Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Research Article - (2018) Volume 6, Issue 1
Objective: To determine the most appropriate indication for total resection (TR) or partial resection(PR) of infected aortic grafts.
Methods: A meta-analysis was conducted on the rates of early/late mortality, amputations and reinfection. A meta-regression was performed with 8 variables: patient age, male prevalence, presence of prosthetic duodenal fistula (PDF), presence of virulent or nonvirulent organisms, urgency, omentoplasty and follow-up.
Results: For TR and PR, the rates of early mortality and reinfection were 16.8% and 10.5%, 11% and 27% respectively.
For TR, the rates of early mortality and reinfection for in situ reconstruction with allografts and veins were 23% and 10.7%, 10.5% and 2.8% respectively.
For TR, urgency, male gender and omentoplasty all had a negative correlation with early mortality. Omentoplasty had a positive correlation with late mortality. Male gender, PDF and virulent organisms had a negative correlation with reinfection, whereas nonvirulent organisms had a positive correlation. Presence of PDF and follow-up had a negative correlation with amputation, whereas male gender had a positive correlation. For PR, no statistical correlation was analyzable except a negative correlation between PDF and reinfection.
Conclusion: For TR, operative mortality increases in males, and in emergencies, so total removal of the infected aortic graft seems not advisable, and alternative interventions should be considered. With regard to the risk of reinfection, TR appears recommendable in the presence of nonvirulent infectious organisms, but there is increased risk in the presence of virulent organisms and PDF, and so other optimal options may be discussed.
For PR results were not analyzable except for a negative correlation in the presence of PDF.
Keywords: Aortic grafts; Infection; Partial resection; Total resection; Prosthetic duodenal fistula
Aortic graft infection (AGI) is a life-threatening complication that occurs in 1% to 4% of patients who undergo conventional abdominal aortic surgery [1-3] causing major morbidity, mortality, and economic cost [4-6]. The prognosis depends on a multitude of factors including the underlying condition of the patient, urgency, presence of sepsis, virulence of the infecting organism(s), infection linked to prostheticduodenal fistula (PDF), and the surgical modalities of AGI treatment [7-11].
Contemporary management of AGI includes total removal of the infected graft with either concomitant extra-anatomic reconstruction (EAR) or in situ reconstruction (ISR) [12]. In a recent meta-analysis, ISR was associated with a lower occurrence of events, (early mortality, amputation, and reinfection) than EAR, and these results suggest that ISR may be considered as a first-line treatment [13]. On the other hand, partial graft preservation techniques are becoming increasingly popular as a method to treat established graft infection [14-18]. However, partial resection (PR) varies widely in the series, there is no consensus for assessing the extent of infection on the graft, indications are not clear, and outcomes reported in the series are limited.
Most authorities agree that total resection (TR) of the infected aortic graft is mandatory for intracavitary AGI [19-21]. However, extensive dissection to achieve total graft excision could disrupt the collateral blood supply and create a problem of pelvic and limb ischemia [22,23]. Moreover, the total graft removal approach is clearly not feasible in some patients with severe comorbidities or extremely hostile abdomens [24]. Ultimately, surgical management can vary, depending on surgical preference and any requirements concerning the underlying conditions of individual patients.
Despite a considerable number of publications including total or partial excision of the infected aortic graft, a lack of sufficient outcome data has so far precluded clear indications, and there has been no systematic review or meta-analysis to assess the clinical outcomes of ISR associated with the 2 excision modalities. The purpose of this metaanalysis was to determine the most appropriate indication for TR or PR of an infected aortic graft in light of the different outcomes after ISR, and to statistically compare the estimated mean occurrence rate of the following events: early (operative) /late mortality, amputation and reinfection. These rates were pooled from studies including the following variables: age, male prevalence, emergency operation, PDF, omentoplasty, microbiology data, follow-up, and different modalities of ISR: cryopreserved allografts, autogenous femoral veins, standard polyester/PTFE, Rifampicin-bonded and Silver-coated prostheses.
The present review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [25]. A review protocol can be accessed online in (Supplementary, Appendix A).
Research strategy
A literature search was performed using MEDLINE and EMBASE, covering all studies published in English between January 1997 and June 2017, as well as recommendations for reporting treatment of aortic graft infections [26]. The medical subject headings (MeSH) used for the search were aortic, graft, and infection. The following key words were also used: Rifampin or Rifampicin-coated polyester grafts, polyester or Dacron, cryopreserved allografts, autogenous veins, Silver-coated polyester, prosthetic-duodenal-fistula, and partial resection (PR), or total resection (TR).
Inclusion and exclusion criteria were defined to determine the selection of clinical studies (detailed online in (Supplementary, Appendix B). References from identified studies were also reviewed to ensure that all relevant published papers had been identified. The electronic search was accompanied by a manual search of all the reference lists from the relevant articles.
Study selection
The selected clinical studies included ISR with autogenous veins, cryopreserved allografts and synthetic prostheses that were either standard, Rifampicin bonded or Silver coated polyesters. They also included PDF, (classified as a separate entity [26] and the modality of intervention (emergency or planned) for assessment in the metaregression analysis. Special attention was paid to the extent of the resection: total resection (TR) or partial resection (PR) of the infected aortic graft.
With no prior knowledge of the authors or the outcomes of the selected publications, two reviewers used a standardized scoring system to rate the clinical and methodological quality of each study [27] (detailed online in (Supplementary, Appendix C). Studies that did not rate above a quality score threshold (e.g. 18/28) were excluded from the meta-analysis. All studies that did meet the inclusion and exclusion criteria were found to have a quality score above this threshold. These assigned quality scores were not used to compare the results of individuals studies.
Data extraction
When the available written information was insufficient for the meta-analysis, strenuous efforts were made to contact the principal investigator and obtain the necessary information in order to reduce the effect of publication bias.
Two reviewers independently extracted the data from each selected publication. Inter-rater reliability was high. The primary outcome measures were early mortality (defined as “perioperative” and “30-day” mortality), and late mortality (defined at 1 year and onwards because follow-up was rarely possible beyond 1 year). Additional data was extracted regarding rates of amputation and reinfection of the in-situ graft.
Statistical analysis
We used Comprehensive Meta-Analysis software to carry out this project. With this software, we estimated the pooled values of the parameters (estimation of frequency in meta-analysis) as well as their confidence intervals.
We estimated the heterogeneity using Cochran’s Q test with the point estimate of I2. Heterogeneity was visually analyzed with a Forest plot and quantified using Cochran’s Q test with the point estimate of I2. If heterogeneity was present (Q statistic at 5%, and I2 high), we took it into account using the DerSimonian and Laird random-effects method, and if not, using the fixed-effects method.
As there were no randomized trials, when we compared 2 groups, we used a percentage comparison test between the 2 independent groups (chi-squared test). We then researched the publication bias using the Egger method and the trim and fill method. With the latter, we reassessed the results and their confidence interval, taking into account potential missing studies belonging to the analyzed pool. Since the percentage tests generally concerned more than 2 modalities, we used the chi-squared test to compare one level with the other levels. When appropriate, correction for multiple comparisons was performed for subgroup analysis.
Meta-regressions were carried out to estimate the heterogeneity effects according to confounding variables, as defined: patient age (above the mean age, patients were defined as older), male prevalence, emergency ISR, presence of PDF, virulent infectious organisms (i.e., Staphylococcus aureus, Enterobacteriaceae, beta-hemolytic Streptococcus, Pseudomonas), non-virulent infectious organisms (i.e., commensal organisms or negative bacteriological cultures), omentoplasty and follow-up. We performed meta-regressions when the number of studies was higher than or equal to 3. The outcome of these methods enabled us to discuss the final results and justify our propositions.
Besides the meta-analysis software, we used the SAS software version 9.3 at the University Institute of Clinical Research of Montpellier (UPRES 2415 Team. Aide à la décision médicale personnalisée - Personalized support for therapeutic decision).
A total of 2,327 unique articles were identified, 382 of which were retrieved for analysis. Inclusion/exclusion criteria were met by 31 publications. Ten articles were excluded using a standard scoring system (detailed online (Supplementary, Appendix D). Twenty-one studies and 1,052 patients, were included in this meta-analysis (detailed online in (Supplementary, Appendix E). They were classified according to the extent of infection of the aortic graft (either as P0 graft infection of cavitary graft, eg. aorto-aortic or aorto- bi-iliac graft, or as P2 graft infection of extra-cavitary graft, eg. infection of extra-cavitary portion of the graft whose origin is cavitary, e.g. aorto-bifemoral graft) [26] and the extent of resection of the infected aortic graft: total resection (TR), or partial resection (PR).
Nearly all the studies used in this meta-analysis were retrospective and observational. As expected, none of the studies were randomized control trials. The primary characteristics of clinical studies and covariates used in this meta-analysis are detailed online in (Supplementary, Appendix F) [7-10,17,18,28-42].
The mean number of patients across all studies was 50 (range: 2-220). There were 887 TR (84 %), and 165 PR (16%) with 6 studies (382 patients) combining TR (259 patients) and PR (123 patients) [ 9,29,32,34,38,40], 11 studies with solely TR (628 patients: 335 cryopreserved allografts, 259 autogenous veins, 23 standard polyesters/ PTFE, and 11 rifampicin-bonded polyesters) [7,8,10,28,30,31,33,35,39,41,42] and 4 studies with solely PR (42 patients: 23 autogenous veins, 11 silver-coated polyesters, and 8 standard polyesters/PTFE) [17,18,36,37].
The mean patient age for the entire series was 66.1 years (range 29- 91 years); the mean age of patients with TR and PR was 65.1 years (range 29-86 years), and 67.7 years (range 43-91 years) respectively (P=NS).
Different comorbidities and risk factors, detailed online in (Supplementary, Appendix E), were not available in all the studies, and therefore statistical comparison between the outcomes of the patients with TR and PR must be interpreted with caution.
Outcomes after total resection
Early mortality: Separate sets of data were available for 13 studies (642 patients), with inter-study heterogeneity (I2=61.3%, PHET=0.002). According to the random-effects method, the operative mortality rate was 16.2%; 95% CI: 11.3%-22.6%. No publication bias was identified by Egger’s regression test. However, one study was missing, identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included this study as a measure of conservation for the assessment of the adjusted operative mortality rate: 16.8%; 95% CI: 11.8%-22.6%, (Table 1). In a meta-regression analysis (Table 2) urgency of the intervention (P=0.001), male prevalence (P=0), and omentoplasty (P=0) had a negative correlation with operative mortality (Figure 1-3).
| No of trials analysis |
I2 statistic | P for heterogeneity |
Method (fixed or Random- effects Model) |
Event Rate | IC Event Rate | |
|---|---|---|---|---|---|---|
| Random model if heterogeneity test is significant or fixed model if not | ||||||
| Operative mortality | 13 | 61.3 | 0.002 | Random | 0.162 | 0.113-0.226 |
| Reinfection | 16 | 69.7 | 0 | Random | 0.064 | 0.034-0.117 |
| Amputation | 14 | 29.7 | 0.14 | Fixed | 0.068 | 0.048-0.095 |
| Late mortality | 11 | 37.4 | 0.1 | Fixed | 0.279 | 0.243-0.319 |
| Event rates after corrections of selection bias (Dural and test is trim and fill) | ||||||
| Operative mortality | 0.168 | 0.118-0.226 | ||||
| Reinfection | 0.11 | 0.06-0.19 | ||||
| Amputation | 0.081 | 0.06-0.11 | ||||
| Late mortality | 0.285 | 0.250-0.320 | ||||
Table 1: Meta-Analysis and Heterogeneity Tests of the Results for Total Resection.
| Event | Variables | group | Study N | Slope | Slope 95 % IC | p-value | T2 |
|---|---|---|---|---|---|---|---|
| Operative Mortality | % male | TR | 10 | 0.04 | -0.08 | 0 | 0.144 |
| PR | 3 | 0.06 | -0.22 | 0.27 | 0 | ||
| Omentoplasty | TR | 3 | 0.05 | 0.02-0.08 | 0 | 0.054 | |
| PR | No correlation analyzable | ||||||
| Emergency | TR | 10 | 0.04 | 0.02-0.06 | 0.001 | 0.1 | |
| PR | No correlation analyzable | ||||||
| Late Mortality | Omentoplasty | TR | 3 | -0.09 | -0.13 | 0.006 | 0 |
| PR | No correlation analyzable | ||||||
TR: total resection; PR: partial resection.
Table 2: Meta-Regression Analysis of the Risk of Operative and Late Mortality According to Male gender, Omentoplasty and Emergency.
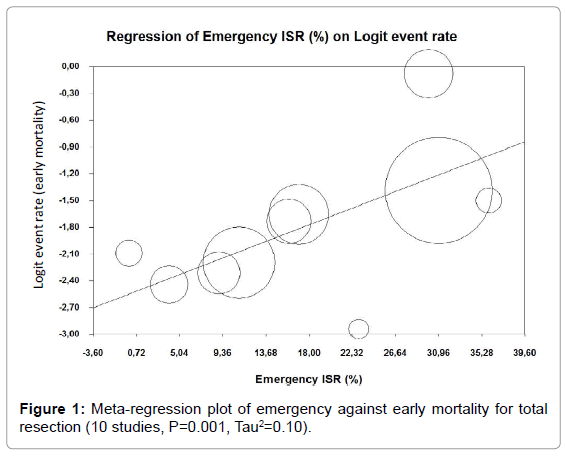
Figure 1: Meta-regression plot of emergency against early mortality for total resection (10 studies, P=0.001, Tau2=0.10).
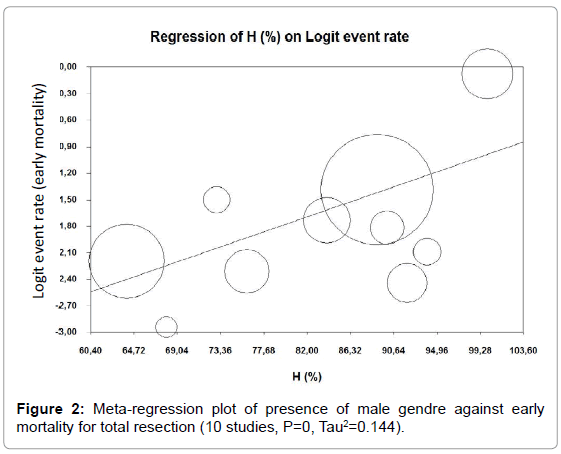
Figure 2: Meta-regression plot of presence of male gendre against early mortality for total resection (10 studies, P=0, Tau2=0.144).
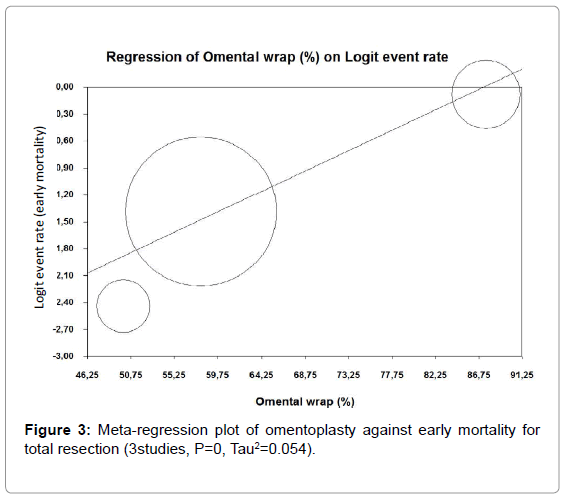
Figure 3: Meta-regression plot of omentoplasty against early mortality for total resection (3studies, P=0, Tau2=0.054).
Late mortality: Separate sets of data were available for 11 studies (585 patients), with no inter-study heterogeneity (I2=37.4%, PHET=0.1). According to the fixed-effects method, the late mortality rate was 27.9%; 95% CI: 24.3%-30.5%. A publication bias was identified by Egger’s regression test. However, three studies were missing identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted late mortality rate: 28.5%; 95% CI: 25%-32%, (Table 1). In a meta-regression analysis (Table 2), only omentoplasty (P=0.006) had a positive correlation with late mortality (Figure 4).
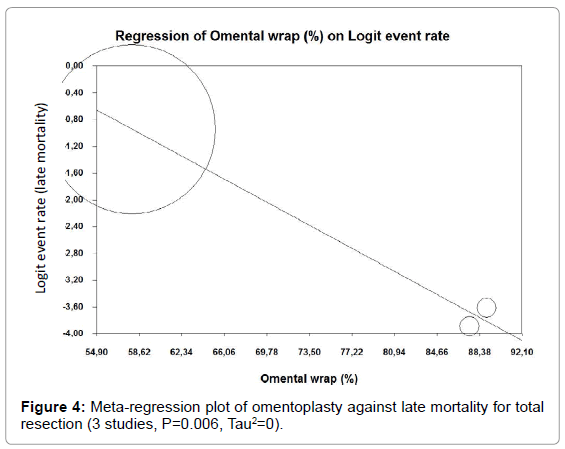
Figure 4: Meta-regression plot of omentoplasty against late mortality for total resection (3 studies, P=0.006, Tau2=0).
Reinfection: Separate sets of data were available for 16 studies (808 patients), with inter-study heterogeneity (I2=69.7%, PHET =0). According to the random-effects method, the reinfection rate was 6.4%; 95% CI: 3.4%-11.7%. A publication bias was identified by Egger’s regression test. However, six studies were missing, identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted reinfection rate: 11%; 95% CI: 6%-19% (Table 1). In a meta-regression analysis (Table 3), patient age (P=0), presence of PDF (P=0.002), and virulent infectious organisms (P=0.001) had a negative correlation with reinfection (Figures 5-7), whereas nonvirulent infectious organisms (P=0), had a positive correlation (Figure 8).
| Event | Variables | group | Study N | Slope | Slope 95 % IC | p-value | T2 |
|---|---|---|---|---|---|---|---|
| Reinfection | Age | TR | 11 | 0.29 | 0.12-0.46 | 0 | 0.75 |
| PR | 4 | 0.16 | -0.38 | 0.095 | 1.76 | ||
| TR | 11 | 0.04 | -0.07 | 0.002 | 0.85 | ||
| PR | 4 | 0.07 | 0.01-0.13 | 0.01 | 0 | ||
| Virulent | TR | 11 | 0.06 | 0.02-0.10 | 0.001 | 1.24 | |
| PR | 5 | -0.00009 | -0.36 | 0.99 | 0 | ||
| Non Virulent | TR | 10 | -0.09 | -0.08 | 0 | 0.33 | |
| PR | 3 | -0.02 | -1.59 | 0.95 | 0 | ||
| Amputation | TR | 11 | 0.02 | 0.00-0.05 | 0.042 | 0.28 | |
| PRp | 3 | 0.02 | -0.18 | 0.66 | 0.09 | ||
| Follow-up | PR | 11 | 0.04 | 0.01-0.06 | 0.006 | 0.15 | |
| 4 | -0.02 | -0.17 | 0.57 | 0 | |||
| % male | 11 | -0.04 | 0.08-(-0.005) | 0.026 | 0.32 | ||
| 3 | 0.05 | -0.22 | 0.34 | 0 |
TR: Total Resection; PR: Partial Resection, PDF: prosthetic-duodenal fistula, % male: male gender.
Table 3: Meta-Regression Analysis of the Risk of Reinfection and Amputation According to Age, PDF, Virulent or Nonvirulent Infecting Organisms, Follow-up and Male gender
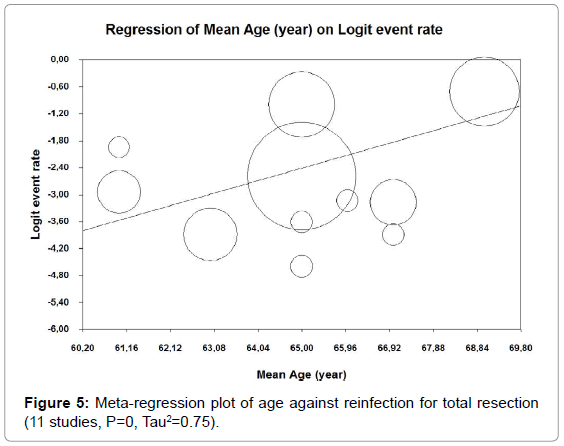
Figure 5: Meta-regression plot of age against reinfection for total resection (11 studies, P=0, Tau2=0.75).
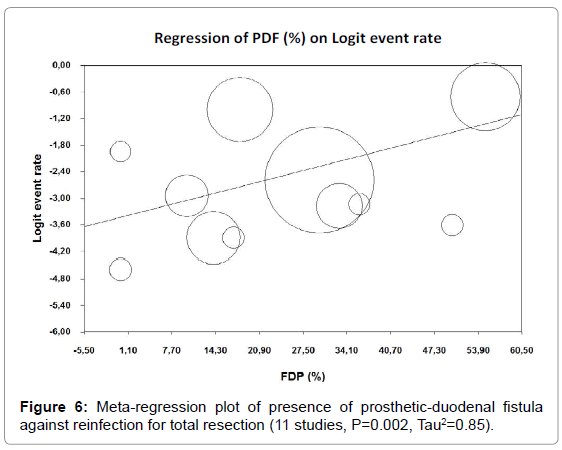
Figure 6: Meta-regression plot of presence of prosthetic-duodenal fistula against reinfection for total resection (11 studies, P=0.002, Tau2=0.85).
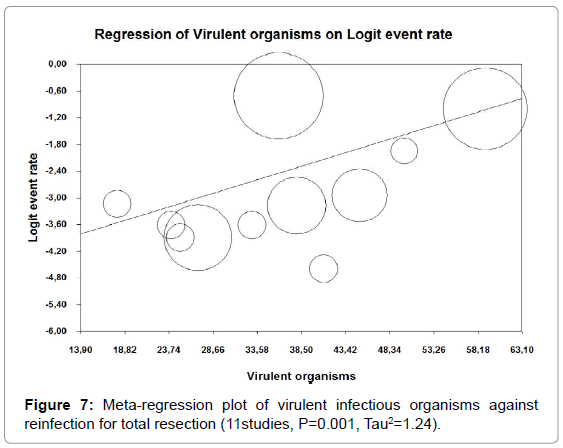
Figure 7: Meta-regression plot of virulent infectious organisms against reinfection for total resection (11studies, P=0.001, Tau2=1.24).
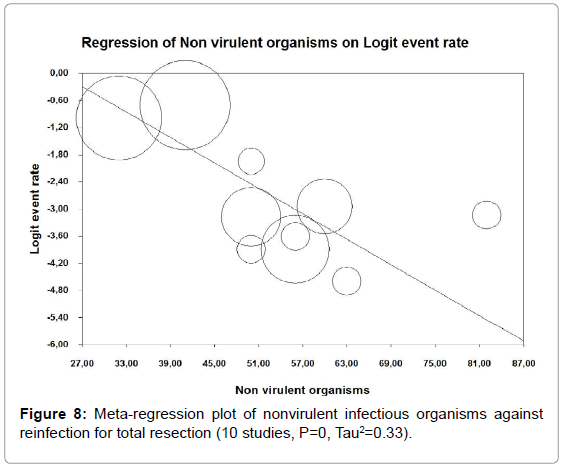
Figure 8: Meta-regression plot of nonvirulent infectious organisms against reinfection for total resection (10 studies, P=0, Tau2=0.33).
Amputation: Separate sets of data were available for 14 studies (660 patients), with no inter-study heterogeneity (I2=29.7%, PHET =0.14). According to the fixed-effects method, amputation rate was 6.8%; 95% CI: 4.8%-9.5%. A publication bias was identified by Egger’s regression test. However, six studies were missing, identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted amputation rate: 8.1%; 95% CI: 6%-11%, (Table 1). In a metaregression analysis, (Table 3), presence of PDF (P=0.042), and length of follow-up (P=0.006) (Figure 9), both had a negative correlation with amputation, whereas male prevalence (P=0.026), had a positive correlation.
Outcomes after partial resection
Early mortality: Separate sets of data were available for 6 studies (68 patients), with no inter-study heterogeneity (I2=0%, PHET=0.8). According to the fixed-effects method, the operative mortality rate was 7.3%; 95% CI: 2.7%-18%. No publication bias was identified by Egger’s regression test. However, 2 studies were missing, identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted operative mortality rate: 10.5%; 95% CI: 4%-22%, (Table 4). In a meta-regression analysis (Table 2), there was no analyzable correlation between the variables considered (P>0.05).
| No of trials analysis | I2 statistic | P for heter ogeneity |
Method (fixed or Random-effects Model) |
Event Rate | IC Event Rate | |
|---|---|---|---|---|---|---|
| Random model if heterogeneity test is significant or fixed model if not | ||||||
| Operative mortality | 6 | 0 | 0.8 | Fixed | 0.073 | 0.027-0.18 |
| Reinfection | 10 | 69.1 | 0.001 | Random | 0.189 | 0.081-0.383 |
| Amputation | 7 | 0 | 0.67 | Fixed | 0.095 | 0.041-0.206 |
| Late mortality | 5 | 0 | 0.64 | Fixed | 0.162 | 0.079-0.305 |
| Event rates after corrections of selection bias (Dural and test is trim and fill) | ||||||
| Operative mortality | 0.105 | 0.04-0.22 | ||||
| Reinfection | 0.27 | 0.12-0.50 | ||||
| Amputation | 0.154 | 0.08-0.29 | ||||
| Late mortality | 0.18 | 0.09-0.32 | ||||
Table 4: Meta-analysis and Heterogeneity Tests of the Results for Partial Resection.
Late mortality: Separate sets of data were available for 5 studies (49 patients), with no inter-study heterogeneity (I2=0, PHET=0.64). According to the fixed-effects method, the late mortality rate was 16.2%; 95% CI: 7.9%-30.5%. No publication bias was identified by Egger’s regression test. However, 1 study was missing identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included this study as a measure of conservation for the assessment of the adjusted late mortality rate: 18%; 95% CI: 9%-32%, (Table 4). In a meta-regression analysis (Table 2), there was no analyzable correlation between the variables considered (P>0.05).
Reinfection: Separate sets of data were available for 10 studies (165 patients), with inter-study heterogeneity (I2=69.1%, PHET=0.001). According to the random-effects method, the reinfection rate was 18.9%; 95% CI: 8.1%-38.3%. No publication bias was identified by Egger’s regression test. However, 3 studies were missing identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted reinfection rate: 27%; 95% CI: 12%-50%, (Table 4). In a meta-regression analysis (Table 3), only the presence of PDF (P=0.01) had a negative correlation with reinfection (Figure 10).
Amputation: Separate sets of data were available for 7 studies (74 patients), with no inter-study heterogeneity (I2=0%, PHET=0.67). According to the fixed-effects method, the amputation rate was 9.5%; 95% CI: 4.1%-20.6%. A publication bias was identified by Egger’s regression test. However, 3 studies were missing, identified by Duval and Tweedie’s trim and fill method. To correct this bias, we have included these studies as a measure of conservation for the assessment of the adjusted amputation rate: 15.4%; 95% CI: 8%-29%, (Table 4). In a meta-regression analysis (Table 3), there was no analyzable correlation with the variables considered (P>0.05).
Outcomes after in situ reconstruction according to the nature of the conduit
Meta-analysis was only feasible for the groups with at least 4 studies, and therefore only for TR and ISR with cryopreserved allografts and autogenous femoral veins (Table 5).
| Group | No of trials analysis |
I² statistic | P for heter- ogeneity |
Method fixed or random – effects model |
Event rate | IC event rate | |
|---|---|---|---|---|---|---|---|
| Random model if heterogeneity test is significant of fixed model if not | |||||||
| Operative mortality | Allograft | 5 | 76.5 | 0.001 | Random | 0.182 | 0.112-0.281 |
| Fem vein | 4 | 48 | 0.123 | Fixed | 0.102 | 0.07-0.148 | |
| Reinfection | Allograft | 5 | 76.2 | 0.002 | Random | 0.058 | 0.019-0.167 |
| Fem Vein | 4 | 0 | 0.515 | Fixed | 0.028 | 0.013-0.061 | |
| Amputation | Allograft | 5 | 26.4 | 0.245 | Fixed | 0.047 | 0.024-0.089 |
| Fem vein | 4 | 0 | 0.598 | Fixed | 0.061 | 0.037-0.10 | |
| Late mortality | Allograft | 6 | 32 | 0.196 | Fixed | 0.258 | 0.22-0.30 |
| Fem vein | 4 | 45.7 | 0.158 | Random | 0.315 | 0.215-0.435 | |
| Event rates after correction of selection bias (dural and Tweedie’s trim and Fill) | |||||||
| Operative mortality | Allograft | 0.23 | 0.14-0.34 | ||||
| Fem vein | 0.107 | 0.075-0.15 | |||||
| Reinfection | Allograft | 0.105 | 0.035-.028 | ||||
| Fem vein | 0 trimmed study | 0.028 | 0.013-0.061 | ||||
| Amputation | Allograft | 0.06 | 0.03-0.11 | ||||
| Fem vein | 0.066 | 0.04-0.107 | |||||
| Late mortality | Allograft | 0.26 | 0.22-0.30 | ||||
| Fem vein | 0.32 | 0.23-0.43 | |||||
Table 5: Meta-analysis and Heterogeneity Tests of the results for total resection and in situ reconstructions with allografts and femoral veins.
Early mortality
For allografts: Separate sets of data were available for 5 studies (481 patients), with inter-study heterogeneity (I2=76.5%, PHET=0.001). According to the random-effects method, the early mortality rate was 18.2%; (95%CI: 0.112-0.281). A publication bias was identified by Egger’s regression test. However, 2 studies were missing, and we have included these studies for the assessment of the adjusted early mortality rate: 23%; 95% CI: 14%-34%.
For femoral veins: Separate sets of data were available for 4 studies (251 patients), with no inter-study heterogeneity (I2= 48%, PHET=0.123). According to the fixed-effects method, the early mortality rate was 10.2%; (95 % CI: 0.07-0.148). A publication bias was identified, 1 study was missing, and the adjusted early mortality rate was: 10.7%; 95% CI: 7.5%-15%.
Late mortality
For allografts: Separate sets of data were available for 6 studies (481 patients), with no inter-study heterogeneity (I2=32%, PHET=0.196). According to the fixed-effects method, the late mortality rate was 25.8%; (95% CI: 22%-30%). A publication bias was identified, 2 studies were missing, and the adjusted late mortality rate was: 26%; 95% CI: 22%-30%.
For femoral veins: Separate sets of data were available for 4 studies (251 patients), with inter-study heterogeneity (I2=45.7%, PHET=0.158). According to the random-effects method, the late mortality rate was 31.5%; (95% CI: 21.5%-43.5%). A publication bias was identified, 1 study was missing, and the adjusted late mortality rate was: 32%; 95% CI: 23%-43%.
Reinfection
For allografts: Separate sets of data were available for 5 studies (413 patients), with inter-study heterogeneity (I2=76.2%, PHET= 0.002). According to the random-effects method, the reinfection rate was 5.8%; (95% CI: 1.9%- 16.7%). A publication bias was identified, 2 studies were missing, and the adjusted reinfection rate was: 10.5%; 95% CI: 3.5%-28%.
For femoral veins: Separate sets of data were available for 4 studies (251 patients), with no inter-study heterogeneity (I2=0, PHET=0.515). According to the fixed-effects method, the reinfection rate was 2.8%; 95% CI: 1.3%-6.1%. 0 studies were trimmed.
Amputation
For allografts: Separate sets of data were available for 5 studies (332 patients), with no inter-study heterogeneity (I2=26.4%, PHET=0.245). According to the fixed-effects method, the amputation rate was 4.7%; (95% CI: 2.4%-8.9%). A publication bias was identified, 2 studies were missing, and the adjusted amputation rate was: 6%; 95% CI: 3%-11%.
For femoral veins: Separate sets of data were available for 4 studies (251 patients), with no inter-study heterogeneity (I2= 0, PHET=0.598). According to the fixed-effects method, the amputation rate was 6.1%; (95% CI: 3.7%-10%). A publication bias was identified, 1 study was missing, and the adjusted amputation rate was: 6.6%; 95% CI: 4%- 10.7%.
Treatment for AGI is still very much under discussion, and optimal management of patients with aortic graft infections requires a full understanding of all potential therapeutic interventions available. Miller [43] was one of the first to introduce the concept of partial aortic graft removal, and thereby challenged the paradigm of entire aortic graft excision: partial graft removal was accomplished in 10 infected aortic graft with a 13% early mortality rate, and 33% persistent infection. On the other hand, in a recent meta-analysis with 80% total resection [13] early mortality, reinfection and amputation had a rate of 17%, 10%, and 8% respectively.
The results from the present meta-analysis are summarized in Tables 1,4 and 5: early/late mortality, reinfection and amputation rates for TR and PR are 16.8% and 10.5%, 28.5% and 18%, 11% and 27%, and 8.1% and 15.4% respectively, and according to the nature of the conduit for ISR are, for allografts and femoral veins, 23% and 10.7%, 26% and 32%, 10.5% and 2.8%, 6% and 6.6% respectively. They are similar to the literature results [11,13]. This retrospectively validates the methodology used for this study. However, statistical comparison with TR and PR must be weighted with the limitations of meta-analysis and interpreted with caution (see below).
Perhaps the most difficult aspect of managing AGI is deciding on the appropriate treatment for any given patient. Regarding the manifestations of the patients concerned, most authorities agree that TR is mandatory for intra-cavitary AGI in patients with favorable conditions [12,19-21] but there is an increasing number of patients with severe comorbidities and for whom this approach would be inappropriate and even ill-advised, resulting in a prohibitive mortality rate. Thus, it was suggested that the premise of a more limited aortic reconstruction might benefit the patient by avoiding aortic clampage, reducing physiological stress, and limiting the extent of dissection needed to excise the entire graft. On the other hand, concerning the extent of AGI, numerous authors [36-39,41-43] agree that for pangraft infection TR is the most advisable, and when AGI is localized, PR appears recommendable [17,18]. However, there are numerous other clinical scenarios where optimal treatment is not clearly defined. To make the most appropriate decision, evaluation of outcomes in each situation may be helpful.
Early and late mortality
In the meta-analysis, operative mortality rates were higher for TR than PR, with 16.8% and 10.5% respectively (Tables 1 and 4). Concerning the nature of the conduit, they were higher for allografts than for femoral veins, with 23% and 10.7% respectively (Table 5). The higher rate of mortality observed probably depends on patient status [10].
In the literature review, urgency of the intervention for AGI is one of the most important determinants of in-hospital mortality [8,11,22,38,44-49]. Patients can be categorized into those who need emergency surgery to control bleeding or sepsis, and those who do not require emergency surgery. Not surprisingly, in the meta-regression analysis (Table 2), urgency had a negative correlation with operative mortality for TR (Figure 1), but no correlation was analyzable for PR. Hence, in order to lower operative mortality in an emergency situation, there may be fewer surgical options available for patients who cannot be stabilized long enough to select the most appropriate surgical option. In this difficult situation, endovascular bridge therapy might be the only realistic option [12,22,50-52].
Male gender was prevalent in this study with rates ranging from 62% to 100% (Supplementary, Online Appendix E). In the metaregression (Table 2), male gender had a negative correlation with operative mortality for TR (Figure 2), but no correlation was analyzable for Pr. Oderich suggests that female gender was an independent predictor for operative mortality [22]. On the contrary, in the results of the present study, the higher operative mortality rate observed in males is probably related to the epidemiology of cardiovascular disease and the prevalence of cardiovascular risks in males [53].
In 1987, Walker was one of the first to propose omentoplasty for protection against reinfection [54] and its benefits were confirmed by numerous studies for both TR and PR [8,10,12,17,35,52]. In the metaregression (Table 2), the negative correlation between omentoplasty and operative mortality is not clear (Figure 3), because omentoplasty is considered a safe procedure, associated with a moderate number of post-operative complications [55]. In our opinion, such discrepancy could only be explained by the differences amongst patients undergoing surgical procedures, particularly any underlying diseases.
In the meta-analysis, late mortality rates were higher for TR than for PR with 28.5% and 18% respectively (Tables 1 and 4), and in the meta-regression, omentoplasty had a positive correlation with late mortality for TR (Figure 4), although no correlation was analyzable for PR (Table 2). Such benefits for patients with omentoplasty are probably linked to the decrease in late infectious mortality caused by dehiscence of anastomosis and fatal hemorrhage.
Reinfection and amputation
In the results of the meta-analysis reinfection rates were higher for PR than for TR, with 27% and 11% respectively (Tables 1 and 4) and concerning the nature of the conduit they were higher for allografts than femoral veins, with 10.5% and 2.8% respectively (Table 5). These last results are similar to those of a recent meta-analysis [13].
To prevent reinfection, instinct suggests removal an infected graft in its entirety rather than partial excision. The literature supports the idea that complete graft excision minimizes the risk of reinfection: Ricotta reported persistent or recurrent infection in 25% of the grafts treated with PR but no reinfection after TR [56]. However, TR does not absolutely prevent the development of recurrent infection, and Batt reported 60% reinfection after PR and 20% after TR [40]. Because of the risk of reinfection, no form of treatment for vascular graft infection can ever be considered definitive.
The literature suggests a link between reinfection and patient age [9,10,57] presence of PDF [9,11,45,46,58] and virulent [9,18,30,41,46,59-61] or nonvirulent [59,62-64] infecting organisms. In the meta-regression (Table 3), age and virulent organisms had a negative correlation with reinfection for TR (Figure 5 and 7), nonvirulent organisms had a positive correlation for TR (Figure 8), and PDF had a negative correlation for TR and PR (Figures 6 and 10). The results of the present study suggest that in order to lower reinfection rates in the presence of nonvirulent organisms, TR appears optimal. In the presence of PDF, neither TR nor PR was advisable. However, for the patients who do not required emergency surgery it was suggested that ISR with autogenous femoral veins [45,65,66] or silver/rifampicin polyesters and cryopreserved allografts [8,13] with omental wrapping [22,45,54] may achieved the best results. For older patients and in the presence of virulent organisms fewer surgical options may have been available because TR was not recommendable and PR had no analyzable correlation. Thus, in the presence of virulent organisms, if the patient is hemodynamically stable and not septic, it has been suggested that percutaneous drainage of peri-aortic abscesses or fluid collections, and intensive treatment of infection or comorbidities could be done before more extensive operation [67] and consequently, extra-anatomic reconstruction [22] or in situ reconstruction [11,13] may be the most appropriate. The results of this study (Table 5) and those of the literature review [11,13] suggested that femoral vein for ISR seems to be the most optimal option for virulent organisms.
Omentoplasty was recommended to lower reinfection rates [8,10,12,17,22,29,35,53]. Unfortunately, in the present study, no correlation was analyzable. However, omentoplasty is not always feasible, for instance in the event of extra-cavitary graft infection or a retroperitoneal approach [17,18].
In the results of the meta-analysis, amputation rates were higher for PR than for TR, with 15.4% and 8.1% respectively (Tables 1 and 4). Unsurprisingly, in the meta-regression (Table 3), amongst the population of patients with vascular risks, follow-up had a negative correlation with amputation for TR (Figure 9), and the results for PR were not analyzable. The nature of the conduit was probably the major factor [11,13] but in this study, amputation rates were similar for allografts and femoral veins (Table 5).
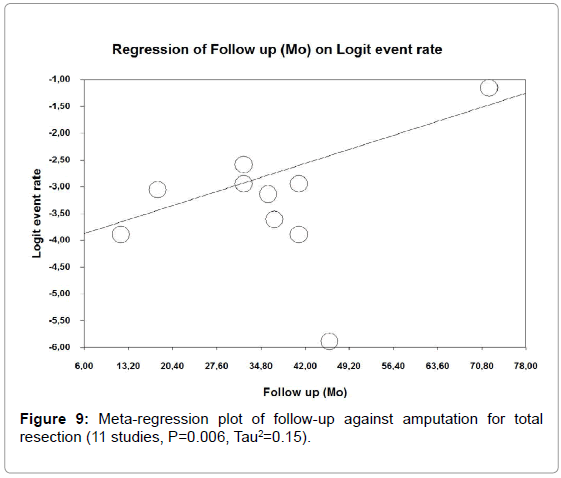
Figure 9: Meta-regression plot of follow-up against amputation for total resection (11 studies, P=0.006, Tau2=0.15).
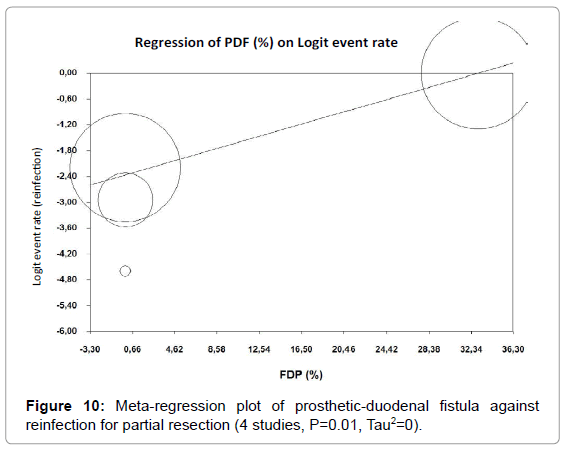
Figure 10: Meta-regression plot of prosthetic-duodenal fistula against reinfection for partial resection (4 studies, P=0.01, Tau2=0).
This meta-analysis is the first report to offer indications for PR or TR of infected aortic graft according to patient manifestations and the bacteriology data. Unfortunately, the observational studies used in this meta-analysis were difficult to analyze and interpret because the discrepancy between patient numbers in each group (887 TR vs 165 PR) caused a problem for statistical comparison. This drawback was owing to the lack of standardized indications for TR or PR in the series, and not this meta- analysis. However, for TR, the optimal strategy could be monitored with matching events and variables. In order to lower operative mortality rates, total removal of the infected aortic graft is probably not the most recommendable indication in urgent cases, and an alternative intervention (endovascular bridge therapy) is perhaps more advisable before a secondary extensive operation. In order to lower reinfection rates, TR is recommendable for nonvirulent infecting organisms. For older patients, in the presence of virulent organisms, and in stable conditions, it is conceivable that priority was given to intensive treatment of infection and comorbidities before resection of the infected aortic graft and more extensive intervention.
Finally, management of AGI is clearly not easy, and is still under discussion. In order to define an optimal strategy, decisions must be tailored following the input of all clinicians involved, i.e. vascular surgeon, microbiologist/infectious disease physician, interventional and imagist radiologist and others, taking due cognizance of the individual patient’s condition and state [12,68-72]. Moreover, operative flexibility is required should unexpected difficulties arise during the intervention.
Study Limitations
Some limitations, mostly related to potential bias, are encountered in this meta-analysis:
Studies selection bias: The selection process for publications, notably the manner in which we pooled the data from individual studies, may be a source of bias. Inclusion/exclusion criteria were defined in attempt to limit selection bias. For example, infected aortic aneurysms were excluded because, etiology, bacteriology and treatment results are different from those of AGI [12,46,73], and the series combining total and partial removal of infected aortic grafts were excluded if the results were not differentiated. On the other hand, our inclusion/exclusion criteria may have biased the outcome of the metaanalysis. For example, we only considered clinical studies whose results were reported in the English language. Hence, results extracted from medical journals in languages other than English were excluded. We believe that publication bias was limited by the use of the Funnel plots and complementarity validation tests.
Outcome reporting bias: Nearly all studies analyzed were retrospective and observational. Consequently, there are problems concerning inter-study heterogeneity and selection bias [74] despite reasonable efforts to perform tests of heterogeneity (Tables 1 and 4).
It is possible that some significant medical considerations were not available in a number of studies. These include, cigarette smoking (not reported in the majority of the series) which is associated with increased surgical risk of site infection [75] time to clinical presentation of the infection divided into early and late presentation (<3months or after 3 months) [16] infection presented, and specific information on the pre-operative status of the patients: coronary heart disease, HTA, diabetes mellitus, renal failure, chronic obstructive pulmonary disease, ASA score, immunosuppression, history of neoplasm, body mass index [76] anatomic considerations (hostile abdomens, poor pelvic collateral blood supply, tight attachment of the infected graft to the iliac vessels and the ureter, aortic graft involving the renal or visceral aortic segment), and so forth. These risks of bias across the studies create reservations regarding the comparison of outcomes after TR and PR [26]. For example, partial graft removal of the infected aortic graft was probably performed in a group of patients who have a more significant operative risk compared to those who underwent total graft removal, but these differences, despite reasonable efforts, cannot be shown in the different studies. This drawback concerns the reported studies themselves and not this meta-analysis.
There is also a possibility that some specific aspects of treatment were not available, yet had an impact on perioperative outcomes: drainage of peri-prosthetic abscesses, use of Sartorius flap [14] or Vacuum- assisted closure device, the experience of each center (number of patients treated per year for AGI), lack of consensus concerning the nature and duration of postoperative antibiotherapy [77] and so forth.
As a result, the eligible sample size for analysis was considerably reduced. However, this drawback concerns the reported studies themselves and not this meta-analysis.
Limits of meta-regression: The associations derived from meta regression are observational and have a weaker interpretation than the causal relationships derived from randomized comparisons. Data dredging is the main pitfall in reaching reliable conclusions from metaregression, and pre-specification of covariates is heightened. Therefore, special attention was paid to selected relevant covariates in this study. For instance, the nature of the conduit has an impact on operative outcomes [11,13] but these differences could not be captured in the present meta-analysis owing to heterogeneity between PR and TR.
The results of this meta-analysis suggest that operative mortality rates are higher for TR than for PR, and reinfection rates are higher for PR than for TR.
For TR, the rate of operative mortality increases in males, and in urgent cases, total removal of the infected aortic graft seems inadvisable. Alternative interventions should be considered. Regarding the risk of reinfection, TR seems recommendable in the presence of nonvirulent infectious organisms. The risk increases in the presence of virulent organisms and PDF, and other optimal options may be discussed.
For PR results were not analyzable except for a negative correlation in the presence of PDF.