Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2014) Volume 1, Issue 3
Keywords: Non-medical prescribing; Pharmacy; Pharmacist prescribing; Safe prescribing; Appropriate prescribing
Inappropriate prescribing is the failure to provide the quality of care related to medication use that should be achieved in practice, and encompasses overprescribing, misprescribing, and under prescribing [1]. Inappropriate medicine use has been defined as that which poses greater risk of harms than benefits, especially when safer alternatives exist [2]. Elderly patients, in particular, are susceptible to the consequences of inappropriate prescribing, increasing the risk of adverse drug events and related morbidity and hospitalisations [3,4]. Patients recently discharged from hospital are also at increased risk of medication misadventure, as medication is often reviewed and changed during an admission, and poorly communicated with community practitioners [5]. The importance of accurate transfer of information across the whole surgical care pathway from preadmission to discharge, including information about medications, was highlighted in a study that reported communication failures led to patient morbidity and mortality [6]. The Australian Commission on Quality and Safety in Health Care has highlighted medication reconciliation, and the accurate transfer of information about medication as a national priority [7].
Within hospital, the medication chart provides a record of patient’s medication, instructions for safe medication supply and administration, and ensures patient access to medications as an inpatient. It is a communication tool between doctors, pharmacists and nurses about prescribing decisions, and is used as the primary source of information regarding medications, both during the inpatient stay and on discharge. An appropriate and accurate medication chart is essential, and unless prescribing errors are found and corrected early, they can lead to errors in supply and administration [8].
Pre admission clinic (PAC) at Princess Alexandra Hospital (PAH) is a multidisciplinary clinic, comprising of nurse, Resident Medical Officer (RMO), pharmacy and anaesthetic review. The pharmacy service in PAC was initiated in 1998, with the aim of improvement in the accuracy of information exchange as patients cross healthcare setting [9]. The benefits of pharmacy involvement in PAC on medication management and information transfer prior to admission and on discharge, and the associated risks of omissions of medications at these times, were highlighted as part of a randomised controlled trial [10]. Pharmacy in PAC is now a well-recognised role in Australia, with the Society of Hospital Pharmacists of Australia (SHPA) publishing a fact sheet on how pharmacists in PAC can contribute to better patient outcomes and quality of care [11].
Several countries have extended the prescribing of prescription only medicines to health care professionals other than doctors, with the aim of increasing patients’ access and choice, and make best use of health professionals’ skills, whilst ensuring patient safety [12]. Health Workforce Australia has highlighted possible models of prescribing for non-medical health professionals within the Australian healthcare system [13,14]. However, there is a lack of evidence to support this model of care. Current literature is predominantly qualitative, with little in the way of evaluation of quality, safety or appropriateness of prescribing. A recent review suggested that acceptance of the model of care was mainly based on the perceived value to the healthcare system [15].
To use a validated national health performance framework to compare a collaborative pharmacist prescribing model with usual care, with regards to effectiveness (incorporating appropriateness), safety, responsiveness, continuity, accessibility and efficiency [16]. The hypothesis was that no difference exists between the models of care. Results so far have shown pharmacist prescribing is as good as usual care in safety and accuracy of medication charts, and appropriateness of venous thromboembolism (VTE) prophylaxis [17].
The significant difference in omissions of medications prompted further investigation in to the appropriateness of prescribing, and the significance of medications that had not been prescribed on to the National Inpatient Medication Chart (NIMC). The aim of the data discussed in this paper to assess a ‘snapshot’ of the appropriateness of prescribing from a pilot study, and the potential health impact or ward inconvenience of omissions from the NIMC. If the methodology utilised in the pilot proves feasible and yields meaningful data, this study will provide guidance for future assessments of appropriateness of prescribing from collaborative non-medical prescribing studies. Ethics approval was obtained from the PAH Human Research Ethics Committee.
The main study was conducted between June to September 2009 in the surgical, multidisciplinary PAC at PAH, a 750 bed tertiary teaching hospital in Queensland.
All patients who attended PAC and could provide written, informed consent were considered for participation. Patients were excluded if they were under 18 years of age, unable to communicate due to language difficulties or undergoing day surgery. A previous audit in PAH PAC showed an error rate of 12% of orders [18]. Using an expected error rate of 8% in the intervention arm a sample size of 932 orders per group was calculated to be required for a power of 80%. Assuming an average of 5 orders per patient, it was estimated that 200 patients per arm would be required for the main study.
Intervention cohort
Patients were seen by a nurse, prescribing pharmacist, Resident Medical Officer (RMO) and anaesthetist. Patients were seen by the pharmacist before they were seen by the RMO to allow usual RMO duties and a countersignature of the pharmacist prescriptions, a site requirement. The pharmacist undertook all pharmacist duties as per usual care, as well as prescribing medications on the NIMC.
Control cohort
Patients were seen by all four health care professionals in clinic, as per usual care. Patients in the control arm were still seen by a pharmacist, for usual care duties of a medication history, which was documented in the PAC assessment form and on the front of the NIMC. There was no set order in the control arm, meaning the patient could see the RMO first. The prescribing of the NIMC was the responsibility of the RMO.
Sample of patients for panel assessment of appropriateness
Intervention and control patients from the main study were stratified in to 5 groups, from the first patient recruited to the last patient, in blocks of 40. Microsoft Excel random number generator was used to pick 2 numbers from each stratified group, giving a total of 10 patients (5%) from both arms. The rationale for the stratification was to enable a selection of patients from across the study timeline, and a selection of prescribers in the control arm, as the study spanned across two rotations of junior doctors. Patients identified in the medication history in PAC as not taking any medication were excluded, and another number was generated until a patient who was taking medication prior to admission was selected. One patient was subsequently removed from the control group, due to being lost to follow up from the main study.
Panel selection
The panel consisted of a number of different health professionals, recognising either their involvement in the care of surgical patients, prescribing expertise or both; a consultant anaesthetist, a consultant hepatobiliary surgeon, a consultant clinical pharmacologist, a senior pharmacist with previous PAC experience, a senior PAC nurse, and a RMO with previous surgical and PAC experience. All panel members were independent to the research team.
Medication appropriateness index
Previous studies assessing appropriateness of prescribing, including non-medical prescribing, have identified the Medication Appropriateness Index (MAI) as the most suitable tool with which to assess appropriateness in an acute setting, with good inter and intra rater variability [19]. The tool consists of a 10-item rating system; indication, effectiveness, dose, correct directions, practical directions, drug-drug interactions, drug-disease interactions, duplication, duration and cost. Amendments were made to the MAI for our study; items regarding duration of therapy and cost effectiveness were not considered applicable, due to the scope of the pharmacist’s prescribing being medications that the patient was already taking. Additional questions were added, as the MAI does not assess under prescribing. Our finalised tool contained two questions to assess whether there had been an omission, and the significance in terms of potential ward inconvenience and patient harm. With regards to appropriateness of prescribing, the final tool contained 8 items. The original three-point Likert scale was dichotomised to either appropriate or inappropriate, as the original midpoint (marginally appropriate) was considered too subjective, as per previous studies [19].
Five patients were piloted by one member of the research team and one panel member prior to the panel assessment to assess whether the modified MAI could be applied to the patients appropriately, and to gain a rough estimate of an average time per patient. Time was an important factor, as this determined the number of patients that could be reasonably assessed, taking in to consideration panel members’ availability. A member of the research team met with all panel members prior to the panel sittings to discuss the modified MAI. Agreement was reached that it would be an appropriate tool to assess appropriateness and significance of omissions.
Assessment of prescribing and omissions
Panel members were provided with copies of patient’s PAC notes, including the medication history taken by the PAC pharmacist, and the NIMC. The panel was blinded as to whether the patients were control or intervention. There was a possibility that panel members may have been able to identify whether the patient was in the control arm or intervention arm from the handwriting of the prescriber, as they were provided with the original medication charts. However, this risk of bias was judged to be minimal due to the multiple prescribers in the control arm, and the patients being presented to the panel in a random order. Signatures were considered to be a more obvious risk to unblinding, and as such they were removed from the NIMC that was given to the panel members. Resources provided included the Australian Medicines Handbook (AMH), locally produced PAC medication guidelines containing recommendations for management of medications peri operatively, and individual consultant preferences obtained by clinic for management of certain groups of medications peri operatively, for example anticoagulants. The panel was convened for 2 sittings, and each individual panel member rated every medication prescribed on to the NIMC using the criteria set out by the amended MAI. An unintentional omission was defined as any medication from the medication history not prescribed on the medication chart, with no supporting documentation as to why. Omissions were noted and panel members rated each one as whether it had the potential for patient harm, ward inconvenience, or both. Due to clinical duties only three panel members, the surgeon, clinical pharmacologist and pharmacist were able to make both sittings, and review all 19 patients. The other three panel members were only able to make one of the 2 sittings and reviewed as many patients possible in that time.
Data analysis
A medication was scored zero, and classed appropriate, if none of the 8 items on the MAI was rated as inappropriate. A medication was given a score of 1, and classed inappropriate, if one or more of the 8 items received a rating of inappropriate. Each panel member’s ratings were evaluated individually, and ratings from all 6 panel members were combined, by adding the number of inappropriate reviews together. This gave the total number of medications that were rated as inappropriately prescribed, from the total number of reviews of medications that were undertaken by the panel. All statistical analysis was conducted using Stata 11.2 (Stata Corp, College Station, Tx). Categorical data was analysed by chi-square tests. When the value in any one cell was below ten a Fisher’s exact test was used as chi-square tests can become unreliable.
A p-value of <0.05 was considered statistically significant for the total number of omissions and individual reviewer assessment of appropriateness of prescribing.
The sample included 19 patients, resulting in 294 medication assessments for appropriateness for the control arm, and 266 for the intervention arm, from the entire panel.
The demographics of patients selected for the appropriateness panel assessment were similar to those of patients from the main study [17] (Table 1).
| Control | Intervention | Control | Intervention | |
|---|---|---|---|---|
| Main Study | Sub Set | |||
| Total Patients | 190 | 194 | 9 | 10 |
| Age ‡ | 57.6 [18-89] | 55.8 [18-86] | 73 [55-85] | 58 [34-77] |
| Male (%) | 58% | 59% | 67% | 60% |
| *Regular Medications† | 4[0-16] | 3[0-18] | 4 [2-13] | 3 [1-10] |
| #When Required ‘PRN’ Medications† | 2[0-7] | 1[0-4] | 2 [0-6] | 0 [0-4] |
| Complementary and Alternative Medicines (CAM) † | (0)[0-9] | (0)[0-6] | (0)[0-7] | (0)[0-1] |
| Over The Counter (OTC) Medications† | (0)[0-2] | (0)[0-2] | (0)[0-1] | (0)[0-1] |
| Total Medications | 1364 | 983 | 89 | 56 |
| Total medications (regular and prn only) | 1217 | 887 | - | - |
| Medication Charts Prescribed | 161 (85%) | 194 (100%) | - | - |
Table 1: Characteristics of Study Population.
Appropriateness of prescribing
Based on individual reviewer’s assessments only one reviewer, the pharmacist, showed statistical significance, 6/61 medications assessed inappropriate in the control arm, compared to 0/54 in the intervention (p=0.029).
Reviewer assessments were combined by adding the results together, in an attempt to describe the overall appropriateness. Out of 294 medication assessments across the panel for appropriateness, 32 (10.9%) of the medications prescribed in the control arm were classed inappropriate, when compared to 13 out of 266 (4.9%) in the intervention arm.
From the entire panel, an average of 5.7% of reviews across both arms were judged as inappropriate, with a range of 0 – 18.8%. Nine of the 19 patients were judged as having no inappropriate prescribing, 4 from the control arm and 5 from the intervention arm.
There was a 78% agreement between panel members on inappropriateness of prescribing.
Table 2 shows total medications reviewed by each panel member, and a breakdown of reasons why each reviewer thought an individual medication was prescribed inappropriately.
| Reviewer | Anaesthetist | Pharmacologist | Nurse | Pharmacist | RMO | Surgeon | ||||||
| Number of Patients Reviewed | 14 | 26 | 15 | 26 | 15 | 26 | ||||||
| Medications Reviewed | 77 | 110 | 73 | 115 | 68 | 117 | ||||||
| Inappropriate Medications (%) | 4 (5) | 10 (9) | 6 (8) | 6 (5) | 6 (9) | 13 (11) | ||||||
| Reason | C | I | C | I | C | I | C | I | C | I | C | I |
| Medication Indicated | 0 | 0 | 2 | 3 | 0 | 0 | 1 | 0 | 1 | 2 | 1 | 2 |
| Medication Effective | 0 | 0 | 1 | 3 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 |
| Dose Correct | 1 | 0 | 0 | 0 | 4 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Directions Correct | 2 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 2 | 0 | 2 | 2 |
| Directions Practical | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 |
| Drug–Drug Interaction | 0 | 0 | 3 | 0 | 4 | 0 | 3 | 0 | 0 | 0 | 1 | 0 |
| Drug–Disease Interaction | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | 6 |
| Duplication | 0 | 0 | 4 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 2 | 0 |
| Total | 3 | 1 | 10 | 6 | 13 | 0 | 7 | 0 | 4 | 3 | 10 | 14 |
Table 2: Number of Inappropriate Ratings and Reasons for Being Classed as Inappropriate by Reviewer (some data missing).
Omissions
There were significantly more omissions in the control arm, of which four panel members’ individual assessments showed significant numbers had the potential for either patient harm or ward inconvenience. Total unintentional medication omissions from the NIMC in the main study was significantly higher for control patients (31.5%) compared to intervention (1.2%) (p<0.001, chi-square). Omissions from the 5% sample of patients were reflective of these results. Out of 89 regular medications in the patients’ medication histories in the control arm, 25 (28%) were omitted from the NIMC, compared to 1 out of 55 (2%) in the control arm (p<0.001, exact). In the control group, all patients had at least one omission. The median number of omissions was 2, with a range between 1-7. When asked to assess the severity of omission, all the reviewers thought a percentage of the omissions had the potential for patient harm, ward inconvenience, or both. The lowest individual reviewer assessment was 40% and the highest 78%, with the average across the panel showing 52% of omissions in the control arm were assessed as having the potential for patient harm or ward inconvenience (Figure 1). Only one reviewer thought the omission in the intervention arm was significant.
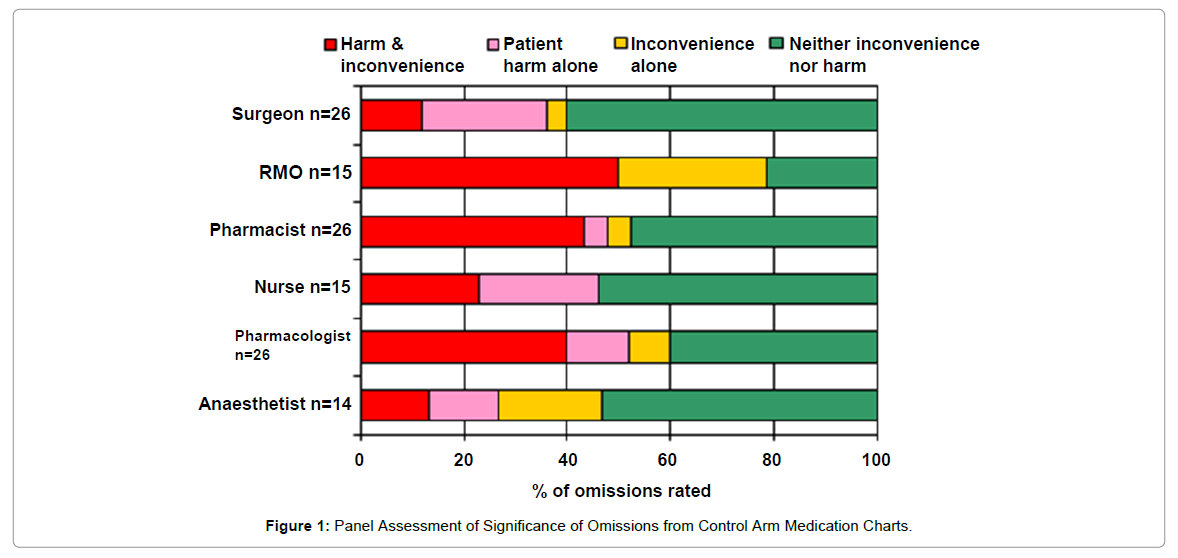
Figure 1: Panel Assessment of Significance of Omissions from Control Arm Medication Charts.
Difference of opinion regarding significance of an omission is inevitable, some of the examples of omissions that were rated as ‘potential for harm’ by all reviewers were; omission of aspirin from the medication chart in two patients, one of whom had a previous cerebrovascular accident (CVA) in 1995, and one of whom had a history of ischaemic heart disease (IHD); omission of esomeprazole 40 mg from the medication chart of a patient who suffered from chronic gastro-oesophogeal reflux disease (GORD), and omission of perindopril 2.5 mg daily in a patient diagnosed with hypertension.
Our study showed that the appropriateness of prescribing from a collaborative doctor – pharmacist approach to prescribing was similar to usual care prescribing, and produced medication charts that contained significantly fewer omissions of relevant medications.
Previous interventions to improve the appropriateness of prescribing have included an increase in clinical pharmacy involvement during the inpatient stay, which improved the prescribing of medicines [20,21]. Since the introduction of non-medical prescribing in UK, studies of appropriateness where nurses and pharmacists have taken on the prescribing role have shown that nurse and pharmacists were making clinically appropriate prescribing decisions [19,22].
There are various methods and tools in the literature to assess the appropriateness of prescribing, each with their own limitations [23,24]. The method chosen for our study was one of individual clinician, judgement based assessment. It has been suggested the results from this method may not always be valid, reproducible or generalisable. However, the same authors suggested that these limitations were remediable by using detailed specifications, validated instruments to obtain data and by training data collectors [1]. The use of the MAI satisfied all of these remedial criteria, although amongst the 6 panel members differences of opinion as to the appropriateness of prescribing, or the significance of an omission is inevitable. Another approach could have been to ask the panel to use the MAI to rate each medication as a panel, rather than individually. The authors felt the issue of perceived seniority within the panel may have introduced bias in to the final decision, hence it was felt more reliable to ask each panel member to rate autonomously.
From Table 2, it can be seen that no one item from the assessment tool stood out as being the main reason why the prescribing was assessed as inappropriate across both arms. No indication, ineffective medications and duplication of medications can contribute to inappropriate polypharmacy, and increase the chance of medication misadventure [3]. Inappropriate doses and directions for medication increase the chance of incorrect administration of medication as an inpatient [11]. Omissions of medications from the inpatient medication chart, if not rectified during the inpatient stay, are likely to be omitted on any discharge information and summary as patients cross settings. This will expose the patient to an increased chance of poor outcomes, including unplanned 30 day readmission [9].
The study is limited by the small numbers of patients assessed by the panel for appropriateness of prescribing, and the inability of the entire panel to review all the patients, due to time constraints. One of the recognised limitations of the MAI is that it is time consuming, however it was considered the best tool for the clinical setting in which the study was conducted. Panel members’ availability and the amount of time deemed reasonable for members to commit to the panel amongst other clinical commitments, limited the number of patients that it was possible to assess, which affected the statistical power of the study, and the ability to assess rater variability. Future studies should bear in mind the requirement for all panel members to see all patients, to ensure consistency in the numbers of medications reviewed by each panel member.
The summing of the individual reviewer assessments to describe overall appropriateness would be flawed in the event of a panel not agreeing on what makes prescribing inappropriate. However, the use of an objective, validated tool with good inter rater variability was used to counteract that concern. Difference of opinion is inevitable, but our panel reached 78% agreement, with regards to inappropriate prescribing.
It can be challenging to link inappropriate prescribing to important outcome measures, such as mortality, morbidity and adverse drug events. However, from what is known on the subject of polypharmacy, and omissions of medication, there is little doubt that a review of medications on admission, a complete and accurate medication chart during the inpatient stay, and accurate transfer of information on discharge are all essential components of effective medication management and quality use of medicines [3,5,7,9].
A methodology had been developed that provides guidance for future assessments of the appropriate of prescribing in any study of non-medical prescribing. Results from this small snapshot of prescribing are encouraging, and merit repeating the panel assessment on a larger scale. Larger numbers and more robust statistical analysis are necessary to enable any sound conclusions to be drawn, and for the results to be extrapolated and generalised outside of our small study.
For the appropriateness of prescribing, observed results were similar between arms, as judged by individual panel members. Medication charts in the control arm contained significantly more omissions than in the intervention arm, a number of which were rated by the panel members as having the potential for patient harm or ward inconvenience.
A larger sample size is required to make statistical significance or non-inferior conclusions between the two arms.
The authors would like to thank the following people for their involvement in the study:
Ms Ching-Ting Hung
Dr Thomas O’Rourke
Dr Elizabeth Maycock
Dr Gary Foo
Ms Elaine Brown