Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 3
Neuropsychiatric manifestations are well known to occur in thyrotoxicosis. In many cases, these manifestations occur in conjunction with the systemic features of the disease, but may be the presenting symptom in some patients. We report on an elderly gentleman with, neuropsychiatric manifestations and thyrotoxicosis in the background of lithium toxicity who presented as a diagnostic dilemma.
Case report: A-70 year old man awaiting coronary artery bypass graft was detected to have thyrotoxicosis with FT4 of 2.7 ng/l(0.7-1.8) and TSH levels of 0.03 μIU/mL (0.4-4.3). A Tc 99 thyroid scan showed <1% iodine uptake suggestive of thyroiditis. He had no prior history of thyroid disorders, but has had a recent coronary angiogram. He was commenced on thioamides, lithium and small doses of prednisolone. One week after initiation of medication he presented with ataxia, dysarthria, choreiform movements and altered level of consciousness following a bout of diarrhea and vomiting and was found to have elevated levels of lithium 2.57 mmol/l(0.6-1.2) with serum creatinine of 219 µmol/l(80-120). In spite of adequate hydration, hemodialysis and normalization of lithium levels he did not show any clinical improvement. Blood and cerebrospinal fluid analysis for a possible infectious etiology were negative. This prompted an alternative diagnosis of Hashimoto’s encephalopathy (HE). Treatment with high doses of steroids led to a remarkable clinical resolution. HE also known as steroid responsive encephalopathy associated with autoimmune thyroiditis is an autoimmune thyroid disease with neuropsychiatric manifestations. Although almost all cases of HE have positive thyroid antibodies, these were repeatedly negative in our patient.
This case posed a diagnostic challenge in differentiating between acute lithium toxicity and thyroiditis with encephalopathy. The dramatic response to high dose steroids in the presence of negative thyroid antibody highlights the possible rare existence of an antibody negative steroid responsive encephalopathy associated with thyroiditis.
<Cognitive impairment is common in hyperthyroidism and may present as one or more different syndromes. Patients may experience behavioral and personality changes, such as psychosis, agitation, and depression. Tremor and hyperreflexia with other pyramidal tract signs are also common features of the neurologic examination in thyrotoxicosis [1]. Elderly patients may have a less activated presentation with depression and lethargy, so-called apathetic thyrotoxicosis [2].
We report on an elderly gentleman who presented acutely with neurological manifestations and lithium toxicity in a background of thyrotoxicosis who presented as a diagnostic dilemma.
Our patient was a-70 year old man with type 2 diabetes mellitus, hypertension who suffered a recent non ST elevation myocardial infarction for which he underwent coronary angiogram. He was planned for a coronary artery bypass graft (CABG). He had never been on amiodarone. Preoperative investigations revealed thyrotoxicosis with FT4 of 2.7 ng/l(0.7-1.8) and TSH levels of 0.03 μIU/mL(0.4-4.3) though clinically euthyroid without a goiter. A Tc99 thyroid scan revealed grossly impaired overall tracer trapping (Figure 1). CABG was postponed and he was started on carbimazole 15mg tds. Due to inadequate response, lithium 500 mg tds was commenced along with a small dose of prednisolone. One week afterwards he presented with unsteadiness of gait, slurring of speech, agitation, altered level of consciousness and reduced urine output. Prior to these symptoms he had experienced vomiting and diarrhea. There was no history of fever, septic foci, acute onset limb weakness or seizures.
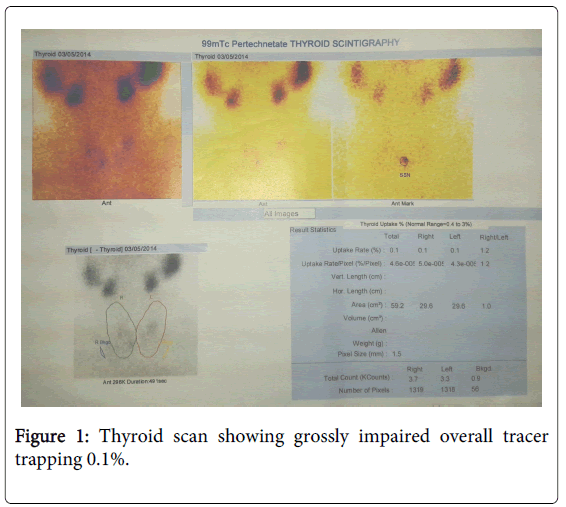
Figure 1: Thyroid scan showing grossly impaired overall tracer trapping 0.1%.
On examination he was afebrile, agitated with a GCS of 10/15. Choreiform movements involving face, and upper limbs were noted. There was no neck stiffness and he was moderately dehydrated. He had a regular pulse rate of 104/min with blood pressure of 120/70 mmHg. Neurological examination revealed increased tone in all four limbs with exaggerated reflexes and bilateral extensor plantar responses.
Investigations revealed elevated level of lithium 2.57 mmol/l (0.6-1.2) with serum creatinin of 219 µmol/l(80-120) and normal electrolytes. Full blood count was significant for mild neutrophil leukocytosis with a total WBC of 13,500 and 85% of neutrophils. Hemoglobin and platelet were normal as were the blood sugar and liver function tests. FT4 was elevated at 2.5 ng/dl with TSH of 0.025 μIU/mL. C reactive protein was 12 mg/l (<6) and ESR was 60mm in the 1st hour. MRI scan of the brain revealed chronic small vessel disease without acute changes. Cerebrospinal fluid(CSF) full report was normal and negative for viral studies inclusive of cytomegalovirus, japanese encephalitis and herpes simplex virus. Cultures of CSF, blood and urine were all sterile. EEG showed non specific generalized delta activity.
An initial working diagnosis was lithium toxicity with possible meningoencephalitis in the back ground of thyrotoxicosis. Lithium was omitted and the patient was hydrated and dialysed. Intravenous ceftriaxone and acyclovir for a possible meningoencephalitis was commenced. Carbimazole was continued. There was no neurological improvement following hemodialysis and normalization of lithium levels and renal functions. This prompted consideration of any alternative diagnosis such as Hashimoto’s encephalopathy and oral prednisolone 60mg/day was initiated. Thyroid auto antibodies inclusive of thyroglobulin antibodies and thyroid peroxidase antibodies were twice negative. He made a remarkable neurological improvement within 5 days of commencement of steroids and was discharged following 2 weeks of hospital stay. It was planned to tail off the steroids and titrate antithyroid drugs.
Our patient’ s clinical presentation with elevated lithium levels suggest a diagnosis of lithium toxicity precipitated by diarrhea and vomiting causing added insult on an already damaged kidney due to long standing diabetes. Lithium is a drug with a narrow therapeutic range and elderly patients are especially at risk of toxicity due to both a lower glomerular filtration rate and a reduced volume of distribution. Potential neurologic symptoms and signs include sluggishness, ataxia, confusion or agitation, and neuromuscular excitability, which can manifest as irregular coarse tremors, fasciculations, or myoclonic jerks. Severe lithium intoxication can lead to seizures, nonconvulsive status epilepticus, and encephalopathy. Treatment of acute lithium toxicity is with hydration and hemodialysis if indicated. Indications for hemodialysis are lithium levels >4 meq/l or levels >2.5 meq/l with significant signs of lithium toxicity (eg, seizures, depressed mental status), has renal insufficiency or other conditions that limit lithium excretion [3]. The latter was the case in our patient. In some cases, neurologic complications persist despite lithium removal by hemodialysis. The syndrome of irreversible lithium effectuated neurotoxicity (SILENT) consists of prolonged neurologic and neuropsychiatric symptoms following lithium toxicity [4]. In typical cases of SILENT, neurologic toxicity develops along with an elevated lithium concentration, but symptoms persist despite successful removal of the drug. The condition is diagnosed if the neurological symptoms persist for more than two months after cessation of Lithium. The pathogenesis of this condition is unclear and no effective treatment is known.
The failure of clinical resolution following successful elimination of Lithium prompted us to consider other possible diagnoses. The recent onset of thyrotoxicosis with grossly impaired tracer uptake in the Tc99 scan suggested thyroiditis or low uptake due to iodine rich contrast following recent coronary angiogram. Usually a single iodine load may transiently reduce the radioiodine uptake in patients with Graves’ disease or toxic nodular goiter to less than 10% for up to two to four weeks, but rarely reduces the uptake to less than 1% as occurs in patients with painless thyroiditis. A continuous iodine load, however, may reduce the uptake to less than 1% [5]. Our patient had a single exposure to iodinated contrast in coronary angiogram and was not exposed to continuous exogenous iodine load such as amiodarone. The tracer trapping was 0.1% and pointed towards a diagnosis of thyroiditis rather than iodine induced low uptake.
Our patient’s thyroiditis with neurological sequel which responded dramatically to high doses of steroids highlighted the possibility of a Hashimoto’s encephalopathy. Encephalopathy associated with autoimmune thyroid disease (EAATD), first described in 1966 by Brain and colleagues, is a rare condition presenting in the setting of autoimmune thyroid disease and characterized by neurological and/or psychiatric symptoms [6]. Thyroid status varies among patients with reported Hashimotos encephalopathy, ranging from overt hypothyroidism to overt hyperthyroidism Majority are associated with Hashimoto's thyroiditis, but recently shown to occur in patients with Graves' disease [7]. Recently, the term steroid responsive encephalopathy associated with autoimmune thyroiditis (SREAT) has been suggested to highlight steroid responsiveness. These conditions are diagnosed with the suggestive clinical picture, thyroid antibody positivity; exclusion of other similar conditions especially infections and rapid responsiveness to steroids. Infections need to be excluded as there will be flare ups when treated with high doses of immunosuppressants. C-reactive protein and the erythrocyte sedimentation rate are elevated in some patients even in the absence of infections [8]. This was the case in our patient as well. Thyroid antibodies are positive in almost all patients with Hashimoto’s encephalopathy [9]. However these performed twice in our patient were found to be negative. The compatible clinical picture with thyroiditis and the rapid resolution to steroids highlights the possibility of a rare existence of an antibody negative thyroiditis with encephalopathy responsive to steroids.
Neurological manifestations associated with thyrotoxicosis are well known. This case highlights a patient who presented with predominant neurological features and lithium toxicity in the background of biochemical thyrotoxicosis with thyroiditis. Failure of clinical resolution despite adequate control of lithium levels prompted the search for another etiology. The dramatic response to high dose steroids in the presence of negative thyroid antibody highlights the possibility of a rare existence of antibody negative steroid responsive encephalopathy associated with thyroiditis.