Journal of Clinical and Experimental Ophthalmology
Open Access
ISSN: 2155-9570
ISSN: 2155-9570
Research Article - (2010) Volume 1, Issue 3
Purpose: This study intend to determine which Acrysoft monofocal IOL between single-piece (SN60WF) and multipiece (MA30AC) is better in terms of accommodation and refractive stability using an objective techniques (Autorefractor) after 1% Tropicamide eye drops to relax ciliary muscle [1]. The better ability of accommodation in monofocal standard IOL will be better to apply to minimonovision (blended monovision) formula for presbyopia correction.
Method: This is a prospective randomized control study of 42 eyes implanted with SN60WF versus 43 eyes of MA30AC by a single surgeon. Both groups were Male 45%, female 55% and the same mean age of 76 years old. The mean post-op was 30 weeks. The refraction was done by Zeiss Autorefractor before cycloplegic drop (have instrument accommodation) and after cycloplegic drop (pharmacologically relax accommodation). The diopter change in spherical equivalent is considered as accommodation. The refractive data was converted to spherical equivalent and transferred to SPSS 16 for statistic study. Pair t-test and Independent t-test was done to compare the mean spherical equivalent. The Autorefractor can be suitable for objective measurement of accommodation was concluded in Win-Hall’s study.
Result: The paired t-test showed statistically significant change (P<0.01) in spherical equivalent of refraction before and after cycloplegic drop for both of the IOLs, mean change was -0.21D. (95% Confidence interval=-0.11 to- 0.30) The independent t-test to compare two IOLs showed significant more negative accommodative change after cycloplegic drop for MA30AC mean change was -0.74D ( P<0.01), versus SN60WF mean change was -0.39D ( P<0.03).
Conclusion: Since we used cycloplegic drops to relax the ciliary muscle, we expected that the refraction diopter change from before to after the drop should be plus if there were positive accommodation. In comparison to Pilocarpine drops to induce accommodation, the change in refraction should be in minus. There were negative accommodations for both IOL 30 weeks after surgery. However, it was more on the MA30AC (5.5 mm optic, 12.5 mm in length and 5 degree angulation) versus SN60WF (6.0 mm optic, 13.0 mm in length, no angulation). This matches other studies using different method of measuring accommodation. The accommodation more likely is a psudo accommodation rather than a psudophakic accommodation according to previous studies.
Most cataract surgery patients desire to not only enjoy excellent non- spectacle corrected distant vision, but also non-corrected near vision with glasses independence in this modern era. The implantation of accommodative IOLs may achieve this vision after cataract surgery according to the literature [2]. However, the price of the accommodative IOLs is about ten times more than the standard IOL. There is also good evidence that the use of multifocal intraocular lenses can improve both near vision and distance vision after cataract surgery [3]. According a systematic review by Leyland and Pringle, it is more likely that the implantation of multifocal intraocular lenses can achieve glasses independence compared to the standard monofocal implantation after cataract surgery [3]. Nevertheless, the setbacks of these premiums multifocal IOLs such as poorer Contrast sensitivity have shown more frequently in participants who had the implantation. Furthermore, the eight studies from the Cochrane review by Leyland and Pringle, described an increased incidence of halos and glares with the premium multifocal IOLs compare to standard IOLs [3].
The attempt to find one standard IOL that can perform accommodation similar to the accommodative IOLs and can provide some degree of spectacle independence similar to multifocal IOLs become necessary to benefit those who need to be glasses independence but cannot afford the price. With a standard IOL having maximum accommodative ability and a formula of minimonovision (blended monovision) to incorporate into an IOL power calculation, may increase the possibility to accomplish glasses independence without the expensive multifocal or accommodative IOLs. The mini monovision formula also is referred to as blended monovision. It is a reduced monovision to a range of -0.75D to -1.25 D on the non-dominant eye for better tolerance. By taking advantage of the psudo accommodation, patients can maintain good distant and near vision with a standard IOLs without optical disturbance and the high cost according to a previous studies [4,5].
The standard IOLs also are called traditional IOLs in contrast to premium IOLs. Currently, it generally represents soft posterior chamber IOLs. In this study, the two standard IOLs with the same material (AcrysoftR) and the same company (Alcon, Fort Worth, Texas) with different design in pieces were compared for statistically significance in accommodation. The one –piece AcrysoftR (SN60WF) IOL already had 25 million implantations worldwide and is the most frequent implanted IOL. It is an aspheric IOL (design to avoid optical aberration) has 13 mm in length, 6.0 mm of optic size and zero haptic angulations. The other is the multi-piece AcrysoftR (MA30AC). It is 5.5 mm of optic size, 12.5 mm of length, 5 degree of haptic angulations with anterior Asymmetric Biconvex design. The accommodation (the dioptric changes from the far to the near point) consist of three mechanisms: contraction of ciliary muscle, convergence of the eye and constriction of pupil [6]. It is necessary when human eye need to see things close. The psudophakic accommodation is the accommodation of the eye when its crystal lens has been replaced by an intraocular lens (IOL). The change of refractive power in psudophakic eye during accommodation can be referred to as accommodation of psudophakic. It is associated with forward or backward movement of an intraocular lens in the eye [6] or other factors of psudo accomodation such as coma, spherical aberration and small pupil. It is hypothesised that the more accommodation the IOL can perform, the more likely it will achieve the desired far and near vision without glasses [8,9]. Various studies compare the accommodative IOL with standard IOL in accommodation [10]. The validity of subjective test is questionable while objective test using ACMaster and A- scan to test the change of anterior chamber depth under either physiological stimulus or pharmacological on ciliary muscle showed questionable change in most of the IOLs in one meta analysis [11]. Nevertheless, there is a paucity of published research regarding the comparison of psudophakic accommodation among different standard IOLs in the literature using Autorefractor as an objective test for validity. From clinical experiences showed there is a possibility that some single piece IOLs may induce more accommodation than multi-piece IOLs. This research aims to determine whether there is a statistically significant difference in mean accommodation between single piece standard IOL (SN60WF) and multi piece standard IOL (MA30AC) by comparing pre-cycloplegic and post –cycloplegic refraction thirty weeks after cataract surgery using auto-refractor as an objective method. Previous studies utilized Pilocarpine to induce accommodation [12]. Hancox found forward shift of optic of accommodative IOL (1CU Human Optics) in comparison to backward movement of MA30 IOL [10]. Forward shift of optic will favor accomodation while backward movement of optic will against accommodation [10]. Another similar study compared multipiece AcrysoftR (MA60AC) and single-piece AcrysoftR (SA60AT) using ACMasterR (Carl Zeiss, Jena, Germany) and Ultrasound Imaging SystemR (Alcon Laboratories, Fort Worth, TX, USA) as an objective method to compare the movement of the two IOLs before and after cycloplegic medication. It showed no significant differences between values of the two IOLs group7. However, in this study, it did show statistically significant difference in the two IOLs. It can be explained that the Autorefractor picked up some psudoaccommodation while ACMasterR can only picked up movement of IOLs (Psuophakic accommodation). This research also uses Cycloplegic medication to relax ciliary muscle to decrease accommodation [13] to compare the non-Cycloplegic eye in diopter change instead of the IOL movement. The non-cycloplegic eye also tends to have an accommodation known as instrument accommodation when look into an auto refractor plus many other factors such as attention and fatigue [14].The difference of refraction power between the pre-cycloplegic and post-cycloplegic will be considered as the accommodation power in diopter (D). If there is no statistical difference in refraction power between pre-cycloplegic and post-cycloplegic, it may indicate there is no statistically significant accomodation. If there is a statistical difference, the difference either favor or against the accommodation can be detected. This accommodation may be a psudoaccommodation.
The aim of this research is to prove, or disprove, the one tailed experimental hypothesis that single- piece IOLs (SN60WF) may demonstrate a statistically significant higher amount of plus accommodation in diopter compared to multipiece IOLs (MA30AC). Therefore, single-piece IOL may be more preferable to multi- piece IOL to patients who desire some degree of spectacle freedom after cataract surgery.
This is a primary experimental research
A prospective randomized Controlled trial employing a parallel group design.
Sampling strategy
The sample was drawn from the population of those patients who were scheduled for cataract surgery with standard IOL implantation in a private practice in Honolulu, Hawaii, USA.
The sample was selected using “systematic sampling”, by picking a random number between 1 and 4 as the first sample then selecting every 4th number until meeting the target.
The patients were then randomly allocated into two groups.
One group of patients received the single piece IOL (SN60WF)
And the other group received the multi- piece IOL (MA30AC).
The inclusion criteria were
1) Adults who scheduled for cataract surgery with standard IOL
2) Patients who could be followed at 30 weeks after cataract surgery.
3) Patients who consented to participate in this study.
The exclusion criteria were:
1. Cataract surgery had complications such as vitreous loss, dislocation of IOL or ciliary sulcus placed IOL.
2. Abnormal pupil such as irregular pupil (due to inflammation or surgical complication), tonic pupil and pupil smaller than 1mm to take away the pupil factor in affecting refraction.
3. Abnormal cornea such as cornea opacity, keratoconus to take away the cornea factor in affecting refraction.
4. Abnormal active vitreous retina disease such as vitreous hemorrhage, retinopathy.
5. Severe refractive errors such as high myopia, hyperopia or astigamatism.
6. Patients schedule for multifocal IOL, accommodative IOL or toric IOL implantation after cataract surgery.
Materials/ Resources
The cataract surgery and IOL implantation was performed by one surgeon at one surgical center. Subjects were scheduled to have eye examination and refraction 30 weeks after cataract surgery.
Eyes had the refraction using auto refractor first without cycloplegic drop. The cycloplegic refraction was then done after one drop of 1% Tropicamide with ten minutes of waiting. The single designated Zeiss auto- refractor (Humphrey Automatic Refractor Keratometer Model 599) was used for auto refraction and was performed by a single designated technician. The technician was masked (blinded) by giving a numbered form (have no record of subjects name, IOL type and other information) to attach the printed -out refraction data of pre-cycloplegic and post-cycloplegic. The using of a single surgeon, a single surgical center, a single technician and single equipment is to avoid inter-rater disagreement. Instead of showing IOL type on the form, the number will be assigned to either single-piece or multi-piece IOLs which will be masked to the technician as well. Using the Zeiss auto-refractor with cycloplegic medication to detect accomodation is an objective and repeatable method [13]. The subjective tests overestimated accommodative amplitude relative to the objective measures. The Autorefractor and aberrometer were accurate, reliable, and appropriate for objective accommodation measurements in pseudophakes [13]. Objective accommodation measurements such as these can be used to evaluate the performance of accommodating IOLs. The 1% Tropicamide has fast onset of cycloplegia which requires about ten to twenty minutes [13]. Therefore, the cycloplegic refraction using auto refractor was performed about ten minutes after the drop. The Zeiss auto-refractor is designed to objectively measure refraction errors of human eyes by using infrared light (880nm). The unit was made by Carl Zeiss of Germany in 1997. There are over twenty thousand of the same units in the United States. The designated unit for this study has just been serviced and calibrated for accuracy about three months ago.
Strategy for data analysis
The statistical power of this research will be calculated according to the formula to detect how many samples will be adequate. Literature has shown the Accommodative IOLs (Crystalens) had mean accommodation of 2.42 ± 0.39 D (the perceived accommodation (5.79 D) was significantly greater than the measured accommodation) versus the standard IOLs of 0.91 ± 0.24 D in one study [15]. It is considered clinically worthwhile if there is a 30% difference (clinical relevant difference) in accommodation between the two standard IOLs. The significant level (α) set at 5% and the statistical power (1-β) set at 80%.Since sample size depends on standard deviation, clinical relevant difference, significance level (Type I error, α) and power (110%-Type I error, β), the formula of n=2x (standard deviation)2 x magic number/ (difference in means)2 is used to calculate the sample size. The other method is to follow the sample size table; 40 subjects in each IOL group would be required to give 80% power, at 5% level of significance, to detect an improvement in accommodation of 25% or more. Therefore, if the null hypothesis is not true and the mean accomodation of standard IOLs of 0.91 ± 0.24 D can be improved 30% by single-piece standard IOL, it will clinically enhance patients’ reading ability especially at intermediate distance.
42 consecutive eyes implanted with SN60WF versus 43 consecutive eyes of MA30AC by a single surgeon at Surgical Suite, Honolulu, Hawaii in 2009. Both groups were Male 45%, female 55% and the same mean age of 76 years old. The mean post-op refraction was done at 30 weeks. The refraction was done by Zeiss Autorefractor before cycloplegic drop and after cycloplegic. One drop of 1% Tropicamide applied to the eye and waited for 10 minutes before refraction. The refractive data was then calculated to spherical equivalent and transferred to SPSS 16 for statistic study. A paired t-test and an Independent t-test were done to compare the mean spherical equivalent. This study has been approved for ethical issues by the IRB (Institutional review committee) of University of Hawaii.
The PAIRED t-test show statistically significantly diopter change (P<0.01) in spherical equivalent of refraction before and after cycloplegic for both of the IOLs, mean change was -0.21D. (95% Confidence interval=-0.11 to- 0.30). There was significant negative accommodation for both IOL.
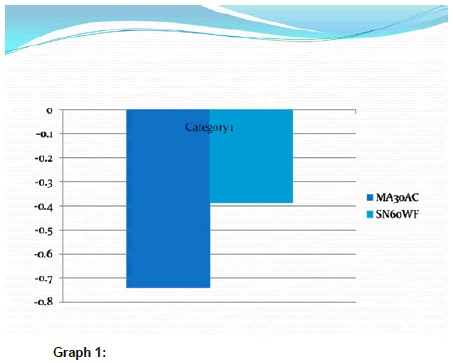
The independent t-test to compare two IOLs showed significant more change after cycloplegic for MA30AC P<0.01, mean change was -0.74 compare to SN60WF. P<0.03, mean change was -0.39. The Graph shown more mean minus diopter change with MA30AC IOL.
With the help of spherical aberration (17% indicated by Dr. Warren Hill) or other factors (small pupil, astigamatism etc), the single piece IOL (SN60WF) may have better ability for near vision with distant corrected vision after surgery compare to multi-piece IOLs (MA30-AC). The one –piece AcrysoftR (SN60WF) IOL already has 25 million implantations worldwide and is the most frequent implanted IOL, may be due to this reason. The multi-piece AcrysoftR (MA30AC) has a 5.5mm of optic size, 12.5mm of length and 5 degree of haptic angulations with anterior Asymmetric Biconvex design. It did not show more ability in accommodation compare to single-piece Acrysoft IOLs. There seems to have no true psudophakic accommodation rather is the psudoaccomodation. Single piece Acrysoft IOLs also are more refractive stable post-op than multi-piece due to its less minus shift. It should facilitate earlier spectacle prescription and quicker visual/social rehabilitation of patients after cataract surgery.
The strength of this study is the fact that the comparisons of the two IOLs were the same material, but with different design. Therefore, the result is a function of the design. In addition, the popular cycloplegic auto refraction can increase the external validity of the study.
Since the single piece IOL of SN60WF has less negative accommodation compared to multi-piece IOL (MA30AC), therefore, it proved the hypothesis that single- piece IOLs (SN60WF) demonstrate statistically significant higher amount of plus accommodation in diopter compared to multipiece IOLs (MA30AC). With a singlepiece IOLs (SN60WF) and a formula of mini monovision (blended monovision), it is likely to increase the chance of glasses independence for some motivated patients.
We would like to thank Mr. Richard Hunter to edit the text.