Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2015) Volume 3, Issue 1
Renal infarction is a common clinical problem and often misdiagnosed because the symptoms are subtle. We are presented our patient who applicant with left flank pain and diagnosed renal infarction. 49-year-old male patient has come with 2 days of severe left flank. Pathologic were; left costovertebral angle tenderness, creatinine: 1.3 mg/dL, C reactive protein: 11.4 mg/dL. On Computed Tomography Angiography renal arteries there was no contrast matter transmission to left arcuat artery distale and there were ischemic regions. With renal infarction diagnose, patient was hospitalized. Organized thrombosis seen inside apical left ventricular aneurysm with transesophageal ecocardiography Patient was discharged from hospital with plannings of policlinic controls for INR follow-ups. We want to emphasize that it should be kept in mind that the diagnosis of renal infarction in the clinical management of patients with flank pain.
Keywords: Thromboembolism; Renal Ä°nfarction; Angiography
One of the most common cause of renal artery thrombosis is thromboembolic events originated from heart or aorta. Spontaneous renal artery thrombosis is quite rare. Renal artery thrombosis are generally due to blunt abdominal trauma and atherosclerotic lesions from renal arteries [1]. Case reports related with renal infarctions were reported in the literature such as possibly connected with polisitemia vera, pregnancy, hypercoagulability, renal transplants, intraabdominal balloon insertion, renal angiography, oral contraceptives, intravenosus cocain usage, nephrotic syndrome, systemic lupus erythematosus, renovascular hypertension, infective endocarditis, Ehler-Danlos syndrome and renal surgery [2-8]. The diagnosis of renal infarction as a rarely seen clinical problem can be difficult. Renal infarction must be kept in mind as a differantial diagnosis in the cases presented with severe flank pain. The most important issue is to think this entity. Herein, we are aimed for to present our case presented with severe flank pain and diagnosed as renal infarction.
When 49-year-old male patient has been admitted to emergency room with 2 days of severe left flank pain and internal medicine clinic was consulted. There were no diabetes mellitus, hypertension, dyslipidemia, heart failure, atrial fibrillation or hypercoagulability syndrome in his history. Vital findings were normal in the physical examination except left costovertebral angle tenderness. Pathological laboratory findings were; creatinine: 1.3 mg/dL, C reactive protein: 11.4 mg/dL. There was no leucocytosis. Lactate dehydrogenase (LDH) levels and coagulation parameters were in normal ranges. In urinary tests, there were no haematuria or proteinuria. Electrocardiogram was in normal sinus rhythm. There were no renal stone or obstructive uropathy in abdominal ultrasonography. Posterior-anterior chest X-ray was normal. There were ischemic regions on upper pole of left kidney related to renal infarction in the contrasted abdominal computed tomography scan. Renal arteries were open in Computer Tomography Angiography but there was no contrast material transmission to distale part of the left arcuat artery (Figure 1).
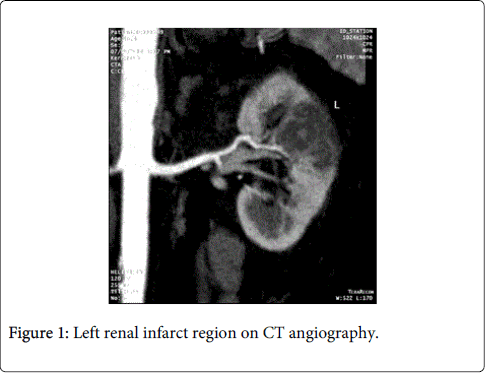
Figure 1: Left renal infarct region on CT angiography.
Patient was hospitalized with the diagnosis of renal infarction. Searching the etiology and anticoagulant treatment were planned. Ceftriaxone antibiotheraphy, low molecule density heparine (LMDH) and warfarine had started. There was regional movement defect in left ventricul of anterior and septum with transthoracic echocardiogram. Left ventricul ejection fraction was %50. Other transthoracic echocardiographic findings were normal but there were an organized thrombosis inside the apical left ventricular aneurysm in the transesophageal echocardiography.
Anti nuclear antibody, perinuclear anti neutrophil and cythoplasmic anti neutrophilic antibody, protein C and protein S levels, Factor V Leiden mutation, anticardiolipine antibody IgM and IgG, antithrombine 3 activity, B12 vitamine, folic acid, homocysteine levels were all in normal ranges. Lower and upper extremities’ arteriovenosus Doppler ultrasonography had been found normal.
We aimed to be INR range 2.0 to 3.0 for treatment. LMDH was stopped when INR reached to effective levels in terms of consequent. Reperfusion was seen after 7 days of the treatment by computed tomographic angiography (CT angiography) on renal infaction regions (Figure 2). The patient had no pain and serum creatinine level was lower to 1.2 mg/dL at that time. Regular INR follow-ups were planned per week and patient was discharged.
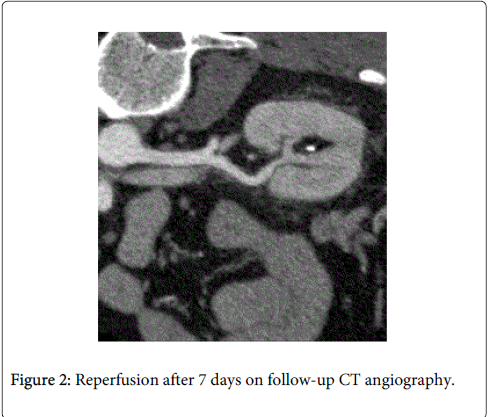
Figure 2: Reperfusion after 7 days on follow-up CT angiography.
Renal artery thrombosis is usually seen at the age of 30-50’s. Incidence is 0.01% in Europe and Asia [9,10]. Atrial fibrillation, heart valve replacement, renal artery injury, mitrale stenosis and tobacco usage are common risk factors for renal infarction [11]. Patients are usually presented by rapidly started colic pain in upper abdomen or flank region. Leucocytosis, haematuria and proteinuria can be seen with symptoms like fever, nausea and vomiting. Although, laboratory findings such as LDH elevation and leucocytosis were not found in our case. renal infarction were still exist in our list of differantial diagnosis and we had tried to image the renal artery tree by CT angiography. This diagnose would be confirmed with Magnetic Resonance Imaging along with Computed Tomography [12]. Also, contrast-enhanced ultrasound (CEUS) would be used instead of CT angiography [13].
Severe acute abdominal or flank pain algorithm is seen on Schema 1 [14]. Computed tomography together with CT angiography can be useful in the diagnosis renal infarction presented with acute abdomen.
Our case was also different from the most cases in the literature which were usually seen with elevated LDH levels [15]. In our case despite of a large infarction area, LDH levels were not elevated Therefore, normal LDH levels may not exclude renal infarction.
We had a good result with a rapid diagnosis and treatment. Reperfusion was achieved by anticoagulant therapy.
In cases with renal infarction, it is important that diagnosis must be configured rapidly and treatment must be started as soon as possible to avoid irreversible renal damage [16]. Thrombolitic treatment is recommended to start within first 6 hours of the pain. In new treatment modalities, there are spesific treatment approaches like low dose of intraarterial streptokinase injection and percutane transluminale angioplasty [17,18]. If there is a delay on diagnosis and if thrombolitic/anticoagulant therapy is not started on time, there will be surgical options leading to nephrectomy [19].
For those cases presented with severe abdominal, lumbal or flank pain, renal infarction must be kept in mind in the differantial diagnosis.