Enzyme Engineering
Open Access
ISSN: 2329-6674
ISSN: 2329-6674
Review Article - (2013) Volume 2, Issue 1
Keywords: Aztreonam, Bioinformatics, Gram-negative pathogens,Metallo-β,-lactamases, Multidrug resistance, New Delhi metallo-betalactamase, NDM-1
New Delhi metallo-β-lactamase (NDM-1) is a serious threat to the existing antibiotic armory [1], and a potent weapon for bacteria to aid in in their ‘battle’ [2]. After the first report in 2009 [3], NDM-1 became a subject of discussion in scientific as well as political circles, and continues to remain so [4]. Extended-spectrum β-lactamases (ESBLs) are bacterial enzymes that confer resistance to advanced generation cephalosporins, and can lead to therapeutic failures [5]. It is agreed upon by experts across the globe that bacteria that simultaneously produce an ESBL, and at least one carbapenemase, are particularly challenging for the clinicians [6]. NDM-1 is a novel class B carbapenemase. Carbapenemases are either serine enzymes or metallo- β-lactamases (MBLs), that utilize at least one zinc ion for hydrolysis. NDM-1 possesses the ability to inactivate all beta lactams, except aztreonam. However, most of the NDM-1 producers also produce beta lactamases that can hydrolyze aztreonam (e.g. CTX-M-type ESBLs). Hence, NDM-1 producers might be expected to harbor resistance against all clinically useful beta lactams [3].
A concise update on global epidemiology (2009-2012)
NDM-1 was named after the Indian capital (New Delhi), as it was first characterized in 2009 from Klebsiella pneumoniae and Escherichia coli, isolated from a Swedish patient who had received medical care in New Delhi [3]. Objections were raised against naming the bacterial enzyme after the Indian capital in political circles. Both Indian [7] and non-Indian [8] scientists voiced their opinions regarding the name given to this bacterial enzyme. An Indian expert addressed this political turmoil as ‘a tale of ersatz patriotism’ [7]. Soon Mumbai (another Indian metro city) was declared to have presence of NDM- 1 producing bacteria by Deshpande et al. [9]. It is important to mention here that Mumbai is a seaport as well. It is the most important gateway to the Middle East countries from India. Not surprisingly, in 2010 itself, NDM-1-harboring pathogens arrived in the Middle East (Sultanate of Oman) [10]. Meanwhile, reports of infection by NDM-1 producing bacteria isolated from various pockets of India continued to be published. Kumarasamy et al. [11] reported 44 NDM-1-producing bacterial isolates from Chennai (South India), 26 isolates from Haryana (North India), and 73 isolates from various other regions of India. Moreover, the same authors also reported 37 NDM-1-positive isolates from the United Kingdom [11]. Subsequently, NDM-1-producing bacteria were reported from the United Kingdom [12], USA [13], Canada [14], China [15], Japan [16]. August 2010 marked the report of the first death due to infection by NDM-1-harboring bacteria [17]. Hence, by and large, the entire globe felt the drug resistance threat imposed by NDM-1-producing pathogens. This makes sense as it is the age of globalization and increased international travel [18]. Switzerland and the Balkan region confirmed the presence of NDM-1-positive bacteria in May and June 2011, respectively [19,20]. The first variant of NDM-1 (designated as NDM-2) was reported in June 2011 [21]. It harbored a C to G substitution at position 82, resulting in an amino acid substitution of proline to alanine at position 28 [21]. Several variants of NDM-1 have been reported, NDM-6 (GenBank: JN967644.1) being the latest addition to the list. Reports about NDM-1 producing pathogens continue to arrive as we are writing this article in 2012 [22,23].
Limited therapeutic options
Tigecycline [24] and colistin, often remain the only effective drugs against NDM-1-producing pathogens. In 2011, Docobo-Pérez et al. [25] performed a study which aimed to assess the efficacies of colistin and tigecycline in an experimental model of pneumonia caused by NDM-1-producing E. coli and K. pneumoniae. The authors suggested that colistin was inappropriate for treating pneumonia due to NDM- 1-producing K. pneumoniae, and that its efficacy was suboptimal against NDM-1-producing E. coli. Also, they maintained that a high tigecycline dose was efficacious for treating experimental pneumonia due to NDM-1-producing E. coli and K. pneumoniae [25]. In contrast, Stone et al. [26] reported successful treatment of a patient infected by tigecycline-resistant and NDM-1-positive E. coli by colistin. However, current data do not reliably support the use of either of these agents as monotherapy for systemic infections due to toxicity and resistance concerns [27]. Henc, it can be safely stated that bacteria with NDM-1 are typically resistant to nearly all antibiotics [28].
Some of the recent attempts to target NDM-1-producing bacteria
In a recent 2012 study, the authors assessed the antibacterial efficacy of chemically synthesized and custom-made sulphur nanoparticles of two different sizes, and surface modifications against a number of NDM-1-positive bacterial isolates [29]. Chemically synthesized PEGylated sulphur nanoparticles showed a bactericidal effect against all tested strains, at a concentration between 9.41 and 18.82 mg/L, using microbroth dilution. In contrast, custom-made sulphur nanoparticles failed to impart any antibacterial effect at the equivalent concentrations of chemically synthesized sulphur nanoparticles [29]. In another 2012 study, Nicholson et al. [30] claimed significant antimicrobial activity of two test compounds against NDM-1-producing pathogens. These compounds were isothiourea derivatives, namely “S-(3,4- dichlorobenzyl)isothiourea hydrochloride” and “S-(4-chlorobenzyl) isothiourea hydrochloride” [30]. Some groups are working to find possible NDM-1-inhibition activity in quercitin, a green tea flavonoid, as well. As a matter of fact, currently no clinically useful NDM-1- inhibitors exist [31].
A suggested solution to the drug resistance threat imposed by NDM-1
It is known that directly targeting NDM-1 enzyme by beta lactamaseinhibitors available till date is not possible, as it possesses a metal ion (Zinc) in its active site instead of serine. NDM-1 does not attack the monobactam, aztreonam. However, most of the NDM-1-producing bacterial pathogens are aztreonam-resistant, as well. It occurs due to coproduction of other beta lactamases, capable of hydrolyzing aztreonam (e.g. CTX-M-variants) in the same bacteria. In the light of this, renowned experts had pleaded with industry to combine NXL-104 (a potent β-lactamase-inhibitor) with aztreonam. We propose to combine “aztreonam” and “inhibitor of the most frequently encountered aztreonam hydrolyzing-beta-lactamases in a given setting”, as a possible strategy against NDM-1 producers. The crux of this proposal is that the status of “most efficient aztreonam hydrolyzing-beta-lactamasesinhibitor” and subsequently, the empirical treatment against NDM-1 producing pathogens is expected to vary from region to region. As of now, it is widely accepted that CTX-Ms are the most prevalent ESBL type across the globe [32]. However, different geographical regions have different statistics with reference to the variants of CTX-M, which are predominant. For instance, CTX-M-15 is the most prevalent CTXM- variant in India [33]. The other regions might have other CTX-Mvariants as the dominant ESBL-type. Hence combining “aztreonam” and “the most efficient CTX-M-inhibitor in a given setting”, might be the therapy of choice for NDM-1-producing pathogens for that region. Furthermore, we should take into account, as to which variants follow the most prevalent variant, and so on, for the concerned geographical setting. Hence, the inhibitor should be ‘versatile’, as well, i.e. it should have the ability to inhibit most of the CTX-M-variants prevalent in the concerned setting, if not all. Figure 1 presents this idea in a focussed flowchart fashion. We find it pertinent to mention few lines regarding the bioinformatics part presented in this figure for the benefit of the readers. With reference to molecular docking studies, higher negative interaction energy for an enzyme-antibiotic complex is an indicator of more stable and effective interaction between the two during binding. A more stable and better fitting of the β-lactam antibiotic (e.g. cefotaxime) into the active site of the CTX-M enzyme would ensure an easy hydrolysis of the drug. Hence, the higher (negative) is the interaction energy for beta-lactamase-antibiotic complex, the poorer is the efficacy of that antibiotic against the given bacterial enzyme [33]. However, the case is just opposite with inhibitors. The higher (negative) is the interaction energy for enzyme-inhibitor complex, the better is the efficacy of the inhibitor against the given enzyme [34]. This is just one of the many bioinformatics parameters which are taken into consideration while comparing the suitability and efficiency of drugs or inhibitors. Furthermore, ‘docking’ might not be enough to predict suitability of inhibitors. Hence, data should be supported by Molecular Dynamic Simulations and finally confirmed by wet lab experiments (e.g. Minimum Inhibitory Conc entration tests). The approach presented in figure 1 seems logical because bacterial enzyme variants (e.g. CTX-M-variants) are appearing at a fast pace, and it is painstaking to co-crystallize each variant with inhibitors/drugs. In conclusion, we expect that this ‘region-specific treatment strategy’ (which lies at the interface of clinical microbiology and bioinformatics) would be helpful in containing the problem of drug resistance due to NDM-1-producing bacterial pathogens.
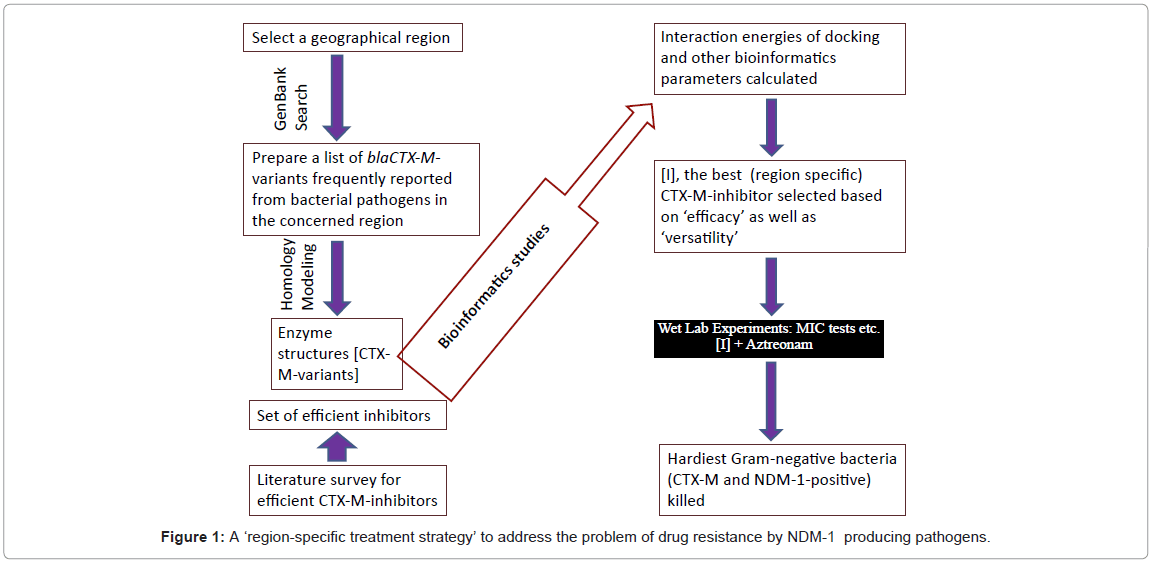
Figure 1: A ‘region-specific treatment strategy’ to address the problem of drug resistance by NDM-1 producing pathogens.
There are no conflicts of interest.
Shazi Shakil extends sincere thanks to all of the staff of Integral University, Lucknow (UP), India for co-operation.