Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2016) Volume 5, Issue 4
Introduction: Phyllodes tumours are rare neoplasms, representing less than 1% of all primary tumours of the breast.
Case report: We report the case of a woman who presented with a malignant phyllodes tumour of the breast, with an osteosarcomatous component. A year after surgery, a control thoracic CT scan revealed nodules in the lung. Shortly after, she also developed cardiac and dermo-hypodermic lesions, histologically characterized as angiosarcoma with an osteoclastic component.
Discussion: Malignant breast phyllodes tumour often metastasizes to the lungs, bones, liver and brain. To the best of our knowledge, there is only one case in literature that reports a cutaneous metastasis of phyllodes tumour under the form of an angiosarcoma, whilst, to date, no such myocardial involvement has been reported.
Keywords: Metastases; Angiosarcomatoid; Breast tumor; Phylloides tumor
Phyllodes tumours (PTs) are very rare neoplasms, representing less than 1% of all primary tumours of the breast [1,2]. A dual population of epithelial and mesenchymal components, as well as a variable clinicopathological behaviour, are the main characteristics of these tumours. In fact, PTs range from benign to malignant lesions. The ductal component is usually benign, whereas malignancy develops in the mesenchymal portion of phyllodes tumour, which can contain liposarcomatous, leiomyosarcomatous, chondrosarcomatous, osteosarcomatous and/or angiosarcomatous constituents, singly or variably admixed [3,4]. Malignant PT most commonly metastasizes to the lungs and to the bones [4]. We present a case of malignant PT of the breast metastasising to the skin and to the heart. To the best of our knowledge, this is only the second case reported in English literature regarding skin metastasis from malignant PT [5], and the first one with cardiac repetitions.
We report a case of a 58-year-old woman who arrived at our hospital with a lump in her left breast. She referred to have undergone an operation for a fibroadenoma in the same breast twenty years earlier. She had no familiarity for breast carcinoma.
On physical examination, there was an area of cutaneous retraction in the superomedial quadrant, with an underlying palpable nodule. Ultrasonography and mammography and total body CT confirmed the presence of a solid lesion, measuring 35 mm in greatest axis, poorly delimited, partly necrotic, calcified and hypervascularized. There were no thoracic or abdominal lymphadenopathies, nor secondary lesions elsewhere. Fine-needle aspiration cytology was performed, yielding numerous atypical cells, often multinucleated, sometimes forming aggregates reminiscent of vascular structures, highly suggestive of angiosarcoma. The patient underwent a simple left mastectomy, followed by adjuvant chemotherapy.
Grossly, the lesion was greyish, solid and polylobate, with some cystic areas and foci of haemorrhage. Histologically, there was a mixed population of both epithelial and stromal cells. The epithelial component was benign, while a heterologous population of highly atypical cells, with a high mitotic index, characterized the stroma. The neoplastic cells were immunoreactive for CD68, p53, AE1/AE3 and were negative for EMA, S-100, MAC387, FACTOR VIII, Cerb-B2, EGFR; Ki67 labelling index was 20%. The diagnosis was a malignant phyllodes tumour with an osteosarcomatous component.
One year after the operation, a thoracic CT scan revealed two nodules in the superior lobe of the right lung, 8 mm and 18 mm respectively in greatest diameter, highly suspicious of secondary lesions, whose position did not allow surgical removal. Shortly after, the patient developed restrictive cardiomyopathy; MRI showed cardiac lesions compatible with metastases. Fifteen months after the operation, the patient returned to hospital due to progressive worsening of her condition. She had a subcutaneous nodule in the forehead, which was excised. Histological examination of the lesion showed the presence of a dermo-hypodermic epithelioid angiosarcoma with an osteoclastic component, compatible with metastasis from a malignant phyllodes tumour. The patient passed away two months later (Figures 1 and 2).
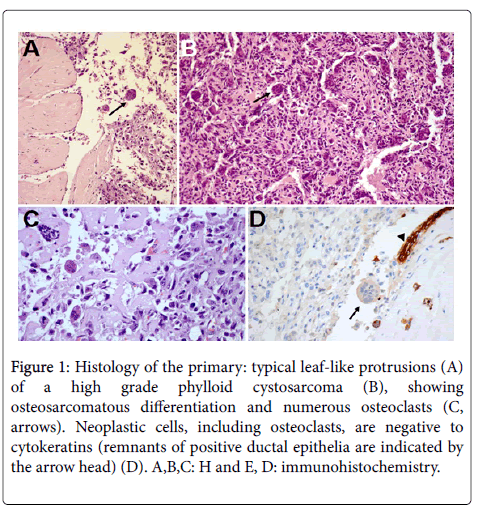
Figure 1: Histology of the primary: typical leaf-like protrusions (A) of a high grade phylloid cystosarcoma (B), showing osteosarcomatous differentiation and numerous osteoclasts (C, arrows). Neoplastic cells, including osteoclasts, are negative to cytokeratins (remnants of positive ductal epithelia are indicated by the arrow head) (D). A,B,C: H and E, D: immunohistochemistry.
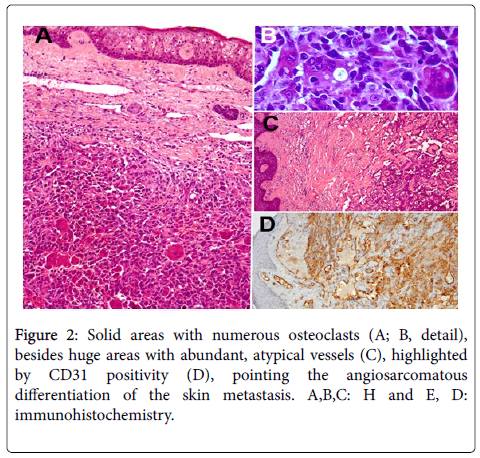
Figure 2: Solid areas with numerous osteoclasts (A; B, detail), besides huge areas with abundant, atypical vessels (C), highlighted by CD31 positivity (D), pointing the angiosarcomatous differentiation of the skin metastasis. A,B,C: H and E, D: immunohistochemistry.
In 1981, the WHO divided PTs into three categories: benign (35% - 65%), borderline (low-grade malignancy 11% - 40%) and malignant (18% - 35%), depending on histological characteristics, especially those of the stromal component, and biological behaviour. Negative prognostic factors are the presence of infiltrated margins, high mitotic activity and marked cytological atypia of the mesenchymal elements.
The concept of a fibroepithelial tumour has been clearly established and the differences between PTs and sarcomas are well defined in literature [6]. However, these neoplasms are still considered tumours of the connective tissue because it is the stromal cellular component which undergoes malignant transformation. As for other mesenchymal tumours of the mammary gland, PTs occur most frequently in the 4th and 5th decades, but, unlike breast sarcomas, their origin is not linked to previous radiotherapy [7-10]. In our paper, we present a particular setting: malignant phyllodes tumour of the breast metastasising in very unusual sites: skin and heart.
To date, the etiopathogenesis of PT is not completely understood. No predisposing factors have been identified. In some cases, p53 mutation has been identified [11] and this can explain the pathogenesis of the tumours occurring in the context of an alteration of the germinal line (Li-Fraumeni syndrome). Some studies [12-14] have suggested that there may be a hormonal trigger that causes a fibroadenoma to progress towards a PT, through the mutation in an Xlined gene that encodes for an androgen receptor. Our patient, in addition to 37% of the female population studied at the Memorial Sloan Kettering Cancer Center [14], reported a history of fibroadenoma preceding the diagnosis of the phyllodes tumour. Another hypothesis that could explain the mechanism that initiates the development of PT seems to be a loss of balance in the interaction between stroma and the epithelium, due to an uncontrollable growth of the mesenchymal component, which becomes progressively independent from the ductal epithelium, assuming malignant features [15,16].
Malignant transformation of the stromal component in PT determines the formation of sarcomatous lesions: more often fibrosarcomas, liposarcomas and rhabdosarcomas, and rarely chondrosarcomas, osteosarcomas and angiosarcomas [17]. Even the capacity to metastasise depends solely on the stromal component. In our case, the cutaneous metastasis presented itself in the form of an angiosarcoma with an osteosarcomatous component, a feature which had also been identified in the primary tumour.
The sites mostly affected by metastasis from phyllodes tumour are lung, bone, liver and brain. Rare involvement of serous cavities and soft tissue, especially skin, has been reported [18]. In literature, only one case of phyllodes tumour has been described to have determined a metastasis in the form of cutaneous angiosarcoma [5], whilst, to the best of our knowledge, no myocardial involvement has been reported.
Unfortunately, it was not possible to ascertain whether the cardiac lesions were metastases from phyllodes tumour since, in the light of the poor conditions of our patient, it was not possible to carry out a myocardial biopsy.
PTs usually have a high percentage of local recurrence. In our patient, however, this was not the case. Usually, these tumours rarely present lymph node involvement. Recommended treatment consists of surgical excision of the lesion, with particular attention to obtaining disease-free margins [16]. In our case, total mastectomy was preferred because of the local extension of the tumour and the apparent involvement of the skin. There is little controversy about chemotherapy. For some authors, it is not recommended especially in localised and well-resected low-grade tumours. For metastasising tumours, treatment is based mainly on chemotherapy using conventional drugs for sarcoma [19,20]. In our opinion it is also very important a strict follow-up, in order to prevent any possible recurrence early. This case report is very anecdotal for the rare presentation of the metastases sites, in particular for cardiac lesion.
In conclusion we recommend for breast PT with malignant characteristics to perform a radical surgery of the primary lesion and a strict follow-up, in order to prevent any possible metastasis, event in rare locations, such as the skin and the heart. Chemotherapy is controversial in these cases.