be seen that level 3, dietician and level 2 enquiries are time consuming and have a higher effect on log t, as they need more time to process. Administration and pharmaceutical categories have the lower effect on log t and they were process quicker than other MI enquiries.
| Model | Unstandardized coefficients (B) | Sig | Time (minute) |
|---|---|---|---|
| (Constant) | 1.371 | .000 | - |
| Level 2 | .361 | .000 | 83.0 |
| Level 3 | .643 | .000 | 157 |
| Administration/dosage | *-.103 | .000 | *-59.7 |
| Adverse effects | .176 | .000 | 114 |
| Pharmaceutical | *-.069 | .032 | *-56.8 |
| Multiple categories1 | .088 | .001 | 99.9 |
| Consultant | .153 | .000 | 126 |
| Dietician | .427 | .000 | 223 |
Table 4: Final regression model to predict time to complete different MI queries.
During the five year period of this review the number of enquires generated and their complexity has increased. Hospital pharmacists are the greatest users of the service but these are largely for queries regarding administration which are relatively quick to answer. Consultants tend to use the service more than other doctors and this is for more complex enquiries.
The increase in both demand and complexity seen however requires regular review as this has significant implications for the workload within the MI department. To manage this increase in workload, further work is required to identify queries which could be more immediately answered on the ward by the enquirer themselves or a clinical pharmacist.
This is the first study to describe the trend of MI service workload in the UK in respect to volume, categories and average time taken spent with answering MI enquiries. In addition, this study also developed a model to predict time taken to answer enquiries. However, there are several potential limitations that should be considered. The analysis of MI enquiries included only two months per year and these many not representative of the whole year. This study took place in a single-centre UK NHS teaching hospital; therefore, it is unlikely that the findings will apply directly to different health care systems in other countries or even between different hospitals inside the UK. In addition, the evaluation of the MI service workload was dependent upon the quality of data entered onto the database and a prospective study may have improved standardisation of recording. Despite the existence of a number of standard criteria established by UKMi [27] used to classified complexity level, these criteria were applied by a range of MI staff, of varying experience and are therefore prone to some subjectivity. The location of MI enquiries within Addenbrooke’s hospital itself was not recorded in MIDatabank, and therefore it was not possible to determine whether these enquiries originated from a small number of locations (wards) or were evenly distributed across the hospital.
Finally, the workload model in this study suggests that the predictive variables explain only 35% of the variance in time spent answering enquiries. This is perhaps unsurprising due to the variability in the time to answer MI enquiries resulting from the wide range of information sources utilised, differences in time to access different resources e.g. primary, secondary and tertiary reference sources, the media utilised for access, paper versus the internet and the different experience of the individuals undertaking the work.
The reason for the increase in MI queries is unknown, however this may reflect the increase in patient turn over in hospitals which have occurred during the time period, it may be due to increased presence of pharmacists on the ward providing an opportunity for doctors to seek advice or may reflect satisfaction with the service driving up demand. Additionally the drive to minimise health service costs may also be resulting in prescribers taking more care to select cost-effective approaches and to minimise the likelihood of patient harm.
The increase in complexity of enquiries may reflect the increase in the number of medicines which patients are prescribed, the fact that patients survive with more morbidity and therefore generate more complex queries or the fact that the availability of the internet and ward pharmacists enables more simple enquiries to be more immediately answered without requiring the MI service.
Unsurprisingly perhaps healthcare professionals within the teaching hospital were the main service users with the greatest proportion coming from hospital pharmacy staff. This is in line with other research [26]. Most of their enquiries were related to drug administration as this category represented the higher percentage; however, such enquiries are processed more quickly than other categories. Increased time for MI queries from healthcare practitioners other than pharmacists has been reported elsewhere [18]. With almost half of enquiries received from hospital pharmacists being of the lowest complexity it suggests that better access to reference sources on the ward, perhaps electronically, may prevent a number of enquiries. A previous study showed that a detailed analysis of level 1 enquiries from hospital pharmacists identified that 25% could have been completed without referral to MI and an additional 20% could have been answered if Medicines Complete (Martindale, Stockley’s Drug Interactions) had been available on the ward [28]. Providing a pro-active material e.g. IV guide, SWANG database (in house intranet advice about administration of medicines to patients with swallowing difficulties or NG tubes) would help to reduce the MI centre workload and provide a safe reference for users.
Interestingly whilst the number of consultants in the hospital is less than the number of registrars and junior doctors, they tended to generate the most queries which on average took longer to respond to. The greater time required to answer consultant enquiries may be due to the specialist nature of their role. Dieticians often asked about nutrition content of medicines and this requires contacting the manufactures to obtain the information. Registrars and junior doctors spend more time on the ward and therefore are able to more readily access the ward based pharmacist where many of their queries may be directed through. Whilst registrars are experienced and therefore may have less need for MI services, the small numbers of queries generated by junior doctors is surprising. Further work to better understand how junior doctors obtain medicines information in the hospital is however warranted.
When considering the nature of enquiries it can be seen that questions regarding medicines administration are the most frequent but usually take less time to answer and this probably reflects the fact that most can be answered with one reference source. A detailed review of these queries may be useful as it may be possible to provide access to more useful reference sources on the ward or access to answers to the most frequently asked questions to prevent some of these from reaching the MI service. Such an approach has been recommended by other researchers [28].
The study shows that certain types of enquiry e.g. interactions and safety in pregnancy and breastfeeding take longer on average to answer. References sources which provide answers to simple questions regarding these topics are available on the ward (BNF reference) and consequently only complex enquiries where information will require detailed research will be sent to the MI service. It could be argued that this is the remit of the MI service as ward based pharmacists are now all trained in how to answer basic MI queries and the skills required for data synthesis and critical appraisal are those which are unique to the MI service providers.
The results obtained from the regression analysis showed that MI enquiries are related to level of enquiry complexity, users’ profession, and type of enquiry. This provides a more complex picture than that provided by other researchers who have just linked time to complexity [26]. The picture is more complex than purely the number of sources used to answer a query, which is the primary driver for defining complexity, as the nature of the enquiry and the person who asks the question will have an effect on the average time taken Consequently any moves to further promote the service to such groups or for certain types of enquiry should take this complexity into consideration.
Over the five year period of review demand for MI services has increased in one teaching hospital. The increase in number and overall complexity of enquiries, which may reflect the increase in turn over in patients within the hospital, increased availability of ward based pharmacists and the success of the service, has a significant impact of workload within the MI team. A review of less complex enquiries received by the service is warranted to ensure that only those queries which require the expertise of the team are answered by the service.
Greater provision of information resources on the ward could reduce this burden. The time taken to respond to enquiries can be predicted by enquiry complexity, profession of the enquirer and the nature of the enquiry and consequently any plans to promote the service further require cognisance of these factors.
The information provided by this study should provide data to enable other hospitals to compare their service with. The process of reviewing five years data enables the future workload to be predicted and for areas for review to be identified to ensure that the service utilises the expertise of the MI staff most appropriately.
The authors would like to thanks all Medicines Information staff at Cambridge University hospital NHS Trust who helped and provided a [29] devices during the data collection process, special thanks to staff members / School of Pharmacy/ University of East Anglia/ Norwich Research Park/ Norwich/ UK for their supervision, assistance, and funding this research.