Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 2
Here we define two cases with a diffuse soft tissue uptake of I-131 in neck and mediastinum on post ablation scan. A diffuse uptake of I-131 in the soft tissue is very rare. In this case report we review the literature and discuss the mechanism of the uptake.
<Keywords: I-131 Ablation, Thyroid cancer, Soft tissue
Although rare, the incidence of thyroid carcinoma is increasing and I-131 remnant ablation is used in some patients to increase the sensitivity of thyroglobulin tests and to decrease the recurrence [1]. A false positive uptake of I-131 demonstrated on whole body imaging following ablative therapy is a challenge for the clinician. The false positive uptake in the head and neck region is mostly due to a thyroglossal cyst uptake, tracheostomy incision or thymic uptake [1]. Here we define two cases with diffuse I-131 uptake in neck and mediastinum in which the above mentioned situations are absent.
Case Report
Case 1
The first patient was a female who is 41 year old. A mass was diagnosed in the left ovary and excised through a wedge resection yielded a mature cystic teratoma of 3 cm diameter. A thyroid tissue of 1 cm diameter was localized in the teratoma and histopathologically it was a papillary thyroid carcinoma of follicular type. A thyroid ultrasonography and thyrod function tests were performed. The patient was euthyroid without any thyroid nodules. There were not any metastases on thorax CT and bone scintigraphy.
A thyroid carcinoma located in an ovarian teratoma is rare [2] with 5 % metastases rate [3]. A total thyroidectomy followed by a radioiodine remnant ablation was performed in order to use the thyroglobulin on follow-up [4]. The other purpose was to ablate thyroid tissue completely so that radioiodine can be applied for the treatment of any metastases whenever there is a need. A total thyroidectomy was performed. The thyroid was benign histopathologically. The patient experienced mild pain and mild edema on neck during her hospital stay, following a 100 mCi radioiodine treatment.
A whole body scan was performed on fifth day following radioiodine treatment. There was a focal residual thyroid tissue on both sides of the neck and a pyramidal lob activity on the left side (Figure 1a). Additionally, there was a diffuse uptake on the mediastinum. The shape of diffuse uptake was similar to two arrow-heads pointing downwards (Figure 1b). We called it a double-V sign. The uptake was proved to be located on the skin and subcutaneous tissue on lateral images (Figure 1c). This activity was nearly absent on 8th day. The patient is disease free at 27th month following radioiodine therapy.
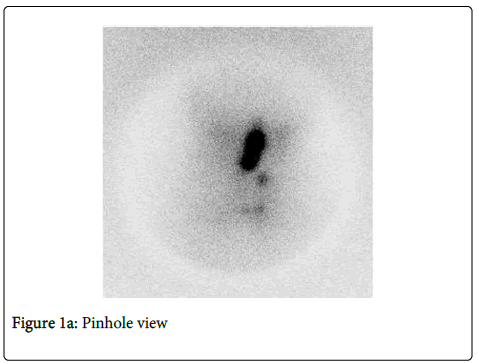
Figure 1a: Pinhole view
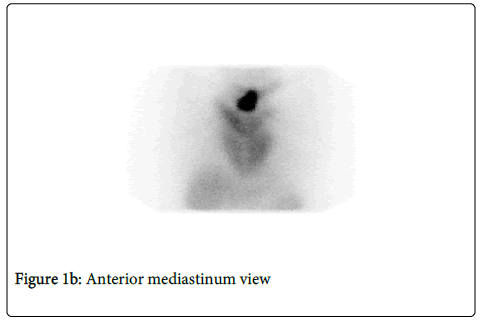
Figure 1b: Anterior mediastinum view
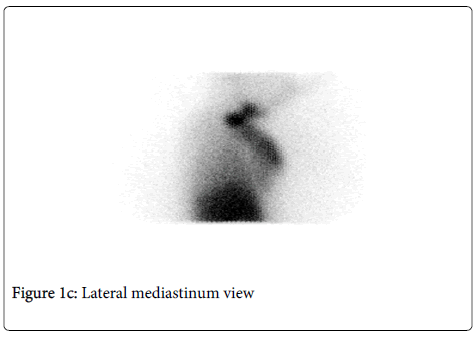
Figure 1c: Lateral mediastinum view
Case 2:
The second patient was a female who is 43 year old. A minimally invasive follicular carcinoma of hurthle cell variant was diagnosed following a total thyroidectomy. A radioiodine therapy of 100 mCi was performed. The patient did not experience any complaints during admission. On the whole body scan obtained on the 7th day following ablative therapy there was a pyramidal lobe activity in the midline and very faint focal activities on the thyroid bed on the left side (Figure 2a). Additionally, there was an activity in the neck and mediastinum (like a “Y” letter) which was prominent on the right side (Figure 2b). The uptake was proved to be located on the skin and subcutaneous tissue on the lateral images (Figure 2c). This activity was nearly absent on 12th day. The patient is disease free at 19th month following radioiodine therapy.
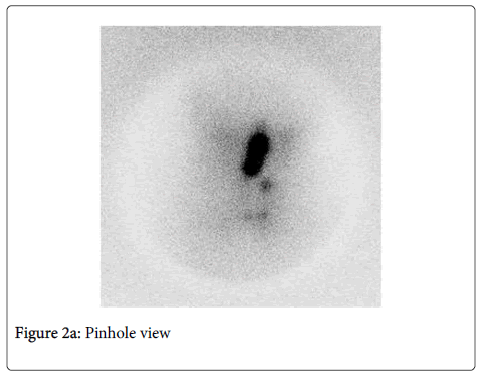
Figure 2a: Pinhole view
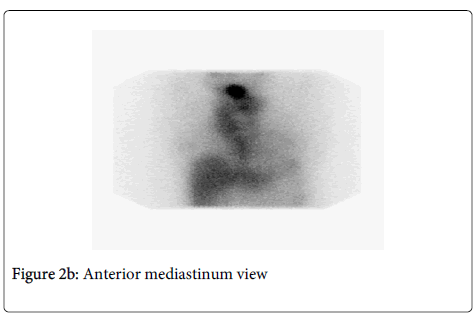
Figure 2b: Anterior mediastinum view
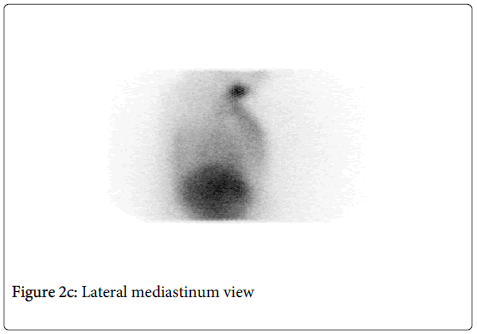
Figure 2c: Lateral mediastinum view
There were many pitfalls that were defined in the literature in the post-ablative I-131 scans. A pyelocalyceal diverticulum [5], or a cyst [6] of the kidney can be the source of the uptake. Also a leiomyoma of the uterus [7] is another cause for false negative images. Also a diffuse uptake in bronchiectasis of lung is another pitfall [8].
A false positive uptake in the neck and mediastinum can also be observed. An uptake in the thyroglossal cyst, in the tracheostomy region and in the thymic tissue is the cause in most cases [1]. Interestingly, in our patients the uptake is both in the neck and mediastinum and is confined to skin and the subcutaneous tissue. Both patients had a prominent residual pyramidal lobe. The uptake was ceased on late follow-up images. We think that the observed uptake in both patients were the due to the increased blood flow followed by hyperemia and the inflammation of the skin and subcutaneous tissue secondary to the I-131 radiation in the residual tissue. This was previously defined by Ho-Cheon in a patient thyroid carcinoma [9]. But, the uptake in that patient was diffuse in the mediastinum.
These two case reports demonstrate a rare pitfall of I-131 post-ablative scan with high mediastinal uptakes in patients with residual thyroid tissue.