Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 1
Introduction: New-onset left bundle branch block (LBBB) in the electrocardiogram (ECG) is considered to be a particularly serious condition, which requires prompt further evaluation for the exclusion of possible underlying myocardial ischemia. . Case presentation: A 76 year old female Caucasian patient presented with gradually worsening abdominal discomfort, accompanied by nausea and vomiting. Initial clinical and laboratory investigations were indicative of acute pancreatitis, which was confirmed with an abdomen ultrasonography. A routine ECG, which was performed in the second day of hospitalisation, identified new-onset LBBB morphology, which was not initially present. The possibility of a rate-dependent LBBB was immediately excluded, since no significant alteration of the heart rate was noted. Considering the fact that myocardial infarction among elderly female individuals may present with non-typical features, a serious diagnostic problem appeared. Since there were no echocardiographic or biochemical indications consistent with acute myocardial ischemia it was decided to continue the medical treatment without alterations. The transthoracic echocardiogram also excluded the presence of significant valve lesions or any abnormalities in the structure and function of the myocardium. An ECG was repeatedly performed on a daily basis, but the LBBB persisted until the patient was discharged, seven days after admission, with a diagnosis of acute idiopathic pancreatitis. About three weeks after discharge, a re-evaluation was arranged. The patient reported no symptoms, without any deterioration of functional status. Also, disappearance of LBBB pattern was noted on the ECG. A myocardial perfusion scintigraphy was also carried out, at both rest and stress, without evidence of infarction or inducible ischemia. Conclusion: Acute pancreatitis can present with several ECG abnormalities, but the presence of transient LBBB in this setting is not considered very common. In fact, most of the times it seems to be correlated with electrolyte disturbances. The case presented here is regarded unique since no electrolyte abnormalities were present and a longer duration was noted. The proposed explanation and pathogenetic mechanism of this clinical manifestation is transdiaphragmatic epicardial irritation secondary to acute pancreatitis. It remains to be established by repeated assessment of the patient, whether this intermittent finding is associated with poor long-term outcome.
<New-onset left bundle branch block (LBBB) in the electrocardiogram (ECG) is considered to be a particularly serious condition, which requires prompt further evaluation for the exclusion of possible underlying myocardial ischemia [1]. A quick patient assessment is always mandatory, since often coronary reperfusion needs to be performed urgently. Although, newly presented LBBB in combination with chest discomfort has been traditionally associated with acute occlusion of left anterior descending artery, recent findings indicate that stable patients with such finding need to be managed with a more judicious approach [2].
A 76 year old female Caucasian patient presented with gradually worsening abdominal discomfort, accompanied by nausea and vomiting. Initial clinical and laboratory investigations were indicative of acute pancreatitis. The suspicion of the above diagnosis was confirmed with an abdomen ultrasonography, in which the pancreas was described to be hypertrophic and non-homogeneous with focal areas of oedema and necrosis. No cholelithiasis was revealed with abdomen ultrasonography. The patient was transferred to the Internal Medicine Ward for intravenous hydration, monitoring of vital signs and further inpatient care according to the development of any complications. Initial respond to the medical treatment was suggested to be particularly good, since the patient soon reported resolution of symptoms. Initial ECG was in sinus rhythm with a heart rate (HR) of 65 beats per minute (Figure 1). A normal electrical heart axis was present with normal PR interval, normal QRS duration, normal progression of R waves, normal QT segment and no significant deviation of ST segment. However, a routine ECG, which was performed in the second day of hospitalisation, identified a new-onset LBBB morphology, which was not initially present (Figure 2). The possibility of a rate-dependent LBBB was immediately excluded since no significant alteration of the HR was present. Considering the fact that myocardial infarction among elderly female individuals may present with non-typical features, a serious diagnostic problem appeared [3,4].
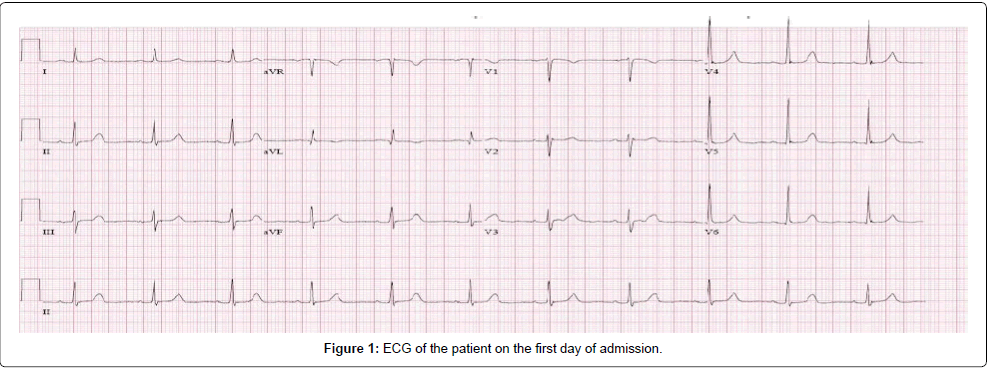
Figure 1: ECG of the patient on the first day of admission.
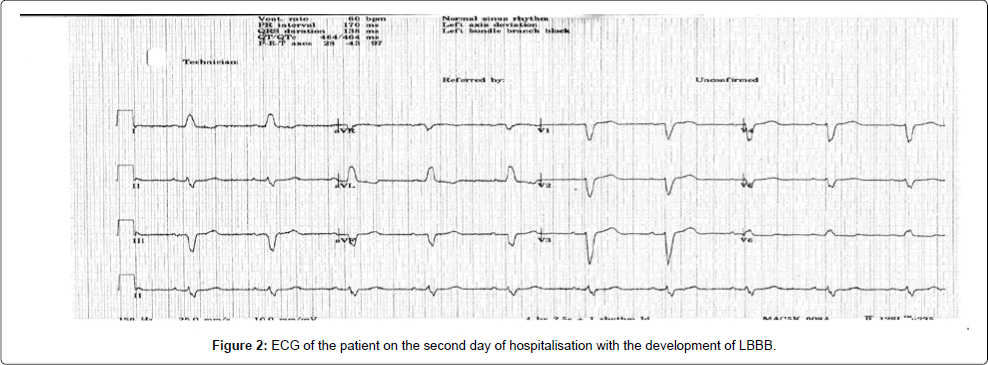
Figure 2: ECG of the patient on the second day of hospitalisation with the development of LBBB.
Urgent transfer of the patient to the coronary care unit was arranged. It is always imperative to manage such patients with suspected acute coronary episode in a setting where continuous monitoring is established, since malignant arrhythmias may occur. Immediate access to resuscitation equipment, including defibrillator and ventilator machine, also needs to be ensured. Initial physical investigation of the patient by the cardiologist identified no abnormal findings, apart from mild epigastric tenderness on deep palpation. The vital signs of the patient were within normal range without significant alteration in comparison with the day of admission. Two consecutive sets of biochemical markers of myocardial injury, including measurement of serum troponin T, were negative. Also, no electrolyte alterations were present. The transthoracic echocardiogram which was urgently performed identified no regional wall motion abnormalities. However paradoxical septal wall motion was noted, presumably due to the bundle branch morphology. Furthermore, no abnormalities in the myocardial structure and no pericardial effusion were detected. No significant valve abnormalities and no evidence of acute aortic syndrome were noted. The above echocardiographic indications were consistent with the absence of acute myocardial ischemia. Therefore it was decided to continue the medical treatment without alterations.
An Endoscopic Retrograde Cholangio Pancreatography (ERCP) was performed without any identified aetiology for the patient’s condition. An ECG was repeatedly performed on a daily basis, but the LBBB persisted until the patient was discharged, seven days after admission, with a diagnosis of acute idiopathic pancreatitis. About three weeks after discharge, a re-evaluation was arranged. The patient reported no symptoms, without any deterioration of functional status. Also, disappearance of LBBB pattern was noted on the ECG with complete resolution back to its initial morphology. A Single Photon Emission Tomography (SPECT) myocardial perfusion imaging study was also carried out in both rest and stress, with the use of technetium 99m labelled tracer. No perfusion defects were identified, confirming the absence of a previous infarction or inducible ischemia.
Transient LBBB can be encountered in several clinical entities [5-7]. ECG abnormalities in the setting of acute pancreatitis are reported to be quite often [8]. Changes in the morphology of T wave, ST segment deviation, conduction abnormalities, atrial extrasystoles and transient intraventricular conduction disturbances have been previously reported. A significant proportion of those ECG abnormalities were correlated with electrolyte alterations. Acute pancreatitis which resembled an acute coronary episode with the presence of transient new-onset LBBB has also been reported [9,10]. In most similar cases described in the literature the presence of underlying myocardial disease was based on measurement of cardiac enzymes. In the case presented here, a thorough assessment was performed, including consecutive transthoracic echocardiograms and a myocardial perfusion imaging study, which all excluded the presence of underlying coronary artery disease. It is also regarded unique from the aspect of longer duration of the ECG abnormality. A proposed explanation and pathogenetic mechanism of this clinical manifestation could be transdiaphragmatic epicardial irritation secondary to acute pancreatitis. It remains to be established by repeated assessment of the patient, whether this intermittent finding is associated with poor long-term outcome. Considering the fact that in the setting of acute pancreatitis, coronary angiography may induce further renal deterioration with the implementation of contrast, a myocardial perfusion imaging study is ideal for definite exclusion of underlying ischemia.
This clinical scenario clearly illustrates that clinical and laboratory findings can sometimes be misleading. Diagnostic problems are occasionally very stressful, particularly when time constraint exists. In order to manage such unique cases a physician should appropriately use clinical judgement. The implementation of several diagnostic modalities can often be very assisting. Also, the importance of traditional clinical skills such as a thorough physical examination and a detailed history should never be neglected. This particularly case report is definitely didactic about the broad spectrum of presentations of a clinical condition.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
IP was responsible as an attending cardiologist to exclude the presence of underlying myocardial ischemia. CP performed and interpreted the myocardial perfusion scintigraphy. EN as the head of the department was supervising. All authors read and approved the final manuscript.
We would like to thank our patient for allowing use of her clinical and laboratory information for publication.