Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Case Report - (2016) Volume 6, Issue 2
The nodule of Sister Mary Joseph is a cutaneous metastasis of an intra-abdominal cancer. Herein, we report a case of a 57 years old female, who had a four months history of an umbilical nodule. The paraclinical investigation showed a cutaneous metastasis of a colon adenocarcinoma, with peritoneal carcinomatosis and a hepatic metastasis. Patient underwent a palliative chemotherapy with a fatal evolution after the second cure. Through this case report, we highlight the importance of an active search for an underlying neoplasm in front of an umbilical nodule.
Keywords: Sister Mary Joseph's nodule; Umbilical metastasis; Colon adenocarcinoma
The umbilical cutaneous metastasis of visceral tumors is rare, they are known as “the Mary Joseph's nodule”. Herein, we report a new case of an umbilical nodule revealing a metastatic colon adenocarcinoma.
A 57 years old female, who presented with a four months history of a reddish and firm umbilical nodule, which gradually increased in size and pain (Figure 1). The histopathological finding showed a cutaneous metastasis of a well-differentiated adenocarcinoma partially mucinous, CK20+ (Figures 2 and 3). Colonoscopy showed a budding tumor, the biopsy confirmed the primary origin of the adenocarcinoma. CT showed a widespread peritoneal carcinomatosis with hepatic metastasis (Figure 4). A palliative chemotherapy with capecitabine, oxaliplatin and bevacizumab was indicated. The patient died two weeks after the 2nd cure of chemotherapy.
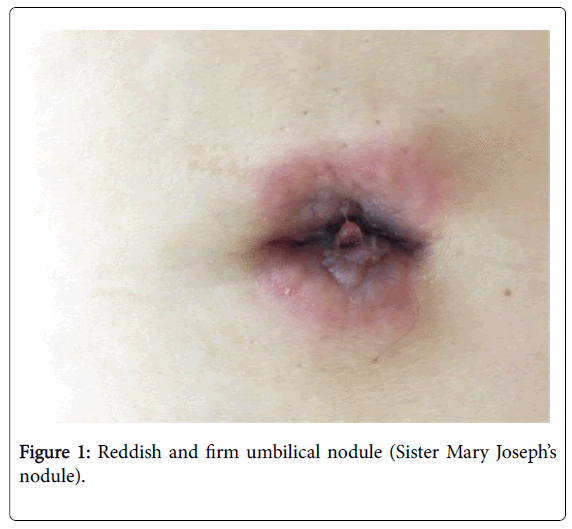
Figure 1: Reddish and firm umbilical nodule (Sister Mary Joseph’s nodule).
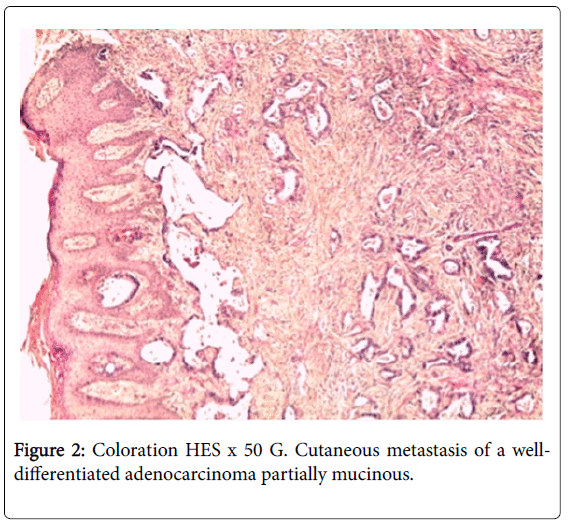
Figure 2: Coloration HES х 50 G. Cutaneous metastasis of a welldifferentiated adenocarcinoma partially mucinous.
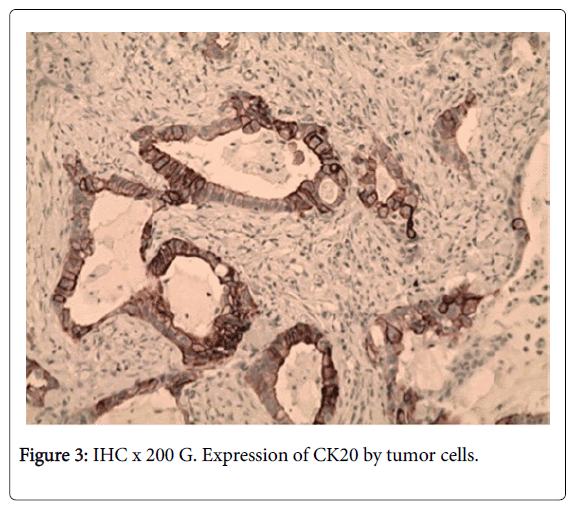
Figure 3: IHC х 200 G. Expression of CK20 by tumor cells.
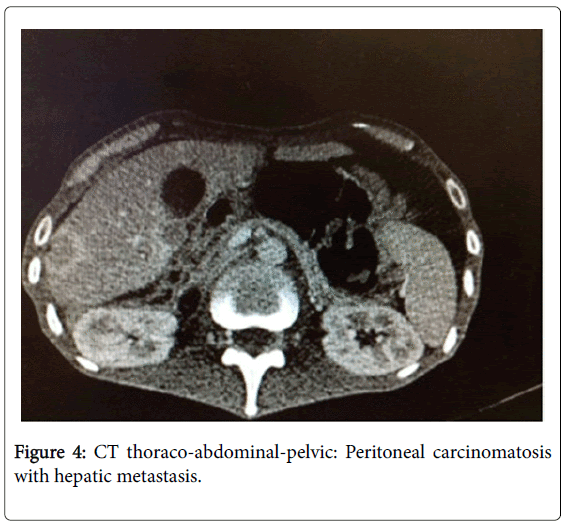
Figure 4: CT thoraco-abdominal-pelvic: Peritoneal carcinomatosis with hepatic metastasis.
Mary Joseph's nodule is usually associated with gastrointestinal tract cancer and ovarian carcinoma. This nomination refers to Sister Mary Joseph, a catholic nurse who worked with the Mayo brothers, and who noticed that patients with terminal carcinoma sometimes developed red papular lesions in the umbilicus [1]. Several hypotheses explain the tumorigenesis of this nodule. Indeed, neoplastic cells can disseminate into the umbilicus through different mechanism: a hematogenous spread; or an extension from the liver round ligament, by contiguity through the dermal vessels of the navel; and finally a retrograde lymphatic flow mechanism [2].
The clinical presentation is an indurated and irregular painless nodule, with variable diameter (typically less than 5 cm), often with a vascular appearance. The surface can be fissured or ulcerated with hemorrhagic, mucinous, serous, or purulent discharge. The histological findings confirm the diagnosis of an adenocarcinoma in 75% of cases, rarely squamous cell carcinoma, and undifferentiated cancer or carcinoid tumors. Primary neoplasms have usually an abdominoperineal origin (ovarian, endometrial, cervix, pancreas, and biliary tract, gastrointestinal or genitourinary tumors). Nevertheless, in 10-30 % of cases, the primary tumor remains unknown. Till now, there isn’t a well-defined consensus on treatment. However, surgery combined with a chemotherapy treatment have improved survival [3,4]. Mary Joseph’s nodule have a poor prognosis, the average survival after the onset of umbilical metastasis is about six months [3].
In summary, an umbilical nodule is easily accessible to clinical examination, its recognition as a secondary lesion of a primary abdominoperineal cancer can enable early diagnosis and treatment.