Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 4
Adenosquamous carcinoma is a rare form of colorectal cancer. It is believed to be more aggressive and carries a poorer prognosis compared to the more typical colonic adenocarcinomas. Here we describe a case of primary cecaladenosquamous carcinoma invading into the terminal ileum along with a review of the literature.
<Adenosquamous Carcinoma (ASC) is a tumor that is rarely of colorectal origin. Herxheimer first described it in 1907 [1]. Multiple interesting clinical features have been reported in terms of its site of origin, association with paraneoplastic syndromes and overall aggressive nature. ASC originating in the cecum has been described in only a handful of case reports. Here, we report a case of primary ASC of the cecum invading into the terminal ileum and review the literature on the topic.
A 52-year-old female with a history of intermittent right upper and lower quadrant abdominal pain presented to the emergency department with a one-day history of nausea and vomiting. She denied passage of blood or mucus in her stool, changes in bowel pattern or weight loss. Her past medical history was notable for gastric bypass surgery, total abdominal hysterectomy with bilateral oophorectomy for dysfunctional uterine bleeding, cholecystectomy, appendectomy, and ventral as well as inguinal hernia repair. Her family history was positive for Crohn’s disease, but there was no family history of colorectal cancer or other gastrointestinal malignancies. A Computed Tomography (CT) scan of the abdomen and pelvis with intravenous contrast revealed a large polypoid mass in the cecum with peripheral enhancement and heterogeneous enhancement in the center (Figure 1); multiple enlarged lymph nodes around the mass were also noted. Subsequent colonoscopy showed a friable, lobulated mass arising from the cecum (Figure 2).
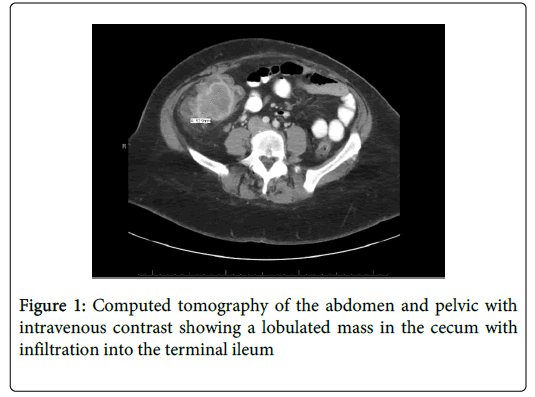
Figure 1: Computed tomography of the abdomen and pelvic with intravenous contrast showing a lobulated mass in the cecum with infiltration into the terminal ileum
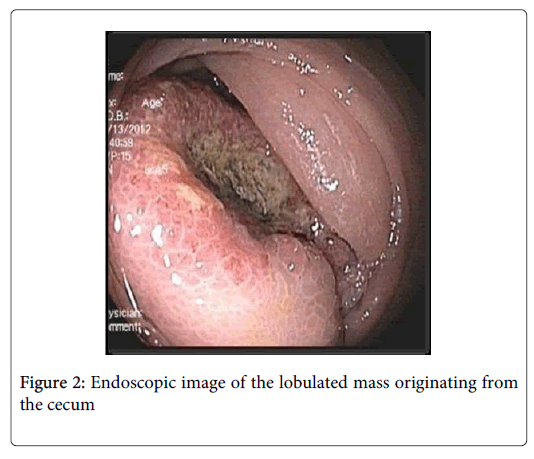
Figure 2: Endoscopic image of the lobulated mass originating from the cecum
Her serum carcinoembryonic antigen level was normal. Histopathological evaluation revealed poorly differentiated invasive carcinoma with squamous differentiation (Figure 3). Malignant cells were strongly positive for p63 at the areas of squamous differentiation and other scattered malignant cells were positive for CK20 and CDX2. MSI staining was performed and malignant cells retained nuclear staining for MLH1, MSH2, MSH6 and PSM2. A 12 cm cecal mass was seen infiltrating into the terminal ileum at the time of surgical exploration, which was followed by an open right hemicolectomy with a stapled primary ileo-colic anastomosis. The tumor was staged as IIIC with lymph-vascular invasion and seven of 64 harvested lymph nodes testing positive for tumor involvement. No other neoplastic lesions were seen at the time of staging. Adjuvant chemotherapy was planned; however, due to infection of the abdominal wall incision site it was postponed. Three months after her initial surgery, she was taken to the operating room for drainage of an abscess and was subsequently found to have cancer recurrence involving the ileocolic anastomosis site and the distal small bowel. En bloc, resection of the abdominal wall, part of the small bowel, and the anastomosis was performed followed by creation of an end ileostomy. A follow up CT scan revealed new liver lesions as well as lesions involving the abdominal wall and diaphragm that were consistent with metastases. Her tumor was re-staged as stage IV. The patient was deemed not to be candidate for chemotherapy due to her poor functional status and active infection. She was subsequently discharged to home with palliative care and passed away 5 months after the diagnosis.
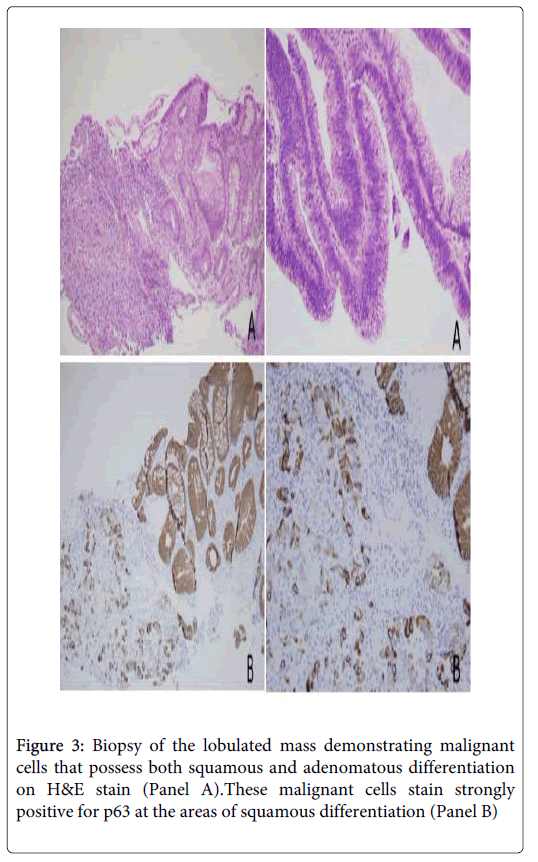
Figure 3: Biopsy of the lobulated mass demonstrating malignant cells that possess both squamous and adenomatous differentiation on H&E stain (Panel A).These malignant cells stain strongly positive for p63 at the areas of squamous differentiation (Panel B)/p>
Adenosquamous Carcinoma (ASC) is a rare form of colorectal cancer. Based on recent studies, ASC constitutes 0.06 to 0.09% of all colorectal cancers [2,3]. The most common cause of squamous histopathology in a colonic mass is a metastatic lesion, which has to be ruled out before it is deemed to be of colonic origin. In our patient, initial CT scans of the chest, abdomen and pelvis did not reveal any additional masses. There is a case report of colorectal ASC arising from endometriosis [4]. In the current case, there was no histological evidence of endometriosis in the tumor. The diagnosis of primary colorectal ASC is confirmed by the presence of both adenomatous and squamous cell carcinoma on histopathology, although the presence of a “keratin pearl” is not mandatory. Other criteria for the diagnosis of primary ASC of the colon include a colonic tumor, which arises at least 8 centimeters above the dentate line, and the absence of a colocutaneous fistula lined with squamous epithelium that communicates with the tumor [5].
Multiple hypotheses have been postulated regarding the pathogenesis of colorectal ASC, which include squamous metaplasia from chronic inflammation, squamous differentiation from pluripotent stem cells and malignant transformation to squamous cells originating from indeterminate basal cells; none of these theories has been investigated in detail [6,7]. However, the noted association of colorectal ASC with both ulcerative colitis and schistosomiasis suggests that chronic inflammation is a contributing factor [8]. The hypothesis that human papilloma virus can result in the pathogenesis of colorectal ASC has been suggested, but no association was found [6,9].
Most cases of colorectal ASC present in the sixth or seventh decade of life with a mean age of 59 years at the time of diagnosis. These findings were reported in a case series involving 44 patients in whom the youngest patient was 19 years old at the time of diagnosis [7]. Other studies reported a mean age of 65 to 67 years at the time of diagnosis [2-3]. In a study by Masoomi et al, a higher proportion of colorectal ASC cases, when compared to cases of colon adenocarcinoma, presented before the age of 60 (37% versus 22%) [2,10]. Based on these reports, it appears that ASC of the colon occurs at a younger age compared to colon adenocarcinoma.ASC of the colon affects males and females equally [2-3,7] and 70% to 84% of cases involve Caucasians [2-3]. Early studies suggested that the sigmoid colon and rectum are the most common sites of primary colorectal ASC [3]. However, a number of more recent studies have shown the distribution of colorectal ASC to be similar to that of colorectal adenocarcinoma with the right side of the colon being more commonly affected [2,7].
Due to the rarity of the disease, no specific pattern of patient presentation or predictors of clinical outcomes have been identified to date. A few cases of ASC of the colon have been found in the setting of hypercalcemia, which is thought to be a paraneoplastic phenomenon [2,11,12]. It has been proposed that the squamous cell component of colorectal ASC results in an increased potential for metastasis, thus leading to a worse prognosis [6]. While the 5-year survival rates for the earlier stages of ASC of the colon (stages I and II) have been reported to be similar to that of equally staged adenocarcinoma of the colon, the overall 5-year survival rate in colorectal ASC is much lower than that of colorectal adenocarcinoma (24%-31% versus 65%) accounting for the fact that patients with colorectal ASC usually present at a more advanced stage [2-3,13]. Additionally the presence of underlying ulcerative colitis and right sided lesions are believed to carry worse prognosis [6].
Similar to colorectal adenocarcinoma, early detection and surgical resection is usually the best therapeutic option for ASC of the colon [3,7]. Chemotherapy has been used for metastatic disease with some encouraging results [14]. However, more studies are needed to determine the exact role of chemotherapy and whether colorectal ASC has a better response to it compared to colorectal adenocarcinoma [3,7,15-17]. While radiotherapy has an established role in the management of squamous cell carcinoma of the rectum, its part in the management of more proximal colonic cancer with squamous differentiation has not been investigated [3,7,15-17]. Our patient had complicated post-surgical course precluding her from receiving timely chemotherapy or radiotherapy.
In conclusion, we believe that our case signifies the aggressive behavior of this infrequent type of colonic neoplasia, especially when it is located in the right side of the colon and diagnosed at stages higher than II. Knowledge of this entity and accurate histopathologic diagnosis is important to determine overall prognosis and direct the therapy. Surgical resection is the primary therapy, but more studies are needed to determine the role that chemotherapy and radiation therapy may play.