Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2014) Volume 4, Issue 1
Abstract
Background: Two methods of pancreatic duct decompression following pancreaticoduodenectomy (PD) are currently employed, the internal and external pancreatic duct stent. Previous analysis of the efficacy of ductal decompression following PD has been confounded by either including both the internal and external stent method or by small sample size. The aim of this meta-analysis was to analyze the efficacy of the external pancreatic duct stent method alone in preventing Post-Operative Pancreatic Fistula (POPF) formation and other complications in patients undergoing PD.
Methods: A systematic literature search was conducted using the Medline, Cochrane Library, SCI, and EMBASE databases on all studies published from January 1970 to March 2012 reporting the peri-operative outcomes following PD. The primary end-point was the incidence of POPF formation in the presence of external pancreatic duct stent placement. Secondary outcomes considered included the incidence of post-operative mortality, Delayed Gastric Emptying (DGE), postoperative wound infection, operative time and blood loss, and length of hospital stay.
Results: Four trials were included comprising 416 patients. There was a statistically significant decrease in the incidence of both any grade POPF formation (OR 0.37, 95% CI=0.23 to 0.58, P=0.0001) and clinically significant (grade B or C) POPF formation (OR 0.50, 95% CI=0.30 to 0.84, P=0.0009) in patients receiving an external pancreatic duct stent versus no stent following PD. Total length of hospital stay was also found to be shortened with the use of an external stent (SMD -0.39, 95% CI=-0.63 to -0.15, P=0.001).
Conclusions: There is a decreased incidence of POPF formation following PD in patients receiving an external pancreatic duct stent versus patients receiving no stent. Total length of hospital stay was also found to be favorably affected by placement of an external pancreatic duct stent.
Keywords: Pancreatic duct stent; Pancreaticoduodenectomy; Pancreatic carcinoma; Post operative pancreatic fistula
The National Cancer Institute has estimated that there will be as many as 45,220 new cases of pancreatic cancer in the U.S. in 2012 and that as many as 38,460 patients will die of the disease this year alone [1]. Pancreaticoduodenectomy (PD) remains the sole potentially curative intervention for several types of peri-ampullary and pancreatic carcinomas and pathologies. Postoperative Pancreatic Fistula Formation (POPF) as a result of pancreaticojejunostomy (PJ) anastomotic failure remains one of the most serious and dreaded complications following PD. POPF is believed to be a consequence of pancreatic exocrine secretion seepage across a compromised anastomotic site, with the most likely mechanism being autodigestion and destruction of the tissue surrounding the PJ anastomotic site leading to dehiscence and seepage into the abdominal cavity. The release of these activated pancreatic juices then cause peripancreatic collections, intra-abdominal abscesses, hemorrhage, and POPF [2].
Protection of this anastomotic site has therefore been the focus of many modifications to the original Whipple procedure. Stent placement across the PJ anastomsis has been proposed to protect the integrity of the site by diverting the potentially caustic exocrine secretions of the pancreatic remnant away from the delicate anastomotic site. In addition, such stents have been theorized to promote precise placement of anastomotic sutures, facilitate decompression of the pancreatic remnant, and maintain patency of the pancreatic duct postoperatively [3,4].
Two similar though uniquely different procedures have been integrated into the traditional PD procedure with varying reports of actual efficacy; an internal and an external pancreatic duct stent. The internal stent technique is generally performed by inserting a 6 cm stent into the pancreatic duct such that one-half of its length remains within the duct itself, bridges across the anastomotic site, and empties into the jejunal lumen. In contrast, the external stent utilizes a longer stent placed similarly within the pancreatic duct stump, bridges across the anastomotic site into the jenual lumen, but the tail of which is exited through a small enterotomy site in the free end of the jejunal loop. This is then closed with a purse-string suture, externalized via a stab incision in the anterior abdominal wall, and closed by suturing the serosa of the jejunum to the peritoneum of the abdominal wall. In both cases migration of the catheter is prevented with an absorbable suture attachment to the jejunal mucosal surface [4-9]. The final PJ reconstruction is then carried out with an end-to-side, duct-to-mucosa anastomosis using 1-or 2-layer interrupted fine sutures [6].
Previous meta analysis performed by Markar et al. [10] examined the combined effect of placement of either stent type on clinical outcome following PJ. Based on the integrated data sets, these authors identified a non-statistically significant trend towards reduced pancreatic fistula with the use of either stent method but the data was unable to definitively rule out the null hypothesis that stenting had no beneficial effect. Given the unique mechanism and distinctive risk and reward profiles of each individual technique, these results may have been affected by co-intervention bias as described by Kelly et al. [11].
The purpose of the present meta-analysis was to determine whether the technique of externalizing the pancreatic duct stent is indeed efficacious in minimizing the incidence of postoperative morbidity and mortality, including POPF formation, versus no stent Placement Following PJ.
An electronic literature search was conducted among all articles from January 1970 to March 2012. Medline, Cochrane Library, SCI, and EMBASE were searched using the following text and keywords in combination with both Medical Subject Headings (MeSH) and text words: “Whipple procedure”, “pancreatoduodenectomy”, “pancreatic fistula”, and “pancreaticojejunostomy”. Further searches were extended to Oncology journals from Asian, American and European continents. In addition, bibliographies of included studies were screened for any additional literature. Prospective randomized control trials reporting primary outcomes on pancreatic fistula and mortality from stent versus non-stent during PJ were reviewed.
Inclusion criteria
Studies included in this analysis were those that were prospective randomized control in nature and that reported POPF formation or at least one of the secondary outcomes of interest in patients receiving an external pancreatic duct stent versus no stent following PD.
Exclusion criteria
Studies were excluded from this study if they included nonrandomized control trials, utilized an internal pancreatic duct stent technique, those in which the outcomes of interest were impossible to calculate from the published results, or those in which the standard deviation of the mean for continuous outcomes of interest (operative time, blood loss, and length of hospitalization) were not reported.
Assessment of study quality
The quality of the randomized control trials included in this study was assessed using the Jadad scoring system [12], which was based upon three criteria; 1) randomization of cohorts, 2) double-blind assessment, and 3) accountability for patients either not included or withdrawn from the study (Table 1). Quality guidelines were adherent to QUOROM (Quality of Reporting of Meta-analyses) statements in order to increase transparency of conclusions made by the aperi-operativeuthors [13]. Methodological qualities were independently assessed and any discrepancies were resolved with detailed discussion. A QUOROM flow chart was also created (Figures 1 and 2).
| Kuroki et al. [14] | Motoi et al. [7] | Pessaux et al. [9] | Poon et al. [6] | ||
| Number of patients | Stent | 23 | 47 | 77 | 60 |
| No stent | 22 | 46 | 81 | 60 | |
| Age | Stent | 68.1 ± 11.2 | 66.0 (33-79) | 60.8 ± 11.8 | 61 ± 12 |
| No stent | 68.2 ± 8.4 | 65.5 (32-80) | 60.6 ± 11.8 | 62 ± 13 | |
| Male/Female | Stent | 13/10 | 26/21 | 39/38 | 31/29 |
| No stent | 12/10 | 29/17 | 47/34 | 41/19 | |
| BMI | Stent | 21.0 ± 3.0 | 21.7 (14.3-32.4) | 24.6 ± 4 | NR |
| No stent | 21.9 ± 3.0 | 21.5 (16.3-29.3) | 25.2 ± 4.7 | NR | |
| Pancreatic duct size | Non-dilated (< 3mm) | 35 | 41 | 158 | 60 |
| Dilated (> 3mm) | 10 | 52 | (excluded) | 60 | |
| Pancreatic texture | Soft | 45* | 47 | 158 | 66 |
| Hard | 22* (excluded) | 46 | (excluded) | 54 | |
| Jadad’s score12 | 3 | 3 | 3 | 3 | |
*Kuroki et al. [14] differentiated soft from hard pancreatic utilizing a Time-signal Intensity Curve (TIC) based upon dynamic contrast-enhanced Magnetic Resonance Imaging (MRI).
NR: Not Reported
Table 1: Baseline and intraoperative demographics.
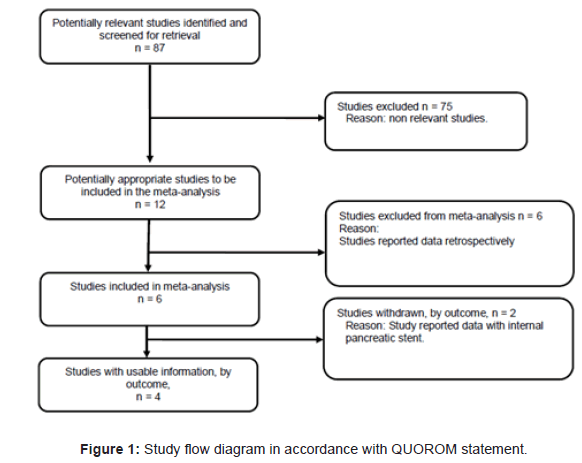
Figure 1: Study flow diagram in accordance with QUOROM statement.
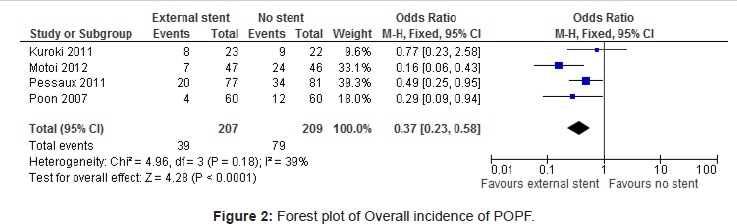
Figure 2: Forest plot of Overall incidence of POPF
Outcomes of interest
The primary outcome of interest was the incidence of POPF formation following PD in the presence versus absence of external pancreatic duct stent placement. Secondary outcomes considered were peri-operative mortality, delayed gastric emptying, operative time and blood loss, and total length of hospital stay.
Statistical analysis
Data on the endpoint measures were entered into a digital spreadsheet for analysis. Data analysis was performed utilizing the freeware program Review Manager (RevMan, Version 5.1 for Windows, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011). For dichotomous data, the Mantel-Hansel method was utilized with a fixed effect model and a 95% confidence interval. Dichotomous data results were considered to be statistically significant with a p value <0.05 provided the 95% confidence interval did not include the value 1. For continuous data reported as mean ± standard deviation, an inverse variance method was used with a fixed effect model and a 95% confidence interval. Continuous data results were considered to be statistically significant with a p value <0.05 provided the 95% confidence interval did not include the value 0. The data for the various outcomes was entered into the RevMan software and Foster plots were generated.
Similar to the previous meta-analysis performed by Marker et al. [10], preliminary electronic and manual searches returned 15 articles matching the initial search criteria. Subsequent screening resulted in four prospective randomized trials examining only external pancreatic stents following PD [6,7,9,14]. Of note, the present study excluded two trials previously included by Markar et al. [10]; 1) the 2009 prospective trial conducted by Smyrniotis et al. [5] on the basis that this study examined internal stents only, and 2) the 2006 trial conducted by Winter et al. [4] on the basis that internal stents were included and because these authors utilized an alternating method of allocating patients to either treatment or control arms, which may have inadvertently introduced selection bias as described by Doll [15]. Baseline and intra-operative demographics of the study populations are listed in Table 1.
All four trials reported on the incidence of POPF formation following PD with versus without external pancreatic duct stent placement [6,7,9,14]. There was a statistically significant difference in the overall incidence of any grade POPF formation among these cohorts (OR 0.37, 95% CI=0.23 to 0.58, P=0.0001) as well as a statistically significant difference in the incidence of clinically significant (grade B or C) POPF (OR 0.50, 95% CI=0.30 to 0.84, P=0.0009) favoring external stent placement (Table 2). Two trials reported length of hospital stay among these two populations, which was found to be statistically significant favoring external stent placement (SMD -0.39, 95% CI=-0.63 to -0.15, P=0.001) [6,9].
| Number of studies | Participants | Odds Ratio (M-H, Fixed, 95% CI) | Statistical Difference | |
| Pancreatic fistula (any grade) with respect to stent | 4 [6,7, 9,14] | 416 | 0.37 [0.23, 0.58] | S (P=0.0001) |
| Clinically significant (grade B or C) pancreatic fistula with respect to stent | 4 [6,7,9,14] | 416 | 0.50 [0.30, 0.84] | S (P=0.0009) |
| Pancreatic fistula with respect to duct diameter | 2 [6,7] | 213 | 4.88 [1.97, 12.04] | S [P=0.0006) |
| Length of hospital stay | 2 [6,9] | 278 | SMD -0.39 [-0.63, -0.15] | S (P=0.001) |
| Perioperative mortality | 3 [6,7,9] | 371 | 0.86 [0.27, 2.73] | NS (P=0.80) |
| Delayed gastric emptying | 3 [6,7,9] | 371 | 0.54 [0.29, 1.01] | NS (P=0.05) |
| Postoperative wound infection | 3 [6,7,9] | 371 | 0.77 [0.38, 1.56] | NS (P=0.047) |
| Total operative time | 3 [6,9,14] | 323 | SMD -0.12 [-0.34, 0.10] | NS (P=0.29) |
| Intraoperative blood loss | 3 [6,9,12] | 323 | SMD 0.04 [-0.18, 0.26] | NS (P=0.71) |
Table 2: Intra- and post-operative outcomes.
There was no significant difference in the incidence of perioperative mortality (3 trials [6,7,9]: OR 0.86, 95% CI=0.27 to 2.73, P=0.80), delayed gastric emptying (3 trials [6,7,9]: OR 0.54, 95% CI=0.29 to 1.01, P=0.05), or postoperative wound infection (3 trials [6,7,9]: OR 0.77, 95% CI=0.38 to 1.56, P=0.047) between external stent and non-stent groups. Likewise there was no significant difference in the total operative time (3 trials [6,9,14], SMD -0.12, 95% CI=-0.34 to 0.10, P=0.29) or intraoperative blood loss (3 trials [6,9,14], SMD 0.04, 95% CI=-0.18 to 0.26, P=0.71) identified.
POPF remains one of the most common and serious complications following pancreatic resection with PJ and is widely regarded as the most ominous indication of clinical course. The two most uniformly and definitively cited risk factors for developing POPF are soft texture of the pancreatic remnant [14-16] and diameter of the pancreatic duct stump [17]. This suggests that the integrity of the PJ anastomosis and its susceptibility to failure is of critical importance in preventing POPF. Thus, exclusion of pancreatic exocrine secretions from the anastomotic site is essential.
The use of a stent to physically isolate the PJ anastomotic site from pancreatic secretions while also providing a conduit for pancreatic decompression is supported by several prospective randomized trials. In a 2012 randomized control trial, Motoi et al. found that the incidence of clinically significant POPF (Figure 3) was decreased in the presence of an externalized pancreatic duct stent (6.4% stented vs. 21.7% non-stented, P=0.04) [7]. Furthermore, researchers noted that among patients with a non-dilated pancreatic duct stump (≤ 3 mm) the incidence of clinically relevant POPF was significantly lower in the external stent group versus non-stented group (9.5% stented vs. 40% non-stented, P=0.033). Among patients with a dilated (>3 mm) pancreatic duct stump, however, the authors noted that the incidence of POPF was equivocal (3.8% stented vs. 7.7%, P=1.0).
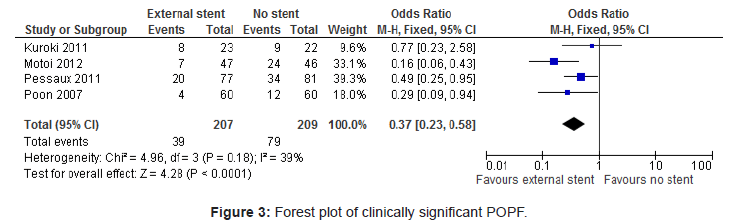
Figure 3: Forest plot of clinically significant POPF.
In 2011, Pessaux et al. [9] examined placement of an external pancreatic duct stent only among high-risk patients, those with a soft pancreatic remnant texture or a non-dilated pancreatic duct (<3 mm). These researchers found that the incidence of POPF was significantly reduced among the stent group (26% stented vs. 42% non-stented, P=0.034) and that the stented group had a significantly lower overall morbidity (41.5% vs. 61.7%, P=0.01), surgical morbidity (35.1% vs. 55.5%, P=0.009), and delayed gastric emptying (7.8% stented vs. 27.2% non-stented, P=0.001) compared to the non-stented group. In a similar 2007 randomized control study, Poon et al. [6] found that external drainage of the pancreatic duct significantly reduced the incidence of POPF (6.7% stented vs. 20% non-stented, P=0.032) and length of hospital stay (mean of 17 days stented vs. 23 days non-stented, P=0.039) following PJ. Furthermore, they noted that the incidence of pancreatic fistula was reduced among stented patients with a nondilated pancreatic duct (14.3% stented vs. 25% non-stented, P=0.349) as well as those with a dilated pancreatic duct (3.1% stented vs. 10.7% non-stented, P=0.257), though neither of these conclusions achieved statistical significance.
However, several studies have refuted the utility of pancreatic duct stenting in mitigating POPF. In 2011, Kuroki et al. [14] found no significant difference in the incidence of any grade POPF (34.5% stented vs. 40.9% non-stented, P=NS) or clinically significant POPF (21.7% stented vs. 27.3% non-stented, P=NS) among patients with a soft pancreatic remnant utilizing the external duct stent following PD. This suggests that while a soft pancreatic texture is a well-documented risk factor for POPF formation [15-19], pancreatic duct stenting has no effect on mitigating that risk.
The meta-analysis performed here has demonstrated that external pancreatic duct stent placement does significantly reduce the incidence of POPF and length of hospital stay following PD. Given that this study differed from the previous meta analysis performed by Markar et al. [10] in just one respect, that the external stent method alone be considered, the conclusion that the external stenting and not internal stenting is efficacious in preventing POPF is reasonable. However, this conclusion is in contrast to the unique 2010 prospective randomized controlled trial by Tani et al. [3], which found that the specific type of drainage stent had no impact on the overall incidence of postoperative complications including POPF (26% internal vs. 20% external, P=NS). This study was hampered by a small sample size, however, and may have suffered from limited the power. Additional randomized controlled trials studies comparing the efficacy of internal versus external pancreatic duct stenting is therefore warranted.
Taking into account both the meta-analysis performed here as well as the breadth of literature summarized above, it is clear that external pancreatic duct stenting does indeed reduce pancreatic leakage leading to POPF, particularly among high-risk patients with a non-dilated pancreatic duct ≤ 3 mm. At present it appears that this effect is not replicated among patients with a dilated (>3 mm) pancreatic duct. Although the univariable analysis of several studies have identified soft pancreatic texture as risk factor for the development of POPF [4,6,7], stenting does not appear to mitigate this risk in any significant manner.
The trend observed that beneficial results were observed most prominently among patients with a non-dilated pancreatic duct supports the hypothesis that the mechanism of action is at least in part due maintaining lumen patency and preventing inflammationrelated constriction and subsequent intraductal hypertension, which would theoretically be more prevalent among smaller duct sizes. This mechanism mimics those of endoscopically placed pancreatic duct stents placed following ERCP for a variety of pancreatic pathologies [20].
The fact that only external stents demonstrated efficacy in preventing POPF or other related complications post-PJ supports previous hypotheses that the longer external stents prevent either premature stent migration or occlusion, which in theory may be more prevalent with the shorter internal stent [21]. The hypothesis previously put forth by Biehl and Traverso [22]. in their animal models that the stent acts as an instrument to assist in the precise placement of sutures, and thereby facilitates a more effective PJ anastomosis, is plausible given that smaller ducts are inherently more difficult to suture. However, should this be the predominant mechanism of action one would expect similar efficacy among both internal and external stents, which has not been shown to be the case.
The results of this study have demonstrated a statistically significant reduction in the incidence of both any grade and clinically significant POPF following PJ using an external pancreatic duct stent. This result affirms the trend towards reduced pancreatic fistula utilizing pancreatic stents previously identified by Markar et al. [10], though with the scope limited to just external stent placement. In the context of all the available literature and trials to date, it is our conclusion that placement of an external pancreatic duct stent is efficacious in preventing POPF and shortening hospital stay among patients with a non-dilated (≤ 3 mm) pancreatic duct. Further randomized controlled trials comparing external pancreatic duct stent versus no stent among patients with a non-dilated pancreatic duct, with sub-group analysis of soft versus fibrotic pancreatic texture, is warranted to confirm these conclusions.
We thank Mr. Dan Dunlany, our librarian for his support for getting all full text articles.