Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2014) Volume 4, Issue 1
Abstract Objectives: Although rare, the pancreatic cystic neoplasms are detected with increased frequency lately. The treatment of these modalities however remains controversial. Methods: In this case reports a multifocal Intraductal Papillary Mucinous Neoplasm (IPMN) along with Pancreatic Serous Cystadenoma (PSC) were identified in the pancreatic specimen following a distal pancreatectomy. The results of the histopathology confirmed the existence of an IPMN inside a large PSC. Results: In our case, the patient with this extremely rare type of mixed cystic neoplasm was managed successfully with extensive distal pancreatectomy. Conclusions: The preoperative evaluation of the extent of the pancreatic involvement and the definition of the histologic type of the involved neoplasms before the pancreatic resection is challenging.
<Keywords: Papillary mucinous neoplasm, Serous cystadenoma, Multifocality
Due to the development of the imaging and endoscopic procedures, an enormous increase in the incidental identification of asymptomatic pancreatic neoplasms has occurred lately during scans for investigations for other modalities [1]. Intraductal Papillary Mucinous Neoplasms (IPMN) and Pancreatic Serous Cystadenomas (PSC) belong to the category of cystic neoplasms which comprise only 1% of the pancreatic cancers [2,3]. Inspite of the evolution in the preoperative evaluation of the patients with these neoplasms, difficulties in the oncologic risk assessment and the operative planning still remain. Distinguishing the invasive IPMN from the benign cases before the operating day is challenging. Moreover the management of - large cysts with almost no malignant potential such as large PSC - IPMNs with multiple involvements of branch ducts is still under debate mainly due to the risk of recurrence as well as the significant rates of complications and the pancreatic functional insufficiency (exocrine and endocrine) that pancreatic resections can cause.
A 83 year old lady presented in our department in June of 2013 with a 2 month history of epigastric pain, weakness and loss of appetite. The pain was getting better after the meals. The results of a gastroscopy one month prior to admission reported the existence of polypoid mobile projection with a diameter of almost 4 cm at the anterior wall of the stomach with normal epithelium giving the impression of the result of external pressure to the gastric wall. No biopsies were taken. The Computed Tomography (CT) scan that followed confirmed the existence of at least 3 pancreatic cystic entities. The larger, located to the tail of the pancreas had a diameter of almost 40 mm whereas the other two were located at the body of the pancreas with diameters 18 and 7 mm respectively. No dilatation of the pancreatic duct was revealed. The patient had another CT of the abdomen 2 years before. The only finding then was the cyst at the tail, which had almost the same size; no other findings had been reported.
From her past medical history she had a history of Chronic Obstructive Pulmonary Disease (COPD), diabetes mellitus, aspergillosis of the left lung, osteoporosis, chronic gastritis and diverticular disease. Two years before, she had undergone endoscopic resection of a polyp of the cecum which was proved to be non malignant.
The first imaging test carried after admission an Endoscopic Ultrasound (EUS) with Fine Needle Aspiration (FNA). The EUS was indicative of a spheric entity with size 45.5 mm×34.2 mm. A biopsy was taken from a small cystic wall projection which was recognized inside this cyst (Figure 1). The cyst was adherent to the splenic vessels and was applying pressure to the gastric wall (confirming the finding of the gastroscopy). Another cyst with similar morphology was detected at the body of the pancreas (19.5 mm×14.9 mm) (Figure 2). The results of the FNA were indicative of IPMN with medium grade epithelial dysplasia.
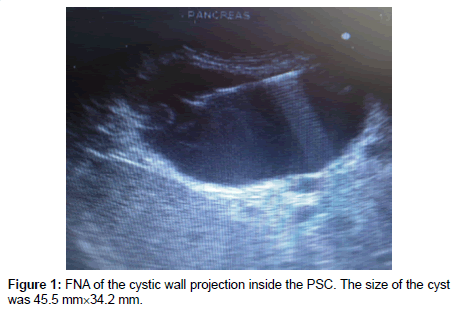
Figure 1: FNA of the cystic wall projection inside the PSC. The size of the cyst was 45.5 mm×34.2 mm.
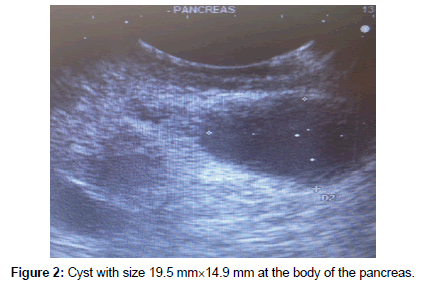
Figure 2: Cyst with size 19.5 mm×14.9 mm at the body of the pancreas.
Almost ten days after the EUS–FNA, an extensive distal pancreatecomy and splenectomy were performed in an open procedure. The histopathological examination showed a specimen of pancreas with size of 12 cm×6 cm×2.5 cm. macroscopically in the tail of the pancreas were identified the following:
i. a cystic lesion of 4.5×4×4 cm filled with a liquid of low viscosity
ii. smaller cysts (max diameter: 0.5 cm) around the main cystic lesion described above
Additionally, in the body of the pancreas were found many cysts with diameter ranging 0.2-1.5 cm, fulfilled with a similar type of liquid.
The microscopical examination revealed: macrosystic variants of serous cystadenoma in the tail both for the main cyst as well as for the smaller cysts closely attached, whereas the vast majority of the cysts in the area of the body were proved to be IPMNs with middle grade epithelial dysplasia. The immunohistological examination was performed with CK7, CK19, CEA, CA19-9, CDX2, MUC1, MUC2, MUC6, MUC5AC and Ki67 which confirmed the abovementioned findings. All the excised lymph nodes (seven) were negative for metastasis.
The postoperative course was uneventful regarding gastrointestinal symptoms and the patient was transfer to a pneumonology clinic due to deterioration of her respiratory function which was attributed to her past medical history and exacerbation of the lung aspergillosis.
Maybe the most interesting finding in our case is the fact that, the results of the cytology that followed the initial FNA were indicative of IPMN whereas the results of the histopathological examination confirms that the cyst from which the sample of the FNA was taken was a PSC. This is an extremely rare case of simultaneous existence of multifocal IPMN and PSC. Multifocality is a novel characteristic of the pancreatic cystic neoplasms. Multiple involvement of the branch ducts along with involvement of the main pancreatic duct has been reported in the literature but the prevalence of this diffused type is still unknown [4,5]. The main duct IPMN carry a significant higher risk of malignancy compared to those located in the side branches. Pancreatic resections have been suggested widely for the managements of these entities due to the malignant potential. The management of PSCs is more challenging, and varies in current practice; very few cases serous cystadenocarcinomas have been described [3]. A diameter of 4 cm or greater and the resulting ‘’pushing’’ effects in organs, such as the stomach in our case, have been discussed as the main reasons for offering patients the choice an operation [1]. The utilization of all the appropriate imaging techniques during the diagnostic work up, along with the intraoperative US for remnant cysts can help the relative complex management of these cases. The available surgical choices at the moment are the Whipple procedure, as well as the distal, the middle and the total pancreatectomy. The immunohistochemical staining on the surgically resected specimens that follows or even on the biopsies following EUS and FNA can help to differential diagnosis of mucinous non neoplastic cysts, IPMN and MCN. The expression frequencies regarding the expression of CK7, CDX2, MUC1, MUC2, MUC6 and MUC5AC vary in small case series [6]. CDX2 and MUC1 seem to be promising for the identification of IPMN and MCN. Moreover MUC1 and HER2 have been reported to be key biomarkers in order to distinguish invasive and non invasive types of IPMN [7].
In spite of the accumulated experience, the morbidity and the mortality of the pancreatic resections remain high; consequently the selection of patients with cystic neoplasms for pancreatectomies should be performed with high level of responsibility and from specialized surgical teams. The patients with IPMNs or PSCs are individuals with benign neoplasms at the time of the operation and as always the benefits should always outweigh the risks.
In this case we presented a very rare type of mixed cystic pancreatic neoplasm with both IPMN and PSC in the pancreatic specimen. The lady was treated with extensive distal pancreatectomy. The post operative course was uneventful until the patient’s admission to the pulmonary clinic. This is the first report, describing such a “mysterious” double type pancreatic cystic neoplasm.