Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2014) Volume 4, Issue 2
Search of etiologies of acute pancreatitis (AP) is important but guidelines or recommendations are limited. In this review, the author summarized the common causes, how to diagnose them, how to address them as a cause of AP and proposes a practical 8-step approach to search the etiologies of AP
<Keywords: Acute pancreatitis, Hypertriglyceridemia, Hypercalcemia, Vasculitis
Acute pancreatitis (AP) is an important abdominal emergency which carries significant morbidity and mortality. There are varieties of etiologies that can account for AP (Table 1). Appropriate search of the etiologies of AP is essential due to the 2 reasons. First, some etiologies may need prompt intervention during the course of AP e.g. gallstone, hypertriglyceridemia, hypercalcemia and vasculitis, etc. Second, the identified causes can be eliminated to prevent further attack.
| Etiologies | Approximate frequency (%) |
|---|---|
| Common | |
| Alcohol | 30-40 |
| Gallstone | 30-40 |
| Idiopathic | 10-20 |
| Less common | 10-20 |
| Iatrogenic (post-ERCP, post-FNA, post-balloon-assisted enteroscopy) | |
| Hypertriglyceridemia | |
| Hypercalcemia | |
| Drugs | |
| Neoplasms | |
| Uncommon causes of pancreatic duct obstruction (choledocholcele, pancreas divisum, sphincter of Oddi dysfunction) | |
| Infections | |
| Vasculitis | |
| Ischemic |
ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasonography; FNA, fine needle aspiration
Table 1: Common etiologies of acute pancreatitis
Despite the importance, there are limited guidelines and recommendations regarding how to search the etiologies of AP appropriately [1-3]. In this review, the author will review, summarize the common causes, how to diagnose and address them as a cause of AP and propose a practical 8-step approach to search the etiologies of AP.
Common etiologies of AP and the frequencies are showed in Table 1
Alcohol
Alcohol is a well-known cause of chronic pancreatitis. However, it is not such straightforward in AP. Most studies on alcoholic AP showed that most patients had chronic use of alcohol (no single heavy binge can cause AP) but the doses of alcohol were usually increased more over a couple weeks before the attack [4,5]. However, there is no exact threshold dose of alcohol to initiate AP [6]. The attack of AP usually had 12-48 hours delay after the last binge (“the afternoon after the night before”) [4]. Thus, in patient with AP and history of drinking, it is sometimes difficult to judge whether this alcohol is enough to cause AP.
It is unclear whether other etiologies of AP should still be sought in patients who already had history of heavy drinking. In the author’s study of 78 patients with first episodes of AP, 58% of the patients drank alcohol for >80 g per day for >5 years. However, a thorough search demonstrated that 29% of these alcoholic patients had gallstones and hypertriglyceridemia, which could also be the causes of AP [7]. It may be difficult to tell which one was the real culprit. However, the author believes that if the other causes are found besides alcohol, they should also be counted and treated. Results of the author’s may support the strategy to exclude other common causes of AP before accusing the alcohol as a cause of AP.
Gallstone
The principle event that initiates gallstone pancreatitis is gallstone migration through the papilla [8]. Most of the gallstones (80%) have already passed and no longer been in the common bile duct. The most sensitive method to identify gallstone as a cause of AP is the combination of a 3-fold elevation of alanine transaminase (ALT) above upper normal limit and ultrasonography (US) of the gallbladder. Early meta-analysis reported that a 3-fold-elevated ALT had a sensitivity of 50% but a positive predictive value (PPV) of 95% for gallstone pancreatitis [9]. More recent studies showed the sensitivity and PPV of the 3-fold elevated ALT were 90% and 100%, respectively in one study [10] and 61% and 92%, respectively in another study [11]. Combination of ALT and US was shown to have the highest sensitivity of 98% and the highest PPV of 100% [10]. Therefore, every current guideline on AP recommends checking ALT and performing US in every AP patient within the first 1-2 days after admission [1,2,12-14].
Iatrogenic
AP can be caused by many gastrointestinal procedures i.e. endoscopic retrograde cholangiopancreatography (ERCP), endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of the pancreas and balloon-assisted enteroscopy. The incidence of post-ERCP pancreatitis is 2-9% [15] and post EUS-FNA pancreatitis is 0.4% [16]. In balloon-assisted enteroscopy, AP occurred in 0.2-0.5% after double-balloon enteroscopy (most performed via antergrade route) [17,18]. For single-balloon enteroscopy, there is only 1 case report [19]. The diagnosis of post-procedure pancreatitis is usually easy by the occurrence of AP within 24 hours after the procedures.
Hypertriglyceridemia
Hypertriglyceridemia, either primary or secondary, can cause AP. The most widely-accepted minimal level of triglyceride that can initiate AP is 1,000 mg/dL [20,21]. However, this number is rather arbitrary and not proven. Furthermore, many genetic mutations have now been shown to associate with the risk of pancreatitis e.g. protease serine 1 (PRSS1), serine protease inhibitor Kazal type 1 (SPINK1), cystic fibrosis transmembrane conductance regulator (CFTR), chymotrypsin C (CTRC) and calcium sensing receptor (CASR) mutations [22]. Recent study demonstrated that some hypertriglyceridemic pancreatitis patients actually have CFTR mutations [23]. The important point is that serum triglyceride level should be measured as soon as possible after admission in all cases of AP [24] because the level may fall rapidly after fasting [25].
Hypercalcemia
Hypercalcemia-induced pancreatitis usually occurred in the setting of undiagnosed hyperparathyroidism. No threshold level of serum calcium has been identified and there is study shown the presence of CFTR and SPINK1 mutation in one third of patients with AP from hyperparathyroidism [26]. Serum calcium should be measured in every patient with AP [24] as soon as possible after admission because the calcium level may fall after intravenous fluid replacement and in case of severe AP.
Drugs
Lists of drug-induced pancreatitis have been recently reviewed by Badalovet al. [27] and Nitsche et al. [28] It is the author’s belief that only drugs that have been classified as “definite” (has recurrence after re-challenge) should be counted as a cause of AP (Table 2). Furthermore, the other more common causes of AP, i.e. gallstone, hypertriglyceridemia and hypercalcemia should also be excluded before concluding the cause as drug-induced pancreatitis.
| Acetaminophen |
| All-trans-retinoic acid |
| Amiodarone |
| L-asparaginase |
| Azathioprine |
| Azodisalicylate |
| Bezafibrate |
| Bortezomib |
| Cannabis |
| Capecitabine |
| Carbamazepine |
| Carbimazole |
| Clomiphene |
| Cimetidine |
| Cisplatin |
| Codeine |
| Cytarabine |
| Dapsone |
| Dexamethasone |
| Didanosine |
| Enalapril |
| Erythromycin |
| Estrogens |
| Hydrochlorothiazide |
| Furosemide |
| Ifosfamide |
| Interferon-a 2b |
| Isoniazid |
| Itraconazole |
| Lamivudine |
| Losartan |
| 6-mercaptopurine |
| Meglumine |
| Mesalamine/olzalazine |
| Methimazole |
| Methyldopa |
| Metronidazole |
| Nelfinavir |
| Octreotide |
| Olanzepine |
| Omeprazole |
| Opiate |
| Oxyphenbutazone |
| Pentamidine |
| Phenformin |
| Pravastatin |
| Procainamide |
| Pyritonol |
| Simvastatin |
| Steroids |
| Stibogluconate |
| Sufamethoxazole/co-trimoxazole |
| Sulfasalazine |
| Sulindac |
| Tamoxifen |
| Tetracycline |
| Valproic acid |
Table 2: Definite drug-induced AP (adapted from Bodalov et al. [27] and Nitsche et al. [28])
Neoplasms
The 3 most common types of neoplasm that cause AP are ampullary neoplasm (25% have AP) [29], intraductal papillary mucinous neoplasm (IPMN, particularly main duct type, 7% have AP) [30] and pancreatic ductal adenocarcinoma (5% have AP) [29], respectively. Pancreatic intraepithelial neoplasia (panIN) is a well-established precursor of pancreatic neoplasm but the lesion is usually small (<0.5 cm) [31] and there is no report to associate with AP. Therefore, it is recommended to perform computed tomography (CT) in every patient >40 years of age (if no other causes of AP has been identified) because one study has shown to identify neoplasms in a significant proportion after this age [32].
Unusual or controversial causes of pancreatic duct obstruction
There are some unusual or controversial causes of pancreatic duct obstruction that may cause AP. Some congenital anomalies (e.g. choledochocele, annular pancreas, etc) may associate with AP. Pancreas divisum is a controversial cause of AP and recurrent AP and has been critically reviewed [33,34]. Sphincter of Oddi dysfunction (SOD) is an even more controversial cause of AP and recurrent AP [35,36]. Since congenital anomalies are rare and pancreas divisum and SOD are controversial, the search of these conditions should be preserved for patients with recurrent AP, not after the first attack of AP.
Infections
There are varieties of infections that can cause AP and have been systemically reviewed by Parenti et al. [37]. In summary, they include viruses (HIV, cytomegalovirus, herpes simplex, hepatitis B, mumps, varicella-zoster, coxsackie B and echoviruses), bacteria (salmonella, leptospira, legionella, mycoplasma, rickettsia), fungi (aspergillus), parasites (ascaris) and protozoa (cryptosporidium, toxoplasma, malaria). The diagnoses are usually based on characteristic signs and symptoms of particular infections at the time of AP [37].
Vasculitides
AP due to vasculitides has been reported in systemic lupus erythematosus [38,39], polyarteritisnodosa [40], Wegener granulomatosis [41], Henoch-Schönleinpurpura [42] and Behcet disease [43]. Diagnosis is usually done by the presence of AP during the setting of these active diseases.
Ischemic
Ischemic AP is difficult to diagnose because it may be the result rather than the cause. However, it has been reported in patient post cardiac arrest [44]. In facing with AP patient who has shock or hypotension, other causes of AP should be ruled-out thoroughly before labeling it as ischemic AP.
Current guidelines suggest that the proportion of AP patients who would be labeled as idiopathic AP should be <10-20%. Thorough history taking, specific work-ups of the etiologies described above should be attempted and will elucidate the cause of AP in approximately 80-90% of the cases [7]. If no cause can be identified, EUS is recommended [45]. EUS may discover small gallstone, common bile duct stone, microlithiasis, small ampullary or pancreatic neoplasms and early chronic pancreatitis that could be presented as AP. Alternatively, MRCP can also be used although there is no comparison study to EUS. ERCP, due to the invasiveness, should be second to EUS [46] and preserved for recurrent AP or in case EUS or MRCP are unavailable.
The author had used this thorough approach in the author’s institution and could reduce the diagnosis of idiopathic AP down from 14% before to 5% after using the thorough search [7]. The etiologies that became increasing markedly after a systematic search were gallstone (from 22% to 37%) and miscellaneous causes (from 11% to 17%) [7].
Currently, there are only few guidelines that specifically address how to search the etiologies of AP [1,2]. Based on these guideline [1,2] and more recent reviews[3,6,24,26]. The author proposes an 8-step search (Figure 1) as follows [7].
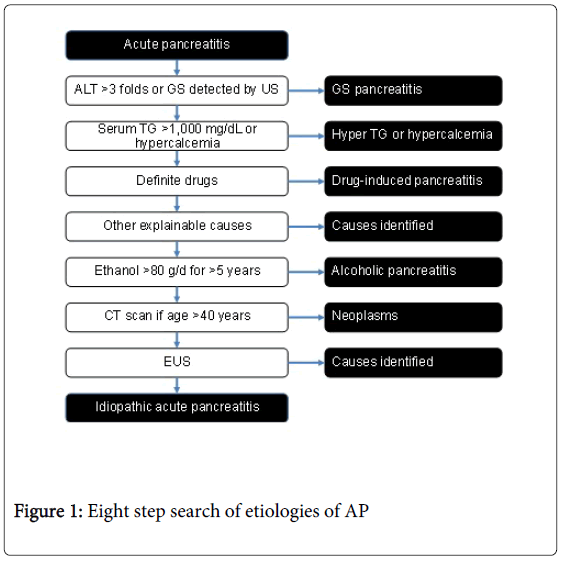
Figure 1: Eight step search of etiologies of AP
1. Check liver biochemistry test and perform transabdominal US to rule out gallstone pancreatitis in all patients [1-3,12-14].
2. Check serum triglyceride in all patients at admission and before discharge [3,24].
3. Check serum calcium in all patients at admission and before discharge [3,24].
4. Review definite drugs that can cause AP.
5. Review other explainable causes of AP e.g. post-ERCP, post-FNA, post balloon-assisted enteroscopy, vasculitis, infections and trauma.
6. Review history, amount and duration of alcohol consumption. If the amount is >80 g per day for >5 years, then it may assume alcohol as the cause of AP.
7. If patient is >40 years of age, perform cross-sectional imaging to rule-out neoplasms [32].
8. Perform EUS to rule out small stones, small ampullary and pancreatic neoplasms and early chronic pancreatitis [45,47].
9. If no cause is identified, then the patient can be labeled as “idiopathic” AP.