Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2016) Volume 5, Issue 1
Background: Positron emission tomography/computed tomography is suggested to have a role in detection of iodine negative recurrence in well differentiated thyroid cancer. The aim of this study is to identify role of different imaging modalities in the management of well differentiated thyroid cancer.
Methods: We reviewed 900 well differentiated thyroid cancer patients after post-thyroidectomy who underwent recombinant human thyroid stimulating hormone stimulated Sodium Iodide I 131 imaging. Out of 900 patients, 74 had positron emission tomography/computed tomography. Multivariate analysis was performed by controlling positron emission tomography/computed tomography, Sodium Iodide I 131 scan, neck ultrasonography, age, sex, primary tumor size, stage, histology, thyroglobulin. Patients were grouped according to results of Sodium Iodide I 131 scan and positron emission tomography/computed tomography.
Results: Positron emission tomography/computed tomography was positive in 23 of 74 patients. The sensitivity for positron emission tomography was 11/11(100%), the specificity was 51/63 (81.0%), the positive predictive value was 11/23 (47.8%), and the negative predictive value was 51/51 (100%). The sensitivity for the neck ultrasonography was 4/8 (50%), the specificity was 53/60 (88.3%), positive predictive value was 4/11 (36.4%), and negative predictive value was 53/57 (93.0%). 50% of patients who had Sodium Iodide I 131 negative scan and positive positron emission tomography/computed tomography had a change in management. Thirty-six percent with positive neck ultrasonography had a change in management. Out of 11 recurrences, 6 had distant metastatic disease, and 5/11 had regional nodal disease. Neck ultrasonography showed nodal metastasis in 4/5 (80%).
Conclusion: Positron emission tomography/computed tomography altered management in the presence of a high thyroglobulin level and a negative Sodium Iodide I 131 scan. Neck ultrasonography should be the first line of imaging with rising thyroglobulin levels. Positron emission tomography/computed tomography should be considered for cases with high thyroglobulin levels and normal neck ultrasonography to look for distant metastatic disease.
Keywords: Positron emission tomography; Well differentiated thyroid cancer; Neck ultrasound; Thyroglobulin
Thyroid cancer is the most common malignancy of the endocrine system [1-3]. Well differentiated thyroid cancer (WDTC) is the most common of all histologic subtypes of thyroid cancer, accounting about 80-85% of all thyroid malignancies [4]. Unlike more aggressive subtypes like anaplastic and medullary thyroid carcinomas, WDTC generally has a favorable prognosis. However 20-30% of WDTC recurs, and 7% of patients with recurrent disease will die within 10 years of initial diagnosis [1,4,5].
Following initial treatment with total thyroidectomy and radioactive iodine therapy (RIT), serum thyroglobulin (Tg) level becomes a reliable marker for persistent or recurring disease in the absence of anti-thyroglobulin antibodies [1,4]. In the case of a rising Tg level with a negative neck ultrasound, clinicians often consider cross sectional imaging [6]. Although radioactive iodine imaging is efficient in most of WDTC follow up, between 10-30% of NaI-131 scans are negative in patients with recurrent WDTC and increased Tg levels [4,7-10]. Localization of recurrence is essential as surgery is the most effective curative option [4]. Hence, for patients with negative radioactive iodine imaging (NRI), negative neck ultrasounds and increased Tg levels, alternative imaging modalities are considered [4].
Feine et al. [11,12] demonstrated that 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/ CT) can detect tumor lesions that are missed by NaI-131 scintigraphy. The mechanism behind this is explained by a “flip flop phenomenon”, where WDTC have iodine uptake due to presence of active Na-I symporters (NIS) but no glucose uptake, whereas dedifferentiated tumors cease expression of NIS with upregulation of glucose metabolism [1,13,14].
A meta-analysis by Leboulleux et al. [15] showed that sensitivity and specificity of FDG-PET for detection of recurrent WDTC ranges from 45 to 100% and 42 to 90%, respectively. Dong et al. [16] reviewed 25 studies and concluded that FDG PET/CT has a sensitivity of 93.5% for detecting recurrent WDTC in the absence of radioiodine uptake. Recently Haslerud et al. [1] reviewed 34 publications in a meta-analysis study and showed that FDG PET/CT has pooled sensitivity of 79.4% and specificity of 79.4% to detect recurrent WDTC. Bertagna et al. [17] reviewed the literature on the correlation of PET/CT and thyroglobulin levels and concluded that a cut off value of 10 ng/ml is reasonable, with high accuracy. Bannas et al. [18] also showed that FDG PET/CT enabled localization of locoregional and distant metastasis in patients with a NRI and rising Tg levels
Currently, there is no consensus for the use of FDG PET/CT in WDTC. Recently updated American Thyroid Association (ATA) guidelines strongly recommend the use of FDG-PET/CT in high risk WDTC patients (patients with gross extra-thyroidal tumor extension, incomplete resection at surgery or patients with known metastatic disease) with elevated serum Tg levels (generally more than 10 ng/dl) with a NRI [19]. ATA also suggests FDG PET/CT as part of the initial staging of poorly differentiated thyroid cancer and invasive Hürthle cell carcinomas, especially with evidence of disease by other imaging modalities or with increased serum Tg levels [19].
Subramaniam et al. [4] had a literature review and reported that FDG PET/CT changed management of WDTC in 14 to 78% of patients. Most of these patients had NRI and high Tg levels [4]. A recent publication by Wiebel et al. [5] also showed that PET scan results changed management in 30% of cases.
Our aim is to identify the role of neck ultrasound, NaI-131, FDG PET/CT imaging, serum Tg levels as well as other parameters including sex, age, and histologic subtype in the clinical management of WDTC.
Patients
After we obtained institutional review board approval for this retrospective study, we performed a review of the database of the Department of Radiology to identify post-thyroidectomy patients with WDTC who had undergone recombinant human TSH (rhTSH) stimulated NaI-131 scans between 2001 and 2014. Nine hundred patients were identified. Out of 900 patients, 74 had a FDG PET/CT performed at the same session. Serum Tg levels were obtained before and after rhTSH injections. Tg antibody levels at the time of imaging was also obtained if available. Neck ultrasounds if available were also evaluated.
Measures
Patient demographics including age, sex and clinical/pathologic characteristics such as histology, vascular invasion, extrathyroidal extension, lymph node metastasis, and tumor size were obtained when available (Table 1).
| Variable | Level | N = 74 | % |
|---|---|---|---|
| Sex | F | 46 | 62.2 |
| M | 28 | 37.8 | |
| Aggressive histology | Negative | 38 | 77.6 |
| Positive | 11 | 22.4 | |
| Missing | 25 | - | |
| Vascular invasion | Negative | 32 | 60.4 |
| Positive | 21 | 39.6 | |
| Missing | 21 | - | |
| Extrathyroidal extension | Negative | 28 | 59.6 |
| Positive | 19 | 40.4 | |
| Missing | 27 | - | |
| Lymph node metastasis | Negative | 12 | 18.5 |
| Positive | 53 | 81.5 | |
| Missing | 9 | - | |
| Multicentricity | Negative | 22 | 32.8 |
| Positive | 45 | 67.2 | |
| Missing | 7 | - | |
| Age | Mean | 54.27 | - |
| Median | 55 | - | |
| Minimum | 22 | - | |
| Maximum | 93 | - | |
| StdDev | 15.67 | - | |
| Missing | 0 | - | |
| Tumor size (cm) | Mean | 2.78 | - |
| Median | 2.2 | - | |
| Minimum | 0.4 | - | |
| Maximum | 13 | - | |
| StdDev | 2.31 | - | |
| Missing | 21 | - |
Table 1: Demographics.
rhTSH
All patients had intramuscular injections of rhTSH on day 1 and day 2. On day 3, all patients had oral administration of 4 mCi NaI-131.
FDG-PET/CT protocol
All PET/CT studies were performed using one of 4 PET/CT systems (GE Discovery 690 Elite, 600, ST, or LS; General Electric, Milwaukee, Wisc.). Patients fasted at least 4 hours before the scan, and were imaged approximately 60 minutes after radiotracer injection. Patients were instructed not to talk during incubation period. Scans were obtained from skull base to mid thigh. All PET data was reconstructed with and without CT-based attenuation correction. The emission scan lasted for 2-4 minutes for each bed position.
NaI-131 scan protocol
48 hours after administration of 4 mCi NaI-131, whole body NaI-131 scans were obtained by using a large dual field of view dual head gamma camera. (Infinia, GE Healthcare or Symbia, Siemens Healthcare). Anterior and posterior whole body images were acquired, with additional spot images of the neck as well as foci with abnormal NaI-131 uptake.
Neck ultrasonography
A Board certified nuclear radiologist (ATK) who also completed a Neuroradiology fellowship with 5 years of expertise in neck USG re-evaluated the available USG images. The thyroid bed and cervical nodal regions were evaluated for findings suspicious for local/regional recurrence.
Image analysis
Board certified nuclear medicine physicians or nuclear radiologists interpreted the NaI-131 scans and PET/CT images at the time of clinical reading. The clinical reports were retrospectively reviewed by a nuclear radiologist (ATK). A study was considered positive if there was a clear statement of recurrence. A study was considered negative when there was a statement clearly mentioning no evidence of disease. Indeterminate studies reevaluated by the nuclear radiologist and included in either positive or negative scan results.
Post imaging management plan analysis
PET/CT and neck USG were accepted as changing management if one of these criteria was present:
1. If PET/CT and/or neck USG found surgically removable disease that was not identified on NaI-131 WBS.
2. If PET/CT and/or neck USG found localized disease that was not seen on NaI-131 WBS that could be irradiated.
3. If PET/CT identified disseminated disease amenable to systemic therapy.
Statistical analysis
The primary endpoint was change in management, and the proportion of those with a change in management was compared across each variable of interest, including serum Tg, PET/CT imaging, NaI-131 scan, neck USG, as well as demographic factors such as sex and age, and clinical characteristics such as histology, vascular invasion, extrathyroidal extension, lymph node metastasis, and tumor size.
For serum Tg (both prior to the rhTSH injections and at the time of PET), the median value was used to create a high/low cut point. For Serum Tg antibody, patients were categorized as positive or negative. For PET/CT imaging, patients were categorized as positive or negative, and for NaI-131/PET status, patients were categorized as NaI-131(+) PET(+), NaI-131(+)PET(-), NaI-131(-)PET(+), and NaI-131(-)PET(- ). Neck USG was categorized as either positive for local/regional recurrence or negative. Categorical variables were compared across change in management groups using chi-squared tests or Fisher’s Exact tests, where appropriate, and numeric variables, such as age and tumor size, were compared across change in management groups using ANOVA. PET-specific sensitivity was estimated, where sensitivity was defined as the proportion of those with a change in management who were PET positive. Neck USG-specific sensitivity also was estimated, where sensitivity was defined as the proportion of those with a change in management who were neck USG positive. Additionally, specificity, positive predicted value (PPV), and negative predicted value (NPV) were estimated for both PET and neck USG. Significance was assessed at the 0.05 level, and the analysis was performed using SAS 9.3.
Twenty-eight patients were male (37.8%), and 46 were female (62.2%). The mean age was 54 years, and the mean tumor size was 2.8 cm. Eleven (14.9%) patients had a change in management. Eleven (22.4%) had an aggressive histology, 21 (39.6%) had vascular invasion, and 53 (81.5%) had lymph node metastasis. Twenty-three (31.1%) patients had a positive PET scan. Of the 23 PET positive patients, 22 were NaI-131 negative, and 1 was NaI-131 positive. Of the 51 PET negative patients, 48 were NaI-131 negative, and 3 were NaI-131 positive. Of the 68 patients who also had ultrasounds, 11 (16.2%) had a positive neck USG, 57 (83.8%) had a negative neck USG (Table 1).
Tg antibodies were measured in 26/74 of patients. Of the 26 patients, 4 had positive Tg antibodies. Tg Ab measurements from three different time points (before ablation, before PET/CT and same time with PET/CT) showed that 2 of these patients had a trend of decrease in Tg Ab levels, whereas 2/4 showed an increase in Tg Ab levels. Of the 4 Tg Ab positive cases, only one had a positive neck USG. Biopsy of the suspicious focus was non malignant. All of the four cases had NaI-131(-) PET (-).
Overall, only serum Tg (prior to PET), PET/CT, serum Tg (same time with PET/CT), NaI-131(-) PET(+) status, neck USG, and age were associated with change in management (Table 2). For example, 50% of the patients in the NaI-131(-) PET (+) group had a change in management, while 0% of the remaining groups had a change in management (p < 0.001). Those with a high Tg value, either prior to PET or at the same time with PET, experienced a higher proportion of change in management (p < 0.05). 48% of the PET positive patients had a change in management compared to 0% of the PET negative patients (p < 0.001). Thirty-six percent of the patients with a positive neck USG had a change in management compared to 7% of patients with a negative ultrasound (Table 2).
| Covariate | Statistics | Level | No N=63 | Yes N=11 | P-value* |
|---|---|---|---|---|---|
| Sex | N (Row %) | F | 39 (84.78) | 7 (15.22) | 1 |
| N (Row %) | M | 24 (85.71) | 4 (14.29) | ||
| Aggressive histology | N (Row %) | Negative | 34 (89.47) | 4 (10.53) | 0.605 |
| N (Row %) | Positive | 9 (81.82) | 2 (18.18) | ||
| Vascular invasion | N (Row %) | Negative | 28 (87.5) | 4 (12.5) | 1 |
| N (Row %) | Positive | 18 (85.71) | 3 (14.29) | ||
| Extrathyroidal extension | N (Row %) | Negative | 22 (78.57) | 6 (21.43) | 0.215 |
| N (Row %) | Positive | 18 (94.74) | 1 (5.26) | ||
| Lymph node metastasis | N (Row %) | Negative | 11 (91.67) | 1 (8.33) | 1 |
| N (Row %) | Positive | 45 (84.91) | 8 (15.09) | ||
| Multicentricity | N (Row %) | Negative | 18 (81.82) | 4 (18.18) | 0.461 |
| N (Row %) | Positive | 40 (88.89) | 5 (11.11) | ||
| Initial whole body scan findings | N (Row %) | Negative | 50 (84.75) | 9 (15.25) | 1 |
| N (Row %) | Positive | 12 (85.71) | 2 (14.29) | ||
| TG (prior to PET) | N (Row %) | Low | 31 (93.94) | 2 (6.06) | 0.044 |
| N (Row %) | High | 24 (75) | 8 (25) | ||
| TG Ab (prior to PET) | N (Row %) | Negative | 16 (100) | 0 (0) | <.001 |
| N (Row %) | Positive | 4 (40) | 6 (60) | ||
| PET | N (Row %) | Negative | 51 (100) | 0 (0) | <.001 |
| N (Row %) | Positive | 12 (52.17) | 11 (47.83) | ||
| Tg (same time with PET) | N (Row %) | Low | 30 (93.75) | 2 (6.25) | 0.036 |
| N (Row %) | High | 27 (75) | 9 (25) | ||
| TG Ab (same time with PET) | N (Row %) | Negative | 22 (100) | 0 (0) | N/A |
| N (Row %) | Positive | 4 (100) | 0 (0) | ||
| I131 PET | N (Row %) | I131(+) PET(+) | 1 (100) | 0 (0) | <.001 |
| N (Row %) | I131(+) PET(-) | 3 (100) | 0 (0) | ||
| N (Row %) | I131(-) PET(+) | 11 (50) | 11 (50) | ||
| N (Row %) | I131(-) PET(-) | 48 (100) | 0 (0) | ||
| Ultrasound | N (Row %) | Negative | 53 (92.98) | 4 (7.02) | 0.02 |
| N (Row %) | Positive | 7 (63.64) | 4 (36.36) | ||
| Age | N | 63 | 11 | 0.038 | |
| Mean | | 52.7 | 63.27 | ||
| Median | 52 | 64 | |||
| Tumor size (cm) | N | 47 | 6 | 0.33 | |
| Mean | 2.66 | 3.65 | |||
| Median | 2.2 | 2.6 | |||
| *Thep-valueiscalculatedbyANOVAfornumericalcovariates;andchi-square testorFisher'sexactforcategoricalcovariates,whereappropriate | |||||
Table 2: Change in management.
The sensitivity for PET was 11/11 or 100%, the specificity was 51/63 (81.0%), the PPV was 11/23 (47.8%), and the NPV was 51/51 (100%). The sensitivity for the neck USG was 4/8 (50%), the specificity was 53/60 (88.3%), the PPV was 4/11 (36.4%), and the NPV was 53/57 (93.0%).
Eleven patients had a change in management. Six of these patients had distant metastatic disease, and 5/11 had regional nodal metastatic disease. Neck USG was able to identify neck nodal metastasis in 4/5 (80%) of these cases.
The objective of this study was to identify the clinical, imaging, histologic, and laboratory parameters that affect clinical management of WDTC. Our results showed that patient age, serum Tg levels, positive PET/CT in the presence of a negative NaI-131 scan, and neck USG have a role in change in clinical management. Other parameters, including Tg antibody, tumor size, extra thyroidal extent, stage, histologic subtype, sex had no significant role. There was change in clinical management of 50% of patients who had a positive PET/CT with a negative NaI-131 scan (Figure 1). Thirty-six percent of the patients with a positive neck USG had a change in management compared to 7% of patients with a negative ultrasound.
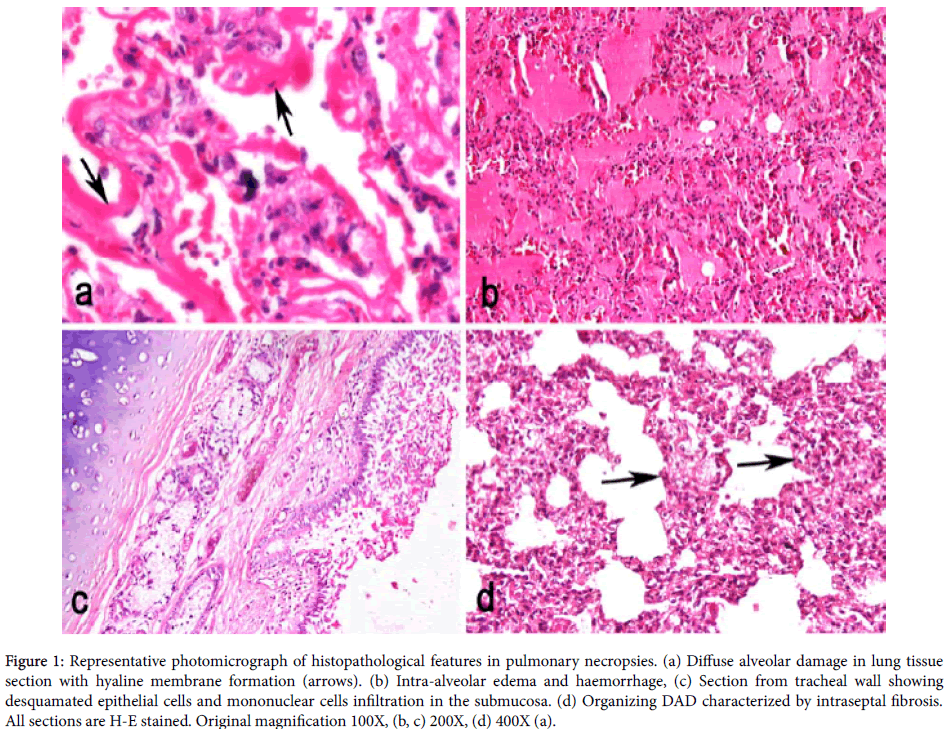
Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies. (a) Diffuse alveolar damage in lung tissue section with hyaline membrane formation (arrows). (b) Intra-alveolar edema and haemorrhage, (c) Section from tracheal wall showing desquamated epithelial cells and mononuclear cells infiltration in the submucosa. (d) Organizing DAD characterized by intraseptal fibrosis. All sections are H-E stained. Original magnification 100X, (b, c) 200X, (d) 400X (a).
Although there are several publications supporting the use of FDG PET/CT in patients with high Tg levels and NRI, there is no clear guidance of when to order PET/CT scans [5]. The ATA guidelines suggest obtaining PET/CT in high risk WDTC patients with elevated Tg levels (generally Tg more than 10 ng/dl) with NRI [19]. However, there are other studies showing PET/CT scans can still be useful in patients with low Tg levels below 10 ng/dl, which may reflect production of mutant Tg not detectable by conventional assays or loss of Tg synthesis altogether [20]. Recently, use of serum Tg velocity and Tg doubling time have been shown to be good predictors of outcome, distant metastases, and loco-regional recurrence [20]. Wiebel et al. [5] also showed a correlation between increased stimulated Tg levels and PET positivity. However, like in our study, there was no Tg level that predicted the presence or absence of disease.
FDG PET/CT is a powerful imaging modality, but it is not without limitations. False negative results may occur due to small tumor volume, especially with the neck lymph nodes. These could be better detected by ultrasound [21]. False negative scans can also result from recurrence near structures with inherently high physiologic background FDG activity such as lingual tonsils and soft palate [20]. Inflammatory lymph nodes, suture granulomas, and other benign entities can cause false positive results [20] (Figure 2).
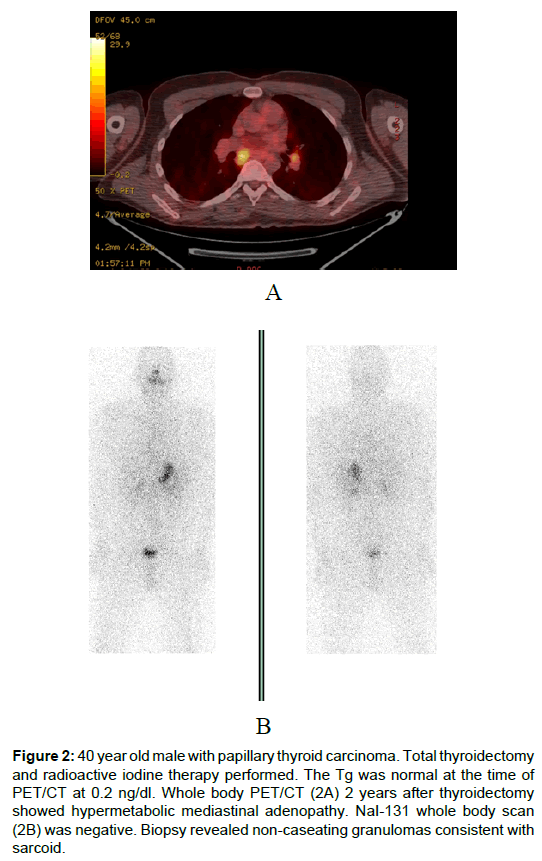
Figure 2: 40 year old male with papillary thyroid carcinoma. Total thyroidectomy and radioactive iodine therapy performed. The Tg was normal at the time of PET/CT at 0.2 ng/dl. Whole body PET/CT (2A) 2 years after thyroidectomy showed hypermetabolic mediastinal adenopathy. NaI-131 whole body scan (2B) was negative. Biopsy revealed non-caseating granulomas consistent with sarcoid.
During decision making, clinicians should also consider the risk of radiation exposure and high cost of PET/CT [5,22,23]. As most of the recurrences are in the neck, initial assessment with a neck USG would offer the advantages of absence of radiation and lower cost [5]. Following surgery, neck USG is recommended at 6-12 months and periodically depending on patient’s risk for recurrence and Tg levels [19]. If a positive result would change management, the ATA suggests biopsy of the cervical lymph nodes larger than 8-10 mm [19]. Our study also showed that neck USG was able to identify most of the (80%) neck nodal metastasis (Figure 3). There was only one case where neck USG was not able to identify malignant nodal disease. Kim et al. [24] showed that administration of empiric RAI therapy to patients with negative NaI-131 and negative FDG PET/CT was not useful both therapeutically and diagnostically. Hence, proper use of FDG PET/ CT may reduce number of unnecessary high dose NaI-131 therapies. Recently Ranade et al. [3] showed that presence of a negative PET/ CT in a patient with rising Tg levels could be regarded as a favorable prognostic factor to predict symptom free status.
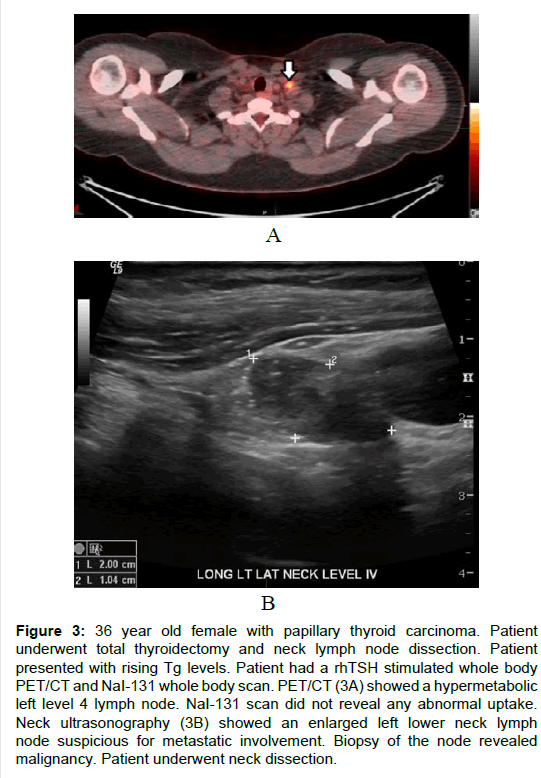
Figure 3: 36 year old female with papillary thyroid carcinoma. Patient underwent total thyroidectomy and neck lymph node dissection. Patient presented with rising Tg levels. Patient had a rhTSH stimulated whole body PET/CT and NaI-131 whole body scan. PET/CT (3A) showed a hypermetabolic left level 4 lymph node. NaI-131 scan did not reveal any abnormal uptake. Neck ultrasonography (3B) showed an enlarged left lower neck lymph node suspicious for metastatic involvement. Biopsy of the node revealed malignancy. Patient underwent neck dissection.
Our study has limitations. It is a retrospective study from a single institution. Only cases with rhTSH stimulation before PET/CT were included in the study. We did not include post therapy NaI WBS into consideration. Future studies assessing role of a negative post therapy NaI WBS will be useful.
In conclusion, our study showed that FDG PET/CT should be considered for patients with higher Tg levels in the presence of NRI. WDTC should be considered as a spectrum of disease rather than as a single entity. Decision making for obtaining FDG PET/CT should be made depending on individual patients’ clinical circumstances. Neck USG should be the first line imaging modality. PET/CT should be considered for cases where there are rising or high Tg levels with a normal neck USG.
Research reported in this publication was supported in part by the Biostatistics & Bioinformatics Shared Resource of Winship Cancer Institute of Emory University and NIH/NCI under award number P30CA138292. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.