Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Case Report - (2015) Volume 3, Issue 1
Peutz Jegher’s syndrome is a mucocutaneous autosomal dominant condition associated with extensive melanin pigmentation and intestinal hamartomatous polyp formation. It is characterised by round, oval patches of blackish brown pigmentation, irregularly distributed over the oral mucosa, lips, tongue and the hard palate. This condition is associated with an increased risk towards carcinoma and several other complications like small intestine intussusception and anemia. The current case report highlights the oral manifestations of Peutz Jeghers syndrome; also it enumerates the important role played by an oral clinician in the early diagnosis of this inherited syndrome, thereby reducing the morbidity.
Keywords: Peutz Jeghers; Oral melanin pigmentation; Periodontitits; Diabetes mellitus
Peutz-Jegher’s syndrome also known as intestinal hamartomatous polyps in association with mucocutaneous melanocytic macules, was first described by Jegher in the year 1949 as a condition characterized by melanin spots of the oral mucosa, digits and lips [1]. The incidence of the following condition is 1 in 30,000-12,000 live births without any form of race or gender predilection [2]. Peutz Jegher’s syndrome is an autosomal dominant inherited disorder with a familial history, however it has been seen that most of the cases are sporadic in nature and they do not show any familial predilection. The cause for Peutz Jegher’s syndrome appears to be a germline mutation of the STK11 (Serine threonine kinase 11) gene in most cases [2]. The oral lesions essentially represent an extension of the perioral freckling, with a diameter of 1-4 mm brown to blue-gray macules primarily affect the vermilion zone, the labial and buccal mucosa and the tongue. The number of lesions and the extent of involvement can vary markedly from patient to patient. The oral manifestations of this condition may precede the occurrence of hamartomatous polyps, early diagnosis of such a condition in a dental setting may act as a boon in recognizing systemic life threatening conditions like short bowel intussusception, carcinomas of the gastro intestinal tract if present [3]. The following case report with periodontitis depicts extensive oral melanotic manifestations in a patient diagnosed with Peutz Jegher’s syndrome.
A 65 year old female patient reported to the Department of Periodontics, presenting with a chief complaint of pigmentation and burning sensation in relation to the oral cavity since the past two months (Figure 1). On clinical examination patient presented with clinical signs and symptoms of periodontitis, showed the presence of multifocal blackish brown pigmentation on the peri oral area. The onset of the pigmentation was sudden and was severe especially with inner surface of the lower lip and the buccal mucosa bilaterally (Figure 2).

Figure 1: Extra oral photographs showing heavily pigmented peri oral region
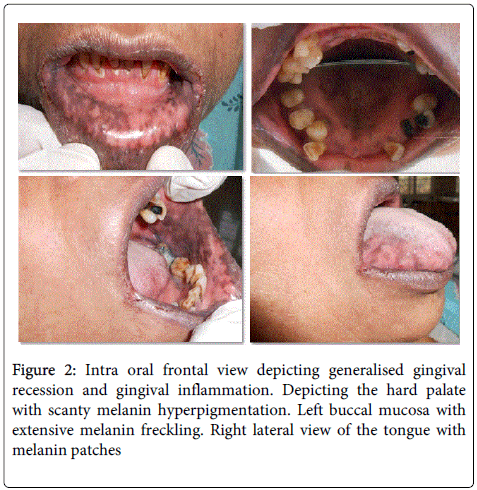
Figure 2: Intra oral frontal view depicting generalised gingival recession and gingival inflammation. Depicting the hard palate with scanty melanin hyperpigmentation. Left buccal mucosa with extensive melanin freckling. Right lateral view of the tongue with melanin patches
Melanin freckling was present on the palate and the lateral borders of the tongue. The patient also presented with angular cheilitis leading to bleeding at the commissures of her mouth. The increased amount of mucocutaneous pigmentation can be attributed to the increased number of melanocytes leading to an increase in the production of melanin.
The patient complained of generalised weakness since the past two months and had a medical history of hypertension and diabetes since the past three years.
On the basis of clinical examination and medical history she was given a differential diagnosis of Peutz Jeghers syndrome.
The patient was rendered non-surgical periodontal therapy, was prescribed 0.1% Triamcinolone acetonide gel 3-4 times daily for the burning sensation of the oral cavity and was referred to the medical hospital for consent for the further treatment.
Medical Examination
Endoscopic examination revealed an absence of intestinal polyposis. Haematological and general thyroid investigations showed haematocrit values and T3, T4, TSH levels within the normal range. The Anti TPO test showed abnormally high levels (129.1) when compared to normal. The test revealed increased levels of serum auto antibodies, with confirmation of diagnosis as Peutz Jeghers syndrome. The patient was referred to the Department of Periodontics from the Department of Internal Medicine, with prescription of parenteral multi vitamin supplements to treat her underlying condition of burning sensation in the oral cavity.
The pigmented lesions seen in relation to the peri oral and oral cavities are important entities as they may serve as initial manifestations of rather severe debilitating conditions like carcinomas [4]. Peutz Jegher’s syndrome being autosomal dominant in nature can be inherited or can be sporadic in nature. In the current case, the patient experienced the onset of the pigmentation over a period of two months. The lesions appeared as small blackish brown macules, 1-2 mm in size. This macules located on the buccal mucosa may persist throughout life, if the onset is sporadic in nature, as it is with the present case. Mucocutaneous melanin pigmentation occurs in more than 90% of the patients. The cause for this can be co related to the mutation in the serine threonine kinase 11 gene. These oral macules were benign and no malignant transformation was present [5]. Intestinal polyposis which is considered as a cardinal sign of Peutz Jeghers syndrome was absent in this case, also the patient did not present with any familial aggregation of this condition. In the present case, anti TPO antibodies were assessed in the patient, results showed rather high anti TPO levels. High anti TPO levels indicate an incline towards hyperthyroidism. Anti-thyroid antibodies are used to track the presence of autoimmune thyroiditis, they are generally not considered to contribute directly to the destruction of the thyroid [6]. There was an increase in serum auto antibody levels. Peutz Jegher which is syndromic in nature is generally associated with aggressive periodontitis, but in the current case , the patient presented with chronic generalized periodontitis with an underlying case of diabetes mellitus and was on medication for the same [6,7]. The periodontal treatment, aided in elimination of pathogenic micro-organisms, and thus decreased the inflammation. And as a consequence, there is a reduction of insulin resistance and an increased sensitivity to insulin and improvement in glycemic control.
Other disorders that mimic the clinical presentation of Peutz Jegher’s syndrome may include Gardner’s syndrome, Carney’s syndrome, Addison’s disease, drug induced pigmentation [3].
The knowledge of the oral manifestations and the systemic complications are important to a oral health care provider. Thus a thorough medical and dental history, and incidental findings such as mucocutaneous pigmentation may help in identifying this condition and the patient can get appropriate guidance towards a specialist to treat the same.