Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Research Article - (2015) Volume 4, Issue 3
Objective: The purpose of this study is to elucidate deformation of each compression and torsion exerted to the proximal left anterior descending (LAD) artery during the cardiac cycle. Background: We hypothesised that mechanical stress exerted on the proximal LAD artery by cardiac contractions is a determinant of the need for repeat revascularization after stenting, though the proximal LAD motion has not been thoroughly studied.
Methods: We prospectively analysed the electrocardiogram-gated, 64-slice multi detector row computed tomography (CT) images obtained in 297 consecutive patients suspected of suffering from coronary artery disease for having major risk factors, an abnormal electrocardiogram, or angina pectoris.
Results: Using multi-planar reconstruction and enhanced cross-sectional CT images, the compression and torsion of the proximal LAD artery between end-systole and end-diastole were 15.6 ± 26.4% and 0.5 ± 0.6°/mm, respectively. The compression ratio was significantly smaller in diabetic (12.3 ± 33.8%) than in non-diabetic (16.5 ± 24.1%) patients (P<0.05). The torsion was also smaller in patients with versus without 3-vessel coronary disease (0.3 ± 0.3°/mm versus 0.5 ± 0.6°/mm; P<0.05) and in patients with versus without histories of previous valve surgery (0.2 ± 0.1°/mm versus 0.5 ± 0.6°/mm; P<0.05).
Conclusions: We measured the amount of compression and torsion to the proximal LAD artery associated with the cardiac contractions. These mechanical stimuli may promote plaque rupture and progression, and in-segment restenosis after stent implantations.
Keywords: Left anterior descending artery; Coronary artery motion; Coronary artery compression; Coronary artery torsion; Coronary artery computed tomography
The left anterior descending (LAD) artery supplies approximately 50% of the blood required for a normal left ventricular function. Consequently, high-grade stenoses of the LAD artery are associated with a worse prognosis than similar lesions in other coronary arteries [1], and percutaneous coronary interventions (PCI) for disease of the proximal LAD artery are followed by a higher incidence of repeat revascularization than coronary artery bypass surgery [2]. In addition, the adverse event-free survival after PCI with bare metal stents for ostial lesions is lower than for non-ostial lesions [3], and the implantation of drug eluting stent in the proximal LAD artery is more frequently a site of restenosis than the proximal left circumflex artery [1], though these observations have not been explained.
Several studies have evoked biomechanical responses as mechanisms behind the development of stent restenosis. Over dilatation of the stent is a cause of enhanced in-stent intimal hyperplasia [4]. The implantation of coronary stents modifies the 3-dimensional vessel geometry, and causes a compliance mismatch between the stented artery and its immediately proximal and distal segments [5]. Longitudinal geographical miss, defined as the mismatch between a diseased vascular target and a stent deployment site, has been associated with an increased incidence of target vessel revascularization and myocardial infarction [6]. A landmark study of the first generation of drug eluting stents found a higher rate of in-segment than of in-stent restenoses, and a higher prevalence of proximal than distal in-segment restenosis [7]. The edge of the vascular response after PCI consisted of a focal though significant proximal lumen loss that required target lesion revascularization [8]. It was hypothesized that the proximal LAD artery is mechanically stressed during the cardiac cycle, and that this stress is one of the mechanisms of in-segment restenosis after PCI, from vascular inflammation, which involves complex interactions among endothelial cells, smooth muscle cells, platelets, and inflammatory cells [9-11]. The purpose of this study was to examine the deformation associated with the proximal LAD artery motion that occurs with each cardiac cycle.
The study included 297 consecutive patients who underwent multidetector (MD) row computed tomography (CT) at the Hokkaido Cardiovascular Hospital between April and December 2012. The study, approved by the ethics committees of the Hospital and Waseda University, was performed in accordance with the ethical standards formulated in the 1964 Declaration of Helsinki and its later amendments. The anatomy and movement of the proximal LAD artery were prospectively examined and analysed, using 64-slice MDCT. Patients in whom coronary artery disease was suspected on the basis of risk factors, abnormal electrocardiogram, or manifestations consistent with angina pectoris, were included in this study. Treated or untreated hypertension, dyslipidaemia (LDL cholesterol >140 mg/dl) and diabetes mellitus, treated with diet, oral hypoglycaemic agent or insulin, were considered coronary risk factors. Patients presenting with ST segment elevation myocardial infarction (MI), unstable angina, or who had a history of coronary artery bypass graft surgery or stent implantation in the proximal LAD artery, were excluded from the study. Among the 297 consecutive patients, 38 had undergone valvular surgeries, 43 had undergone previous PCI for MI, and 40 had undergone previous PCI for angina pectoris.
Before the acquisition of the MDCT scan images, the patients were placed on a regimen of beta-adrenergic blocker and sublingual nitroglycerine. An oral or intravenous beta-adrenergic blocker was administered to lower the heart rate to <65 bpm. Cardiac electrocardiogram-gated MDCT scan images were acquired during breath-hold, using a Philips Ingenuity Core system (Philips Medical System, Eindhoven, The Netherlands). Iopamilone, (Bayer Health Care, Osaka, Japan) 0.7 ml/kg, was injected as a contrast agent at a rate of 3-5 ml/sec, immediately followed by 30 ml of saline. The effective radiation exposure was 0.78 mSv for 300 mA, and 48 contiguous 0.4-mm slice images were acquired at a 120 kV(p) tube voltage, 580-mA tube current for a 220 lb body weight, 420-ms or 500-ms gantry rotation time, and 210-ms temporal resolution. The images were reconstructed at 75% of the R-R interval to coincide with end-diastole, and at 40% of the R-R interval to coincide with end-systole. The CT images were analysed off-line by a single experienced radiological technician, using an Advantage Volume Share 4.4 Workstation (GE Healthcare, Milwaukee, WI). The display of images to measure the luminal size was set as described in a previous study [12]. A >50% vessel stenosis on a curved multiplanar image reconstruction was considered significant. A vessel was defined as diseased if a significant stenosis was present in its main trunk. An area >130 heat unit in density indicated the presence of calcification [13]. The length of the proximal LAD artery was measured in end-diastole (Ld) and end-systole (Ls) from a stretched multiplanar image reconstruction (Figure 1). The proximal LAD artery shortened (Ld>Ls) or lengthened (Ld
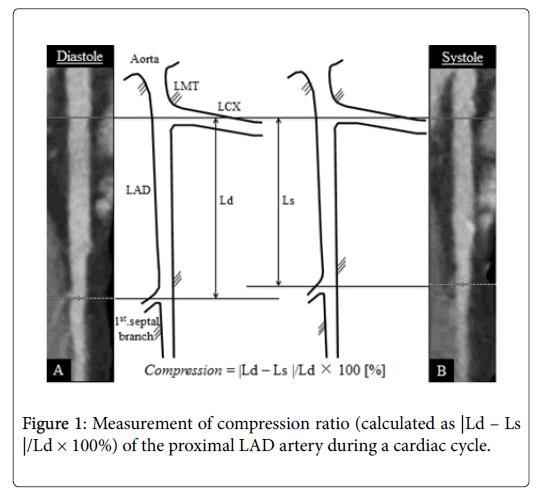
Figure 1: Measurement of compression ratio (calculated as |Ld – Ls |/Ld × 100%) of the proximal LAD artery during a cardiac cycle.
|Ld − Ls|/Ld ×100 [%] (1)
and the twist angle (Figure 2) by the formula:
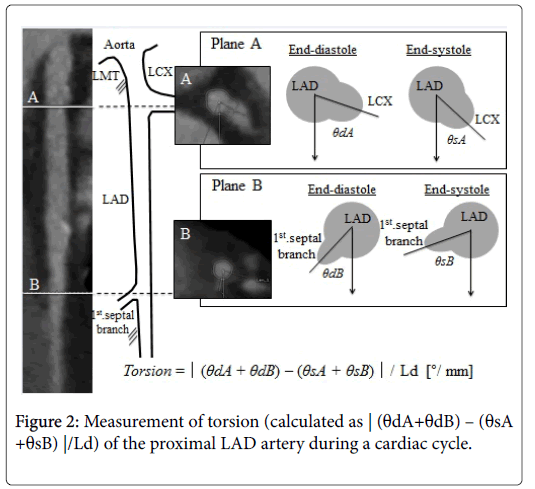
Figure 2: Measurement of torsion (calculated as | (θdA+θdB) – (θsA +θsB) |/Ld) of the proximal LAD artery during a cardiac cycle.
Δ θ=(θdA+θdB) – (θsA+θsB) (2)
where θdA and θsA are the angles between the line connecting the centres of the LAD and left circumflex arteries and the perpendicular line from abdominal to dorsal in end-diastole and end-systole, respectively. θdB and θsB are the angles between the lines connecting the centres of the LAD artery and first septal branch and the perpendicular line from abdominal to dorsal in end-diastole and end-systole, respectively. Torsion was expressed by the formula:
Δ θ/Ld [°/mm] (3)
Continuous variables are expressed as the means ± SD [95% confidence interval], and were compared, using the unpaired t-test or Mann-Whitney U-test, depending on the data distribution. A P value <0.05 was considered statistically significant. The data were analysed, using the SPSS software package, version 21.0 (SPSS, Chicago, IL).
Patient characteristics
The characteristics of the 297 patients (mean age=68.7 ± 10.7 years; 201 men) are listed in Table 1. Significant stenoses were present in 83 patients (28.8%), located in the proximal LAD artery in 6 patients (2.0%). Calcifications of the proximal LAD artery were observed in 179 patients (60.3%). The motion of the proximal LAD coronary artery was quantified as compression and torsion. The length of the proximal LAD artery in end-diastole was 27.7 ± 14.7 mm, and the difference in length between diastole and systole was 5.4 ± 11.6 mm. The twist angle was 9.6 ± 9.6°. Consequently, the compression ratio in the proximal LAD was 15.6 ± 26.4% [12.6-18.6], and the torsion was 0.5 ± 0.6°/mm [0.4-0.5].
| Age, y | 68.7 ± 10.7 |
| Male | 201 (67.7) |
| Coronary risk factors | |
| Diabetes mellitus | 64 (21.5) |
| Hypertension | 207 (69.7) |
| Dyslipidemia | 164 (55.2) |
| History of: | |
| Percutaneous coronary intervention | 83 (27.9) |
| Myocardial infarction | 43 (14.5) |
| Valvular surgery | 38 (12.8) |
| Number of diseased coronary arteries | |
| 0-vessel | 214 (71.2) |
| 1-vessel | 68 (22.9) |
| 2-vessel | 16 (5.4) |
| 3-vessel | 9 (3.0) |
| Proximal disease of the left anterior descending artery | |
| Significant stenosis | 6 (2.0) |
| Calcification | 179 (60.3) |
| Drug therapy | |
| Statin | 131 (44.1) |
| Angiotensin-converting enzyme inhibitor/receptor blocker | 84 (28.3) |
| Beta-adrenergic blocker | 83 (27.9) |
Table 1: Baseline characteristics of the 297 study patients.
The compression exerted to the proximal LAD coronary artery in men versus women and with respect to several key characteristics is shown in Table 2. The compression ratio was significantly smaller in the diabetic (12.3 ± 33.8%) than in the non-diabetic (16.5 ± 24.1%) patients (P<0.05). The compression ratio was larger in patients with (16.9 ± 41.4%) than in patients without (15.4 ± 22.9%) histories of previous MI, though the difference was of borderline significance (P=0.05). No significant differences were observed among the other subgroups. Representative end-systolic and end-diastolic CT images of the proximal LAD arteries in a diabetic and a non-diabetic patient are shown in Figure 3, along with their corresponding, calculated compression ratios. One possible reason for low compression rate may be due higher female population to male population of diabetics (men:female=49:15).
| Mean ± SD [mm] | [95% CI] | P | |
|---|---|---|---|
| Male (n=201) | 16.9 ± 29.5 | [12.8-21.0] | 0.892 |
| Female (n=96) | 12.9 ± 18.5 | [9.1-16.6] | |
| Diabetes | 0.012 | ||
| Present(n=64) | 12.3 ± 33.8 | [3.9-20.7] | |
| Absent(n=233) | 16.5 ± 24.1 | [13.4-19.6] | |
| Hypertension | 0.781 | ||
| Present(n=207) | 15.3 ± 23.5 | [12.0-18.5] | |
| Absent(n=90) | 16.3 ± 32.3 | [9.6-23.1] | |
| Dyslipidaemia | 0.994 | ||
| Present(n=164) | 15.6 ± 28.5 | [11.1-19.9] | |
| Absent(n=133) | 15.6 ± 23.8 | [11.6-19.7] | |
| Previous percutaneous coronary intervention | 0.672 | ||
| Present(n=83) | 18.0 ± 34.0 | [10.5-25.3] | |
| Absent(n=214) | 14.7 ± 22.9 | [11.6-17.7] | |
| Previous myocardial infarction | 0.050 | ||
| Present(n=43) | 16.9 ± 41.9 | [4.0-29.8] | |
| Absent(n=254) | 15.4 ± 22.9 | [12.5-18.2] | |
| Previous valve surgery | 0.490 | ||
| Present(n=38) | 15.8 ± 21.7 | [8.6-22.9] | |
| Absent(n=259) | 15.6 ± 27.1 | [12.2-18.9] | |
| Number of diseased vessels | |||
| 0-vessel (n=201) | 14.9 ± 27.2 | [1.2-18.7] | Reference |
| 1-vessel (n=71) | 18.9 ± 26.0 | [12.7-25.0] | 0.096 |
| 2-vessel (n=16) | 15.1 ± 25.0 | [1.6-28.3] | 0.519 |
| 3-vessel (n=9) | 4.7 ± 5.5 | [0.5-8.8] | 0.308 |
| >50% stenosis in proximal left anterior descending artery | 0.319 | ||
| Present(n=6) | 17.1 ± 30.8 | [-15.2-49.4] | |
| Absent(n=291) | 15.6 ± 26.4 | [12.5-18.6] | |
| Calcification in proximal left anterior descending artery | 0.137 | ||
| Present(n=179) | 16.1 ± 27.9 | [12.0-20.2] | |
| Absent(n=118) | 14.8 ± 24.2 | [10.4-19.2] | |
| Statin | 0.846 | ||
| Present(n=131) | 15.8 ± 29.7 | [10.6-20.9] | |
| Absent (n=166) | 15.4 ± 23.6 | [11.8-19.0] | |
| Angiotensin-converting inhibitor/receptor blocker | 0.995 | ||
| Present(n=84) | 13.2 ± 20.7 | [8.7-17.7] | |
| Absent (n=213) | 16.5 ± 28.4 | [12.7-20.3] | |
| Beta-adrenergic blocker | 0.599 | ||
| Present(n=83) | 14.1 ± 20.4 | [9.6-18.5] | |
| Absent(n=214) | 16.1 ± 28.5 | [12.0-19.5] | |
| Left ventricular ejection fraction | 0.999 | ||
| <50% (n=18) | 17.0 ± 27.1 | [3.5-30.5] | |
| ≥50% (n=279) | 15.5 ± 26.5 | [12.4-18.6] |
Table 2: Proximal LAD arteries compression in 297 patients.
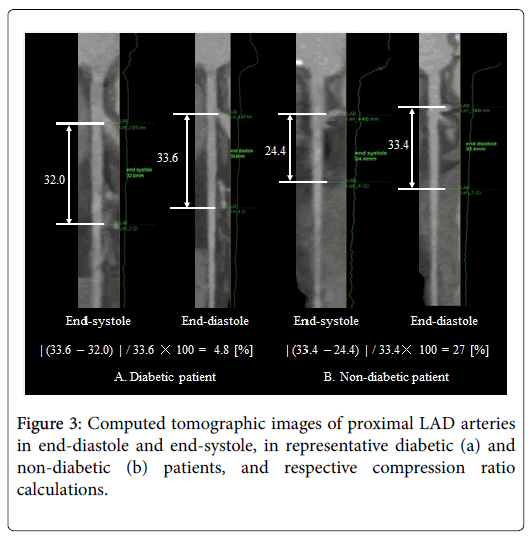
Figure 3: Computed tomographic images of proximal LAD arteries in end-diastole and end-systole, in representative diabetic (a) and non-diabetic (b) patients, and respective compression ratio calculations.
The torsion exerted to the proximal LAD coronary artery in men versus women and with respect to the same key characteristics is shown in Table 3. The torsion in patients with histories of previous valve surgery was significantly lower (0.3 ± 0.3°/mm) than in patients without (0.5 ± 0.6°/mm) histories of previous valve surgery (P<0.05). Likewise, the torsion in patients with triple vessel disease was lower (0.2 ± 0.1°/mm) than in patients without (0.5 ± 0.6°/mm) triple vessel disease, though the difference was of borderline statistical significance (P<0.05). A trend was also observed toward a lower torsion in the group of patients with (0.4 ± 0.8 mm) versus without (0.5 ± 0.6°/mm) significant stenoses of the proximal LAD (P=0.055). No significant differences were observed among the other subgroups. Representative end-systolic and end-diastolic CT images of the proximal LAD arteries of a patient with and a patient without triple vessel coronary disease, along with their corresponding, calculated measurements of torsion are shown in Figure 4.
| Mean ±SD [°/mm] | [95% CI] | P | |
|---|---|---|---|
| Male (n=201) | 0.5 ±0.6 | [0.4-0.6] | 0.128 |
| Female (n=96) | 0.4 ±0.5 | [0.3-0.5] | |
| Diabetes | 0.779 | ||
| Present(n=64) | 0.4 ±0.4 | [0.3-0.5] | |
| Absent(n=233) | 0.5 ±0.6 | [0.4-0.6] | |
| Hypertension | 0.226 | ||
| Present(n=207) | 0.4 ±0.5 | [0.4-0.5] | |
| Absent(n=90) | 0.5 ±0.7 | [0.4-0.7] | |
| Dyslipidaemia | 0.257 | ||
| Present(n=164) | 0.5 ±0.6 | [0.4-0.6] | |
| Absent(n=133) | 0.5 ±0.6 | [0.3-0.6] | |
| Previous percutaneous coronary intervention | 0.758 | ||
| Present(n=83) | 0.4 ±0.5 | [0.3-0.5] | |
| Absent(n=214) | 0.5 ±0.6 | [0.4-0.6] | |
| Previous myocardial infarction | 0.837 | ||
| Present(n=43) | 0.4 ±0.5 | [0.3-0.5] | |
| Absent(n=254) | 0.5 ±0.6 | [0.4-0.6] | |
| Previous valve surgery | 0.013 | ||
| Present(n=38) | 0.3 ±0.3 | [0.2-0.4] | |
| Absent(n=259) | 0.5 ±0.6 | [0.4-0.6] | |
| Number of diseased vessels | |||
| 0-vessel(n=201) | 0.5 ±0.6 | [0.4-0.6] | Reference |
| 1-vessel (n=71) | 0.5 ±0.6 | [0.3-0.6] | 0.972 |
| 2-vessel (n=16) | 0.3 ±0.3 | [0.2-0.5] | 0.242 |
| 3-vessel (n=9) | 0.2 ±0.1 | [0.0-0.3] | 0.009 |
| Significant stenosis in proximal left anterior descending artery | 0.055 | ||
| Present(n=6) | 0.4 ±0.8 | [-0.4-1.2] | |
| Absent(n=291) | 0.5 ±0.6 | [0.4-0.5] | |
| Calcification of proximal left anterior descending artery | 0.300 | ||
| Present(n=179) | 0.4 ±0.5 | [0.4-0.5] | |
| Absent(n=118) | 0.5 ±0.6 | [0.4-0.6] | |
| Statin | 0.710 | ||
| Present(n=131) | 0.5 ±0.6 | [0.4-0.6] | |
| Absent (n=166) | 0.5 ±0.6 | [0.4-0.6] | |
| Angiotensin-converting inhibitor/receptor blocker | 0.197 | ||
| Present(n=84) | 0.4 ±0.4 | [0.3-0.4] | |
| Absent (n=213) | 0.5 ±0.6 | [0.4-0.6] | |
| Beta-adrenergic blocker | 0.474 | ||
| Present(n=83) | 0.5 ±0.8 | [0.4-0.7] | |
| Absent(n=214) | 0.4 ±0.5 | [0.4-0.5] | |
| Left ventricular ejection fraction | 0.960 | ||
| <50% (n=18) | 0.4 ±0.5 | [0.2-0.7] | |
| ≧50% (n=279) | 0.5 ±0.6 | [0.4-0.5] |
Table 3: Proximal LAD artery torsion in 297 patients.
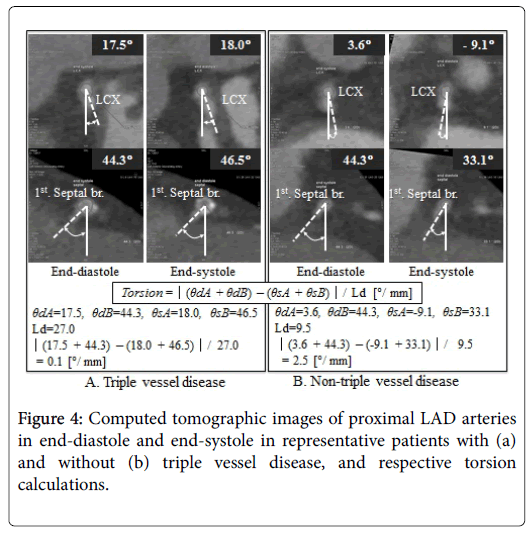
Figure 4: Computed tomographic images of proximal LAD arteries in end-diastole and end-systole in representative patients with (a) and without (b) triple vessel disease, and respective torsion calculations.
This is, to the best of our knowledge, the first quantitative study of longitudinal compression and torsion of the proximal LAD artery. We made several observations in this analysis of the proximal LAD artery motion throughout the cardiac cycle. First, the longitudinal compression of the proximal LAD artery was significantly smaller in diabetics than that in non-diabetics. The stiffness properties of the carotid arteries of patients suffering from type 2 diabetes have been found significantly greater than in control subjects [14]. These differences in arterial mechanical properties would explain the different longitudinal compression of the proximal LAD artery observed between diabetics and non-diabetics. Therefore the compression rate of the proximal LAD artery may became lower due to stiffing of coronary artery with diabetics. Second, the longitudinal compression in the proximal LAD of our patients who had histories of MI was greater than in patients without histories of MI. Hyperkinesis in the non-infarcted area has been reported to normalize overall global ventricular function [15,16]. One might hypothesize, therefore, that the presence of hyperkinesis augments the non-infarcted wall motion near the proximal LAD. Third, torsion in the proximal LAD artery during the cardiac cycle was smaller in our patients with triple vessel disease or a history of valve surgery than in patients without triple vessel disease or without previous valve surgery. Regional wall motion in the non-infarcted zone is known to be markedly depressed in presence of triple vessel disease, compared with single or two-vessel disease [16]. These observations are concordant with ours. Finally, valvular surgery decreases the motion of the atrioventricular valvular annuli, which might decrease the torsion of the proximal LAD artery. The number of valvular surgery in this study was Aortic valve replacement (n=18) and Mitral valve replacement (n=20). Both surgeries were for valves near the base of heart and it required a placement of hard structures at outer rim of these valves. This may have resulted in a limitation of cardiac twisting motion during cardiac contraction, which results in minimizing the motion near the proximal LAD artery lesion and caused the lowering of shrinking rate at the proximal LAD artery.
A previous study has described 3 types of coronary artery motion: 1) compression, 2) displacement, and 3) bend [17]. However, that study, which used 2-dimensional angiographic imaging, was limited to a qualitative analysis, and the torsion motion was not clarified. The proximal LAD artery is the most frequent site of plaque rupture resulting in acute coronary syndrome [18-21]. The cyclic longitudinal compression and torsion that we observed at the proximal LAD artery might represent mechanical causes of plaque rupture and in-segment restenosis after coronary stent implantation. And the plaque left at the proximal LAD that was not covered by coronary stent may result in plaque rupture or progression. Stent implantation as close to the ostial LAD artery may also possibly result in less effecting the compression motion. Therefore a proximal stent edge implanted closest to the ostial LAD artery would prevent proximal in-segment restenosis.
All patients included in this study were Japanese; our results should be confirmed in a non-Asian population, as the average movements of compression and torsion of the proximal LAD artery might be influenced by the heart size. Reproducibility of the measurement was pledged by having only a single technician. Beta-adrenergic blocker was used to control the cardiac rate which may result in giving negative inotropic to the heart and lower the cardiac contraction, however this study treated the measured data to be relatively equal to the data at about 65 bpm.
We measured the amount of compression and torsion to the proximal LAD artery associated with the cardiac contractions, and found the compression to be smaller in patients with than without diabetes mellitus and greater in patients with than without previous MI. Torsion was also smaller in patients with than in patients without histories of previous valve surgery or triple vessel disease. These coronary motion were considered as a risk of in-segment restenosis due to provide a mechanical stimuli to coronary artery, that may promote plaque rupture and progression, and in-segment restenosis after stent implantations.