Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2018) Volume 8, Issue 8
Keywords: Knowledge; Practice; Emergency contraceptive
Background
Worldwide young women and men suffer a disproportionate share of unplanned pregnancies, sexual transmitted disease STD including HIV and other serious reproductive health problems. To alleviate this problem, increasing accessibility and awareness of contraception methods including emergency contraception’s to these vulnerable young population is a critical step to be implemented.
Emergency contraceptives is a type of modern contraception which is indicated after unprotected sexual intercourse, following sexual abuse, misuse of regular contraception or non-use of contraception [1].
EC plays a vital role in preventing unintended pregnancy, which in turn helps to reduce unintended child birth and unsafe abortion, which are major problems of maternal health [1]. EC is found to be effective if used as soon as possible after unprotected sexual intercourse, especially within 72 hours of unprotected sexual intercourse [2]. There are two types of ECs namely, emergency contraceptive pills and intrauterine devices (IUDs).
The pills include combined oral contraceptive pills (COCs) and a progestin only pills (POPs); IUDs can be effective if it is inserted within 5 days of unprotected sexual intercourse [3]. EC is said to be safe with minor side effects like nausea and vomiting in case of pills and infection for IUDs if not used properly [3].
Effectiveness of EC said to be 75% in case of COCs and 85% in case of POPs [4]. Regarding the mechanism of action, EC works by preventing fertilization, implantation and tubal transportation of sperm and ovum [5].
Most adolescent pregnancies seem to be intended; just because they happen within marriage but in reality most of them are unintended rather the marriage itself is arranged by the girls’ family due to some cultural influences [6-8]. Adolescent pregnancy affect the health of mother and child, it has a devastating impact in social and psychological life of the girls [8].
Considering the importance of EC in preventing unintended pregnancy, this study aimed to assess the knowledge and practice of EC and to further elucidate the relationship between these factors and socio economic and demographic characteristics. Among female students of Ayder Preparatory School [9-15]
Statement of the problem
Unsafe abortion is a major public health problem in low-andmiddle income countries. Young and unmarried women constitute a high risk group for unsafe abortions. The World Health Organization estimates that 84 million unwanted pregnancies occur annually worldwide. On average, 46 million abortions take place every year, out of which 20 million (43.8%) are performed under unsafe conditions. Seventy thousand women die yearly as a consequence of unsafe abortion, while five million suffer permanent or temporary disability [16-18]. Approximately 13% of pregnancy-related mortality worldwide is due to unsafe abortions and the majority of these deaths (and morbidities) occur in low-and-middle income countries. An important proportion of maternal deaths worldwide are attributable to induced unsafe abortion.
There is unexpected discrepancy between modern contraceptive services and high levels of unwanted pregnancy and unsafe abortion on the other. According to the study by World Health Organization (WHO) the reason for this is societal change caused by rapid industrialization and urbanization lead to loosening of family ties and erosion of traditional sanctions that inhibited premarital sexual activity [19-23]. Younger age of menarche, combined with delayed age of marriage, and adolescents are increasingly forced to learn and exercise sexual activities from their peers and mass media. Maternal mortality in Ethiopia is one of the highest in the world which is 673/100,000 live births. Unwanted pregnancy is a big problem in Ethiopia; more than 60% of pregnancies in adolescents are unwanted and most of them ends up as unsafe abortion.
According to MoH abortion account for nearly 60% of Gynecological and almost 30% of all Obstetric & Gynecological admissions. A community based survey in Addis Ababa Showed that 54% of maternal deaths resulted from unsafe abortion [18].
Significance of study
The study is designed to investigate the prevailing Knowledge and Practice of ECPs and related gaps among female students in Ayder preparatory school. From the finding of this research one can learn the status of Knowledge and practice of students towards using ECPs. Related gaps were also identified. And the finding of this research can also show us the real picture ECPs utilization by preparatory school girls. Government and Non-Governmental organization’s working in this area will get important information that will help them to address the gaps. Similar studies could also be promoted by using the finding of this research.
This study will provide valuable information to the health professionals, researchers, regional health bureau and other stakeholders. By using this study the above professional will plan their resource for intervention.
General objective
• To assess the Knowledge and Practice of Emergency contraceptive among female students of Ayder preparatory school
Specific objectives
• To identify the knowledge of emergency contraception among female students of Ayder preparatory school
• To identify the practice of emergency contraception among female students of Ayderpreparatory school
Study area and period
The study was conducted from December 15 to February 03/ 2009 E.C in Ayder preparatory school, which is located in Mekelle city, the capital city of Tigray, in Northern Ethiopia, at a distance of 783 kilometers from the Ethiopian capital city, Addis Ababa [12].
Study design
The study used quantitative method which is institutional based cross-sectional study was conducted for data collection from 520 Ayder preparatory school female students during the month of December to February 2009.
Population
Source population: All female students whose age is 15 and above in Ayder preparatory schools.
Study population: A sample of female students drawn from Ayder preparatory schools.
Study subjects: who were present and attend the class during data collection.
Inclusion and exclusion criteria
Inclusion Criteria: All female students aged 15 & above attending class, who were present and consented during study period.
Exclusion Criteria: Regular students suspended from the school by breaking rules and regulations absent from class by any means, extension students, not consented and disabled.
Sample size calculation
The following assumption was considered to calculate the sample size. Since there is specific study done that is similar to this one, we have used 75% as a proportion of students having awareness of emergency contraception in Ambo preparatory school. So as to minimize variability the sampling procedure will comprise two sampling techniques: SRS and systemic sampling. The determined sample size was 276 and to compute non-response rate 10% of the sample size will be added; this gives a total of 304.
Sampling procedure
Multistage sampling technique was used to select study subjects from the entire student currently in Ayder preparatory school. Ayder preparatory school was purposefully selected followed by registration of all female students based on the inclusion criteria. Required number of total sample size was proportionally allocated among all female students of preparatory schools based on the different grades as well as by the number of the students through allocation formula. Finally respondents from each grade were selected by random sampling method (Figure 1).
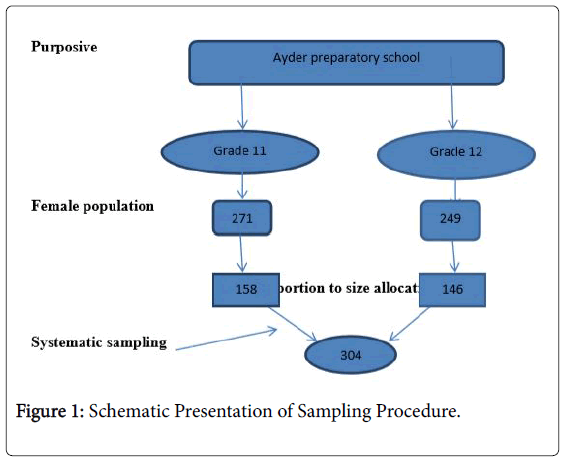
Figure 1: Schematic Presentation of Sampling Procedure.
Data collection instruments
Data was collected using self- administered Questionnaire which was prepared in English to assess socioeconomic status, reproductive characteristics as well as their knowledge and practice towards EC.
Study variables
Dependent variables:
• Knowledge towards emergency contraceptive
• Practices towards emergency contraception
Independent variables:
• Age (in years): different age groups
• Ethnicity: Amhara, Oromo, Tigre, and others (Somalia, Affar)
• Region: Addis Ababa, Oromo, Amhara, Tigray, Affar
• Marital status: Unmarried, married, divorced and widowed
• Parent seducational status: Can't write and read, can write and read, primary school (1-8th), secondary school (9-12th) and Higher education
Data quality control
Different methods were used to assure data quality such as questionnaire will be checked for its completeness, clear instruction was given for data collectors.
Data processing and analysis
After data collection is completed, the data was entered into SPSS software version [23]. It was then be checked for its completeness and analyzed. Results was presented using different forms of analysis like descriptive statistics, Table of frequency and pie chart were present the result. Multivariate analysis was done to see the relative effects of the predictors on dependent variables (Tables 1 and 2).
| Characteristics | Number | Remark |
|---|---|---|
| Age (years) | N=304 | |
| 15-18 | 173 | 58.6% |
| 18-21 | 122 | 41.6% |
| Religion | N=304 | |
| Orthodox | 244 | 82.7% |
| Muslim | 27 | 9.2% |
| Others (…………) | 24 | 8.2% |
| Educational level | N=295 | |
| Grade 11 | 150 | 50.8% |
| Grade 12 | 145 | 49.2% |
| Marital status | ||
| Single | 290 | 98.3% |
| Married | 4 | 1.7% |
Table 1: Socio-demographic and academic Characteristics among female students in Ayder preparatory school Mekelle town; February 2009 EC.
| Characteristics | Number | Remark |
|---|---|---|
| Ever Heard(know) Emergency | N=295 | |
| Contraceptive | ||
| Yes | 188 | 63.7% |
| No | 103 | 36.3% |
| Know Emergency Contraceptive Used after Unprotected Sexual intercourse | n=295 | |
| Yes | 152 | 51.5% |
| No | 143 | 48.5% |
| Method Reported as Emergency Contraceptive (Multiple response) | n=295 | |
| OCP | 105 | 40.1% |
| IUCD | 64 | 24.4% |
| Others | 95 | 35.7% |
| n= 295 | ||
| Sources of EC Supply Multiple Response | ||
| Health Institution | 144 | 42.2% |
| Pharmacy | 85 | 31.5% |
| Private clinic | 51 | 18.9% |
| Others | 20 | 7.5% |
| EC pill taken within 72 hours | n=295 | |
| Yes | 67 | 22% |
| No | 117 | 39.7% |
| No response | 11 | 3.7% |
| Don’t know | 100 | 33.9% |
| Your sources of information | n= 295 | |
| Multiple responses | ||
| Mass media | 103 | 35.6% |
| Friends | 49 | 17% |
| School clubs | 94 | 32.5% |
| Others | 43 | 14.9% |
| Ever had sex | n=295 | |
| Yes | 155 | 54.4% |
| No | 130 | 45.6% |
| Age ate first sex | ||
| 15-17 | 35 | 21.1% |
| 17-19 | 83 | 50% |
| 19+ | 48 | 28.9% |
| Ever used EC | ||
| Yes | 83 | 28.1% |
| No | 191 | 64.7% |
| No response | 21 | 7.1% |
| Types of contraceptive used | n=295 | |
| Multiple responses | ||
| Pills | 76 | 86.4% |
| IUCD | 2 | 2.3% |
| Others | 10 | 3.4% |
| Reasons for not using EC Multiple responses | n=295 | |
| Health worker unwilling | 10 | 5.4% |
| Drug unavailable | 23 | 12.4% |
| Time | 27 | 14.5% |
| Inconvenient | 17 | 9.1% |
| Privacy is not kept | 35 | 18.8% |
| Others | 81 | 43.5% |
Table 2: Knowledge and Practice of contraception among female students of Ayder preparatory school Mekelle city, February 2009 EC.
Ethical permission for the study was obtained from Mekelle university ethical board commute and the ethical board of Ayder preparatory school. Written letter from Mekelle university midwifery department was obtained. Informed consent from each participant was obtained. No form of identifiers was included in the questionnaires to maintain confidentiality. Participant was informed that they could withdraw from the study at any stage if they desire, without any penalty.
Final document of the result was given to department of midwifery, Mekelle University, collage of health science, library and Ayder preparatory school.
Socio demographic characteristics in our study the response rate was 97%. Among 304 study participants 173(58.6%) participants were 15-18 and 122 (41.4%) were 18-21 years age. When we see the study participants’ religion, about 244 (827%) were orthodox, 27(9.2) were Muslim in religion and 8.2% were other religion follower and 290(98.3%) are single. The predominant ethnic group was 281 (95.3) Tigray the rest was Amara, Oromo and other. Their family occupations were 26.8%gevernmental employers, 25.8% merchant, 10.5% were private employer and 37%were other works.
Knowledge of study participants
In this study it has been found that out of the study participants 188(63.7%) was heard and 103(36.3%) are not heard (not know) about emergency contraceptive. Of those heard emergency contraceptive, 103(35.6%) mass media, school club 94 (32.5%) Friends 49(17%) and others 43(14.9%) are sources of information for their knowledge about Emergency contraceptive and152 (51.5%) know about emergency contraception taken after unprotected sexual intercourse. 105 (35.6%) of them reported that they know post pills (OCPs) and of this 77(26.1%) reported that they know two types of emergency contraceptive, whereas 64(21.7%) know intrauterine device. Of those respondents who have heard about EC, 144(42.2%) identified places to get EC as health institution, 85(31.5%) pharmacy and 51(18.9 %) private clinic and 21(7.5%) from other source. 67 (22.7%) of those ever heard about EC knows that OCPs could be used within 72 hours (3days) after unprotected sexual intercourse.
Emergency contraceptive practice of respondents
Among 304 sampled students 155(54.4%)practices sex out of which35(21.5%)practice sex ate age of 15-17,83(50%) ate age of [17-19]and 48(28.9%)are ate age 19 and above.
About 83(28.1%) of the respondent Used EC and 191 (64.7%) doesn’t used EC and 21(7.1%) are none response. Of those who have used EC .76(86.4%) have used pills and 2(2.3%) IUCD are the method they are used as emergency contraceptive and 10(3.4%) Others method they are used as emergency contraceptive. Of those who are not used emergency contraceptive are 35(18.8) due to lack of privacy, time 27(14.5%) inappropriateness, drug unavailability 23(12.4%) and others reasons 81(43.5%).
This study has tried to assess knowledge and practices of contraception with special Emphasis to EC among female students in Ayder Preparatoryschool’ Mekelle city, Tigray, North Ethiopia Family planning is defined by WHO as a way of thinking and living that is adopted voluntarily, upon the basis of knowledge, attitudes and responsible decisions by individuals and couples, in order to promote the health and welfare of family groups and thus contribute effectively to the social development of a country.
Although emergency contraception is not recommended as a regular family planning method it is a useful method after unprotected sexual intercourse to reduce the chance of unwanted pregnancies. Emergency contraception is most useful when there is a failure of barrier methods. Such as slippage and breakage of condoms, or when sexual intercourse was unpremeditated. The result of this study showed that 63.7% of the respondents had known about EC. The major source of their knowledge as revealed in the study was media, school club and their friends. This result is lower than the study done on atse yohannes preparatory school in Mekelle (90.7%) [19]. This finding was higher than reports of students from other urban centers of the country where contraceptive knowledge level varies from 54% in Harar (20) and 53-62% in northern Gonder [21].
Besides, the figure in this study is lower than when compared to similar studies done among university students in Addis Ababa University (84.2%) [22] and Bahir Dar University 83.5% [23]. This magnitude was also less than adolescents’ contraceptive knowledge in Asia, North Africa, the Caribbean and Latin America, where the level of adolescents’ knowledge on contraception was above 90% [24]. This might be due to the better information exposure and communication that school adolescents now have and influence of mass media. Perhaps, it could be due to the fact that the most widely available method of family planning is oral contraceptive pills, the most familiar method obtained in this paper was oral contraceptive pill, which was congruent with other studies [21]. About 63.7% of study subjects had heard about emergency contraception. A study conducted in Nigeria and Addis Ababa University showed that 58 and 43.3% [22] knew about emergency contraception, respectively.
The result of this study was lower; the difference could be due to the difference in the population studied and time interval between the studies. Contraceptive use in this study was 28.1%. A research done in North Gondar showed that contraceptive use was 30.7% [21], while a study done in Harar was 20% [20].
The possible reason for this difference could be variation in the population studied. The major source of information on contraception in this study was mass media (35.6%) while it was 23.8% in a study done in North Gondar [21]. This difference might be due to increasing number of televisions per household with increasing emphasis by the government through different attractive announcements and programs on television. In this study, it was observed that health institution was the main source of contraceptive method accounting for 42.2%. A study done in Jimma Seto Semero high school showed 98.96% from clinic and pharmacy [24]. Among those who did not use any method of contraceptive in this study, 18.8% were not using for privacy are not kept, and 14.5% for time reason and 12.5% because off drug unavailability. A study done in north Gondar showed that majority of non-users did not use because of privacy or time reason [21]. This could be the difference in the population studied and changes in the study period.
This study showed that most of the students had knowledge of contraception. Predominant Methods known by students were oral contraceptive pills, intrauterine device respectively. And also the number one method used by students was oral contraceptive pills.
Even among those who were aware, the detail knowledge and practice of EC was very low. There is a need to educate adolescents about emergency contraceptives, with emphasis on available methods and correct timing of use.
Older adolescents (age 17-19 years) ever used contraceptive methods than younger ones.
Mass media and school clubs were found to be the most important source of information for promoting utilization of contraceptives.
Among the non-users, the majority of respondents did not use for lack of privacy and time.
Information education and communication activities regarding utilization of modern contraceptive methods among adolescents and their importance should be strengthened by the Ministry of health through mass media messages and encouraging school health programs.
To improve reproductive health outcomes; Policy makers must ensure that the school curricula provide an overriding role in developing the knowledge e and proper practice of Contraceptives in general and emergency contraceptive pills in particular.
Information education and communication activities regarding utilization of modern contraceptive methods among adolescents and their importance should be strengthened by the Ministry of health through mass media messages and encouraging school health programs.
School community and parents of students should discuss about the students’ academic and other issues like reproductive health needs of youth.
School management and stakeholders should take responsibility of organizing youth and other reproductive health clubs at school.
In addition, broader Media coverage like TV, Radio, Bulletin, Magazines, and Newspapers can be well organized and consistently used in such a way that it can develop awareness on reproductive health related Matters. Regular monitoring and evaluation of the available services are also decisive for enhancement actions to be undertaken.
Promoting similar research work can also play a great role in addressing the issues of Reproductive Health.