Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Review Article - (2013) Volume 1, Issue 2
Objective: The purpose of this research was to develop an interdisciplinary understanding of the determinants of falls leading to hip fractures among osteoporotic patients according to the disciplines of neurology and environmental epidemiology.
Background: The complexity of risk factors associated with falls and hip fractures among Canadians with osteoporosis poses a distinct challenge in injury prevention. In addition, frequent hospitalizations for hip fractures have contributed to the economic burden faced by the Canadian health care system. An interdisciplinary approach provides the possibility of developing a more profound understanding of the determinants of falls causing osteoporotic hip fractures.
Methods: The disciplines of neurology and environmental epidemiology were selected and critiqued following methods and techniques to establish an interdisciplinary understanding. A literature search was conducted to compare determinants of osteoporotic hip fractures caused by falls in regards to the neurological and environmental epidemiology disciplines. Five databases: Medline, Psycho INFO, CINAHL, Embase, and Scopus were used in the literature search from 1974 through to December 2012.
Discussion: The discipline of neurology provides insight on the role of neurological diseases and the association with falls. Environmental epidemiology provides insight on environmental exposures related to falls. Common ground was established using integrative techniques and the creation of a new interdisciplinary model.
Conclusion: An integrated understanding of what causes falls can be achieved by redefining concepts through the combination of disciplinary insights from neurology and environmental epidemiology. Further investigation into other disciplines can contribute to an interdisciplinary understanding of the determinants of hip fractures.
<Keywords: Neurology; Epidemiology; Environment and public health; Risk factors; Accidental falls; Hip fractures; Osteoporosis
Osteoporosis is major health concern in Canada as one quarter of females and one in eight men are affected by this condition [1]. Each year, osteoporosis is responsible for 70 to 90 percent of 30,000 hip fractures among Canadians [2]. Between 1985 and 2005, there were approximately 570, 872 hospitalizations for hip fractures in Canada [3]. In addition, osteoporotic hip fractures have shown to be an enormous economic burden on the Canadian health care system with approximately $44,156 in direct costs for each patient who was institutionalized after a hip fracture [4]. The purpose of this research was to develop an interdisciplinary understanding of the determinants of falls leading to hip fractures among osteoporotic patients according to the disciplines of neurology and environmental epidemiology.
There is a vast amount of literature examining nutrition [5-7] and physical activity [8-10] as determinants of hip fractures, yet it is not transparent as to why there is a high prevalence of injuries. An interdisciplinary approach to understanding other determinants of hip fractures among Canadians can support future fall and hip fracture prevention programs for osteoporotic patients.
Falls have a multi-factorial etiology [11] and researchers from diverse disciplines have various beliefs on why people suffer from falls and injuries. Falls are defined as “unintentional events in which an individual comes to rest on the ground or a lower level” [12]. After consulting scientific literature and an expert in rehabilitation sciences, the disciplines of neurology and environmental epidemiology were identified as being relevant for investigating determinants of falls. Neurology researchers typically focus on how the nervous system and neurological disorders affect injury prevalence [13]. Environmental epidemiologists are more interested in environmental determinants of injuries such as home hazards (loose carpets, narrow stairs, poor lighting) and community/institutional hazards (uneven sidewalks, obstacles in walkways, poorly designed/maintained buildings) [14].
This paper illustrates the role of neurology and environmental epidemiology in determining the causes of falls resulting in hip fractures. Both disciplines provide valuable insight in determining elements to improve fall and hip fracture prevention. A description of the methods used to search for theories which support each discipline are presented. In addition, the conflicts and commonalities between these two disciplines are described in order to develop an enhanced interdisciplinary understanding.
In order to establish an interdisciplinary understanding, steps outlined by Repko [15] were utilized. The steps include drawing on disciplinary insights by: 1) defining the problem, 2) justifying using an interdisciplinary approach, 3)identifying relevant disciplines, 4) conducting a literature search, 5) developing adequacy in each relevant discipline, and 6) analysing the problem and evaluating each insight into it. These steps are followed by integrating the insights to produce an interdisciplinary understanding by identifying conflicts between insights and their sources, creating or discovering common ground, integrating insights and producing an interdisciplinary understanding of the problem. After identifying the problem of osteoporotic hip fractures caused by falls and justifying the use of an interdisciplinary approach, a literature search was conducted to compare neurological and environmental epidemiological insights of determinants of falls resulting in osteoporotic hip fractures. Five databases: Medline, PsychoINFO, CINAHL, Embase, and Scopus were searched from 1974 through to December 2012 using the following terms: neurology, epidemiology, environment and public health, risk factors, accidental falls, hip fractures, and osteoporosis. Articles were screened by one reviewer and were included if they provided insight on determinants of accidental falls resulting in osteoporotic hip fractures from the perspective of the disciplines of neurology and environmental epidemiology. Articles were excluded if they were not written in English and if they fell outside of the scope of the two selected disciplines.
Disciplinary perspectives
Neurology: Neurology is the study of diagnosis and treatment of central, peripheral, and autonomic nervous systems [16]. In regards to determinants of falls, neurologists are interested in how neurological diseases may compromise gait patterns, increasing the risk of falls [17]. A loss of balance and marked sway are features of abnormal neurological gaits [18]. Stroke, dementia, Parkinson disease, and neuropathy have been associated with increased falls [12,19,20].
Neurologists have identified that the commonality between the groups of neurological diseases associated with falls is the common disturbance of the sensory motor system [19]. Three sensory areas which determine balance are the visual system, the vestibular system, and the proprioceptive system [21]. The primary focus is to develop interventions that promote secured mobility through the improvement mood, attention, executive functions and dual task performances [22].
The theory of sensory integration was first developed by Jean Ayres and describes the function of the brain with the aim of improving functional ability [23]. Ayres defined sensory integration as:
..the neurological process that organizes sensation from one’s own body and from the environment and makes it possible to sue the body effectively within the environment. The spatial and temporal aspects of inputs from different sensory modalities are interpreted, associated and unified. Sensory integration is information processing [24] (p.11)
The focus of the sensory integration model is the organization of sensory information in the central nervous system and how it directs adaptive motor behaviours [25]. The model, originally designed to explain the development of brain organization among children, has also been adapted to demonstrate how adults with acquired deficits revert to avoiding sensory stimulation, which they are unable to process [25]. May-Benson agrees that that the sensory integration model is appropriate for adults and stated [26]:
“Adults with sensory processing problems present with the same patterns of sensory integrative dysfunction as children. They tend to seek professional intervention when they are so overwhelmed by some aspect of defensiveness, or they are experiencing significant problems in mental health or occupational performance” [26]
The sensory integration model can illustrate how neurological disorders affect balance and gait, increasing the risk of falls. The model proposes that sensory information processing occurs in a developmental sequence of four levels. The primary level consists of the vestibular and proprioceptive senses such as eye movements, posture, balance, muscle tone and gravitational security. The second level demonstrates how the two senses are integrated into body precept, bilateral coordination, attention span, activity level, and emotional stability. The third level includes auditory and visual senses that produce speech and language, eye-hand coordination, visual perception, and purposeful activity. The fourth and final level represents the end points which allow for the ability to concentrate, ability to organize, self-esteem, self-control, self- confidence, and specialization of each side of body and brain. The model demonstrates how difficulties performing integrative tasks within each level affect motor behaviour, causing unstable gait and balance.
Dementia and Alzheimer’s disease deteriorates the interaction between neocortical areas, creating difficulties with distinct visual features such as motion and color of objects [27]. A cognitive impairment, such as dementia or delirium, often causes individuals to lose insight, creating difficulties in distinguishing between an unsafe and safe surrounding [28]. Patients with dementia in nursing homes suffer twice the amount of falls when compared to those with normal cognition [29]. A study revealed that poor scores on the Mini-Mental State Examination [11], a short mental status questionnaire, were associated with an increased risk of falls [30]. Furthermore, confused patients have an increased risk of falling [31], and depression can create physical barriers causing slower gait, balance impairment and reduced dual task performance, increasing the risk of falls [20,21]. The Longitudinal Aging Study revealed a lack of immediate memory as a risk factor for falls among individuals over the age of 75 years [32]. Patients with memory difficulties are not fully aware of past experiences, thus affecting his or her perception of falls or motivation to prevent a fall from occurring. Difficulties in visual perception are highlighted under the third level of the sensory integration model. Dementia patients have also shown to be easily distracted and inattentive to a task [33], an endpoint of the model.
Neurological disorders such as Parkinson’s disease or stroke, which affect quick generation muscle activation, create feeble responses to self-generated postural movements and external perturbations such as falls [34]. Stroke and frontal lobe disorders affect sensory feedback causing inappropriate balance responses, resulting in a greater number of falls [34]. Stroke patients tend to lean to the hemiplegic side and have a distorted sense of upright vertical [34]. The integrative tasks of balance and posture are depicted in the first level of the sensory integration model while coordination and motor planning tasks are portrayed in the second level of the model.
Cognitive disorders, including depression and fear of falling, cause executive deficits, abnormal sensory weighting, and delayed latencies which constrain the balance system [34] and cause unsecured gait [35]. Depressive symptoms may cause impaired judgement and distractions [36,37], change gait speed patterns [38,39], reduce stride length and double limb support [40], all which are important components of psychomotor retardation [41]. A fear of falling may distort a patient’s perception of falls and hip fractures, limiting an individual’s willingness to participate in activities, resulting in a decline in function [30,42]. Seventy percent of individuals who had previously fallen admitted a fear of falling, while 40 percent of those not reporting a recent fall acknowledged this same fear [30,43,44]. The lack of physical activity caused by fear can eventually lead to muscle weakness and slower walking gait [45], reducing postural performance [46]. In regards to the sensory integration model, cognitive disorders affect integrative tasks of the second level such as “attention span” and “emotional stability”, resulting in difficulties with concentration. Individuals with executive deficits require a greater amount of cognitive attention to control balance and gait [34].
Environmental epidemiology: Environmental epidemiology addresses environmental exposures that cause adverse events such as illnesses, injuries, disabilities and death [47]. The focus of environmental epidemiology is to determine the effect of external factors resulting in involuntary physical environmental exposures [48]. The physical environment consists of the natural environment as well as the built environment (roads, buildings and furniture) [49]. Environmental factors are responsible for up to half of the incidences of hip fractures [50-53]. The environmental epidemiology approach is community based and relevant interventions include street and pavement repair, home safety fall risk awareness programs. Population-based strategies are targeted to reach larger amounts of individuals and depending on the size of the injury prevention program, can vary in cost [54].
Parker et al. [55] developed a composite model which incorporates The Stress Process Model [56-61] with an ecological framework, referred to as “The Ecological Stress Process Model” (ESPM). The model focuses on physical and social environmental stressors and their effect on short and long-term outcomes. Environmental epidemiologists consider osteoporotic hip fractures, caused by falls, an environmental health-related problem [30]. According to the ESPM model, there are five categories of stressors: ambient environment, major life events, daily hassles, chronic strains, and cataclysmic events [58].
The two categories most relevant to the field of environmental epidemiology and most important when considering environmental determinants of osteoporotic hip fracture caused by falls are “ambient environmental stressors” and “daily hassles”. Parker et al. define ambient environmental stressors as “continuous conditions that exist in the physical environment that can affect an individual” [55]. Ambient environmental stressors causing falls include indoor hazards, such as those within the home, and outdoor hazards which include weather conditions. Creating a safer home environment by limiting hazards which include loose carpets, trailing wires and poor indoor and outdoor lighting can reduce the number of fractures caused by falls [62,63]. Furniture can create a tripping hazard when changing posture [64] resulting in fractures [65,66]. Floor rugs are another home hazard, responsible for up to 20 percent of falls in several studies [64-66]. Hip fractures are more common (57%) among indoor falls compared to outdoor falls [67].
Parker et al. define daily hassles as “ongoing minor events that may be perceived as bothersome” [55]. Inclement weather can disrupt daily activities and is a potential determinant of hip fractures caused by falls. Cold weather and icy condition [51,68] and inappropriate walking aids or assistive devices [69] are associated with increased incidences of hip fractures. Daily hassles may be exacerbated without walking aids and assistive devices such as ramps, grab rails, shopping carriages and scooters in commercial centres. Another factor which may contribute to daily hassles is the design of neighbourhoods. Hip fracture incidence rates are higher in residential settings [70] and neighbourhoods with an absence of public transportation services, narrow, discontinuous or steep paths, and damaged public fixtures create more inconveniences and hazards for residents [71].
The ESPM illustrates how different conditioning factors may influence the relationship between the stressor categories and short and long-term outcomes. Environmental epidemiologists are concerned with physical/structural conditioning factors, which emphasizes safe housing and neighbourhoods, reducing exposure to environmental stressors of falls.
Critique of disciplines: The sensory integration model demonstrates the organization of sensory information from the central nervous system and how it guides adaptive motor behaviours. It highlights the influence of neurological and cognitive deficits on adverse events and allows for hypothesis testing. Neurologists draw attention to how the nervous system and neurological disorders can distort senses causing health risks, such as falls.
The primary limitation of the neurological approach and the sensory integration model is its failure to incorporate interpersonal factors. The influence of those who surround us and their experiences play a vital role in health behaviour. Although sensory models provide insight of neurological and cognitive causal factors leading to adverse events, there is a lack of transparency regarding causal ordering. Furthermore, assessing determinants of falls solely from the neurological discipline fails to capture the synergistic effect of interpersonal and extrinsic factors. The sensory integration theory was not originally intended to be used among adults therefore there are a variety of proposed models that differ slightly from the original model by Ayers. There also appears to be confusion in sensory intervention terminology as researchers use both “sensory processing disorder” and “sensory modulation” [72]. A sensory approach can be identify coping strategies for individuals with sensory disorders which increase the risk of falls.
The ESPM is a simple model which demonstrates the influence of environmental hazards on the risk of falls. The discipline of environmental epidemiology theorizes that environmental hazards are necessary for the causation of falls. There is a vast amount of literature highlighting the importance of environmental hazards on falls [50-53]. Although this discipline can easily identify determinants of falls, the reality is that not all hazards are modifiable. Environmental epidemiologists identify environmental hazards, yet it is unclear as to why these hazards exist and how they are created. Creating a single environmental intervention to reduce modifiable hazards may be challenging [73]. An interdisciplinary approach may facilitate and strengthen these types of interventions.
Description and analysis of conflict: The two diverse disciplines provide different insights on the types of risk factors of falls. Causes and risk factors of injuries, including falls, are typically grouped into two categories: intrinsic and extrinsic risk factors. The neurological approach focuses on intrinsic risk factors that are related to an individual’s physical and psychological condition. Intrinsic factors are characteristics within the individual such as age, gender, ethnicity, medical condition, psychological status, and musculoskeletal factors [74]. The environmental epidemiology approach is more focused on extrinsic risk factors which include environmental influences and are external to the individual [74].
Creation of common ground: In order to develop a comprehensive interdisciplinary understanding of the determinants of falls, Repko [15] has suggested the use of several integrative techniques. The technique of organization proposes identifying an underlying commonality in meaning of different disciplinary concepts. Both disciplines address physical barriers. Patients with neurological deficits or living in a hazardous physical environment will have greater difficulties with daily living activities and participating in society. The two disciplines also highlight psychological barriers. Neurological disorders are associated with a lack of awareness, low self-confidence, low self-esteem, communication difficulties, and underdeveloped social, interpersonal and self-management skills [75]. Patients residing in unsafe physical environments have concerns about personal security, and may have a fear of incurring an injury which limits their participation in daily living activities [76].
Both disciplines highlight important aspects of determinants of falls. To create a common ground among the two disciplines, the theoretical models from each discipline require modification. The sensory integration model fails to incorporate interpersonal and extrinsic factors while the ecological stress process model does not provide enough depth regarding neurological intrinsic factors. Repko [15] proposes using an integrative technique of theory expansion. A new model which integrates both disciplinary insights and demonstrates the relationship of intrinsic and extrinsic determinants of falls is therefore needed. Repko suggests redefining key concepts from each discipline in order to create a common ground. The discipline of neurology summarizes determinants and risk factors of falls as any deviation to the sensory system which may alter balance or gait control. Environmental epidemiologists define determinants and risk factors of falls as any environmental stressor or exposure that contributes to the incidence of falls. From a multidisciplinary approach, a definition of risk factors of falls should take into account both intrinsic and extrinsic causes.
Integration and production of an interdisciplinary understanding: Investigating determinants of falls requires a multidisciplinary approach as causes are a combination of both internal and external factors. Evidence demonstrates that multi-factor approaches are more effective in reducing falls compared to single strategies [77]. The literature pertaining to interdisciplinary approaches when investigating falls is limited. A study which investigated the effect of residential light demonstrated an increased risk of falling by 1.4 times (95%CI 1.2,1.7) and were 1.5 times (95%CI 1.2,1.9) more likely to report a fall among individuals who reported inadequate natural light in their dwellings when compared to those who reported an adequate amount of natural light [78].
Repko provides various methods of expressing an interdisciplinary understanding. One method is to create a model which demonstrates how the common ground between the two disciplines can be combined to create an interdisciplinary understanding. A new model entitled “The Barriers to Falls Model” (BTF) (Figure 1) exhibits two spheres (intrinsic and extrinsic risk factors of falls) and demonstrates how a synergistic effect of both types of risk factors create physical and psychological barriers, increasing the probability of a fall. The model demonstrates how risk factors influence human behaviour and activity. Multi-level (community, physical environment, municipal/provincial/ national policy) risk factors are illustrated in the “extrinsic sphere” while individual level risk factors previously depicted in the social ecological model [79,80] can be found in the “intrinsic sphere”.
Similar to the Social Ecological Model, the BTF model considers the complex interaction between individuals, communities, environmental factors, and various levels of policy. In regards to the disciplines discussed in this paper, the concepts of neurology are characterized in the intrinsic sphere. This sphere exhibits the effects of neurological and cognitive deficits on behaviour and activity resulting in falls. Concepts of environmental epidemiology are portrayed in the extrinsic sphere as risk factors. The BTF model uses an integrated approach in identifying determinants of falls at different levels and can be useful to establish how multiple intervention programs can address these concerns.
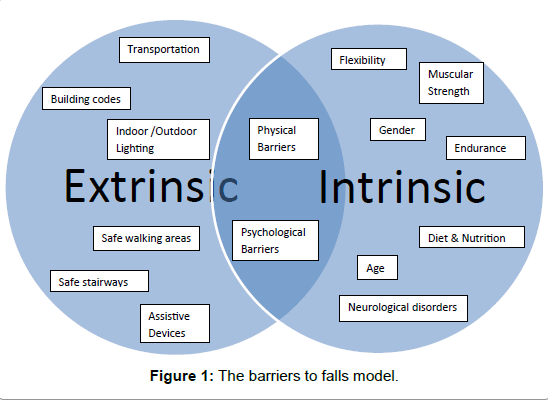
Figure 1:The barriers to falls model.
Repko suggests using a narrative to convey an interdisciplinary understanding by explaining the common ground between the two disciplines.
Mrs. Johnson is an elderly widow who has osteoporosis. She has recently suffered from a stroke, and must now walk to the local store to pick up a few groceries. A public transit strike has given her no choice but to walk in wet and slippery winter conditions. Exhausted from her long and treacherous walk, she finally arrives to the store and notices that there are no grab rails along the entrance ramp and no shopping scooters.
This brief narrative depicts the synergistic effect of intrinsic (age and neurological disorder) and extrinsic factors (transportation, safe walking areas, and assistive devices) that create physical barriers.
Another technique by Repko proposes posing a new question or developing a new avenue of research to express the interdisciplinary understanding. The use of the BTF model generates a new research question in determining which disciplines, other than those mentioned in this paper, are most relevant in investigating determinants of falls resulting in osteoporotic hip fractures.
The identification of determinants of falls resulting in osteoporotic hip fractures is a very complex task. The disciplines of neurology and environmental epidemiology provide significant insight on determinants of falls. Following the steps proposed by Repko [15], an integrated understanding of what causes falls can be achieved by combining disciplinary insights and redefining concepts from neurology and environmental epidemiology. The field of neurology illustrates the role of intrinsic risk factors of falls resulting in osteoporotic hip fractures, while environmental epidemiology identifies the importance of external risk factors. Although this paper provides insights of two separate disciplines, further investigation from other disciplines is necessary for developing a complete understanding of the determinants of falls. The use of a multidisciplinary framework such as the BTF model provides a starting point to identify relevant disciplines that can contribute to future fall and hip fracture prevention programs for osteoporotic patients.
This research was financially supported by the CIHR Doctoral Research Award and the University of Ottawa Excellence Scholarship. The author is indebted to Dr. Mary Egan for her guidance and comments on this publication.