Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2013) Volume 3, Issue 3
Introduction: The increasing prevalence of Adverse Drug Reaction (ADR) has been reported by many countries and to develop a good ADR reporting system is the need of present time.
Aim and objective: To assess attitude and awareness towards ADR reporting and factors that influences their reporting by health professionals.
Materials and method: The present cross-sectional study was conducted in seven hospitals in Makkah. All the health professionals were invited to participate in the study. A prescribed questioners was used to collect basic information, professional information and knowledge about ADR reporting system.
Results and conclusion: It was observed that most of the professionals were aware of ADR. They were having positive attitude to report ADRs. But major factor found as obstacle in ADR reporting were lack of training, non availability of forms, insufficient clinical knowledge and fear to report ADR.
Keywords: Pharmacovigilance, Adverse Drug Reactions (ADRs), Makkah, Attitude, Awareness, Health professionals, Saudi Arabia
Today, there is a public expectation that diseases can be alleviated by suitable use of drugs. The presence of Adverse Drug Reactions (ADRs) is considered to be a global problem and a major concern for causing unexpected morbidity and mortality [1]. This is reflected by ADRs being claimed to be responsible for many patient hospital admissions and based on meta-analyses and systematic reviews the percentage rate of admissions was 5% [2].
The increasing prevalence of ADR has been reported by many countries. For example: 12% in Sweden [3], 11.5% in Norway [4], 12.9% in New Zealand and 16.6% in Australia [5]. In USA 0.32% of death in hospital patients was due to ADR [6]. In 2000, the American Institute of Medicine reported around 6000 deaths annually due to the ADRs. In the United Kingdom (UK), studies showed during 1999-2008 the numbers of patients admissions for all NSH public English hospitals in England were 557,978 related ADRs which represented 0.9% of total hospital admissions. Every year the rate of ADRs is increased by 76.8% and the mortality rate increased by 10% [7]. This problem has economic cost for both the person and society, which cannot be predicted from the clinical trials due to their limitations in identifying ADRs for unexpected and/or rate events [8].
Thus ADR reporting is the cornerstone for any Pharmacovigilance system [9]. The attitude and awareness towards Adverse Drug Reaction (ADR) reporting shows great variation among the health professionals and many factors influences the reporting of ADR.
a) To assess attitude and awareness towards Adverse Drug Reaction (ADR) reporting and
b) Factors that influence their reporting by health professionals.
The present cross-sectional study was conducted in the Holy city of Makkah, Kingdom of Saudi Arabia. For this purpose the author visited seven hospitals in Makkah. Out of these hospitals 5 were general hospital and 2 were specialists hospitals, which were the King Abdul- Aziz Hospital, King Faisal Hospital, General Ajiad Hospital, Children and Delivery Hospital, Abin-Sina Hospital, Al-Noor Specialist Hospital and General Hira Specialist Hospital. All the health professionals were invited to participate in the study.
The study was fully explained to the participating health professional and they were assured about the anonymity and confidentiality of the data. The responses of the health professionals were collected on a pre-structured questionnaire either obtained at the same time as the distribution or collected over the next 12 weeks.
The questionnaire comprised of 5 groups of questions i.e. part A, B, C, D and E. The part A consists of Demographic information of health professionals. Information about Familiarity with the ADR reporting system was covered in part B. Purpose of the ADR reporting system was in part in C. Attitude towards ADR reporting and Constraint of ADR reporting in the City of Makkah was collected in part D and E respectively.
Statistics
The survey questionnaire was analyzed by the response to each question and their percentage value was calculated. In the analysis of all the questions, the total number of respondents to the questionnaire survey was considered, rather than the total number of respondents to each question.
A total of 470 questionnaires were distributed. Out of these 310 were completed and 160 questionnaires were returned blank. Thus the overall response rate for the study was 65.9%. The major reasons for non-completion were being too busy and/or unwilling to participate. Results of part A were shown in table 1. Out of the total 310 participants 70.3% were male and 29.7 % were female. Most of the patricians were in the age group of 31-40 yrs (45.8%). Only 34.8% professional were from Saudi whereas 65.2% professional were of non Saudi nationality. Out of total 310 professionals 205 (66.1%) were physicians, 25 (8.1%) dentist, 49 (15.8%) pharmacist and 31 (10.0%) nurses. Most of the professional were having bachelors and masters degree qualification. Thirty-five percent of the health professionals had experience between 11 to 20 years. Most of the professional (34.2%) spent 6-10 hours on continuing education per month. Only 39.1% professional were having internet facility. Commonly the health professionals did not have references available to check for ADRs. Only 35.2% professional were trained for to report ADR (Table 1).
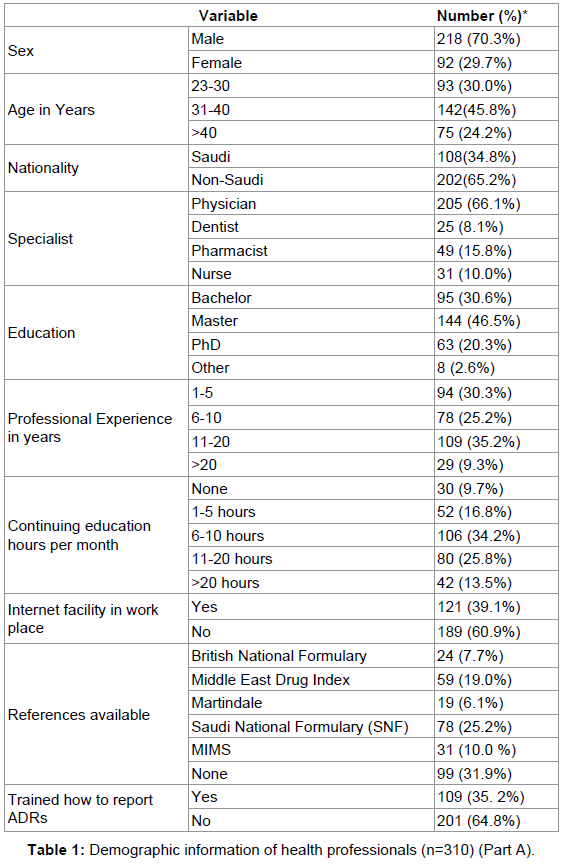
Table 1: Demographic information of health professionals (n=310) (Part A).
Familiarity with the ADR reporting system
The results revealed that 47.1% (n=146) of the responders were aware of existence of ADR reporting and monitoring system. 51.9% professional said that ADRs reporting program was present in their hospital. 59.1% professional were not aware of the existence of National Pharmacovigilance Center (NPC) in Saudi Food and Drug Authority (SFDA). 55.5% had learnt about the ADRs programme from official work and thirty-six percent of respondents thought the MOH was the department which was responsible for receiving the ADRs reports and interpreting them (Table 2).
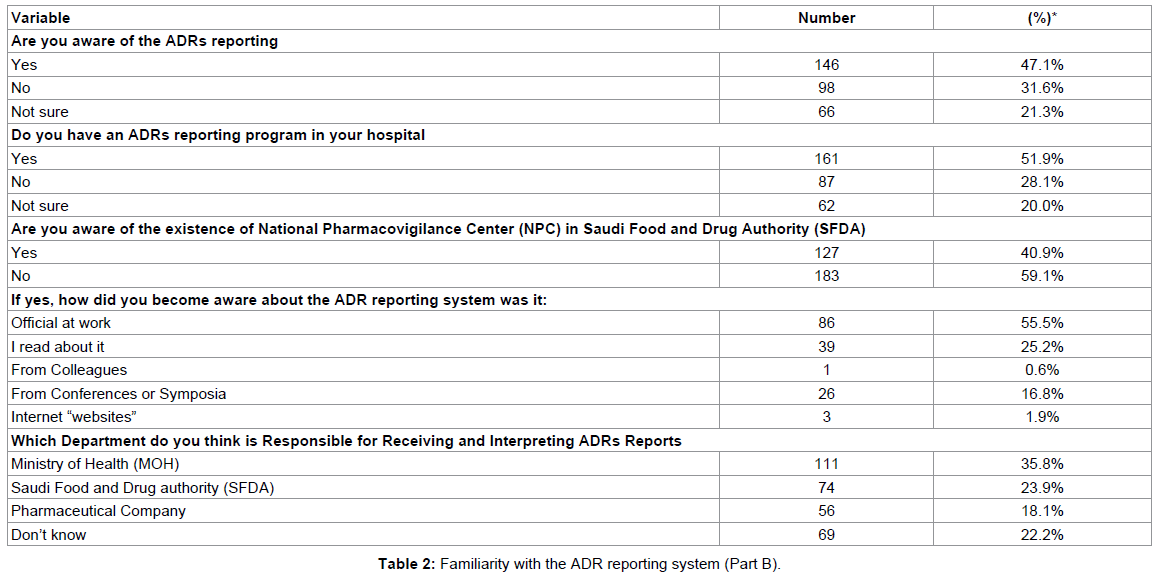
Table 2: Familiarity with the ADR reporting system (Part B).
The purpose of ADRs reporting system
50% of the health professionals think that the ADR reporting and monitoring system had benefited patients by identifying safe drug use. 46.1% professional opinioned that ADR reporting will simply identify rate of incidence. 54.2% of health professionals considered that the reporting system was to identify ADR within the same pharmaceutical class. 48.4% respondents considered the purpose of the ADR reporting was to detect potential ADRs. 42.9% of respondents thought the system served as a source of information about the characteristics of ADRs whereas 30.6% were not sure (Table 3).
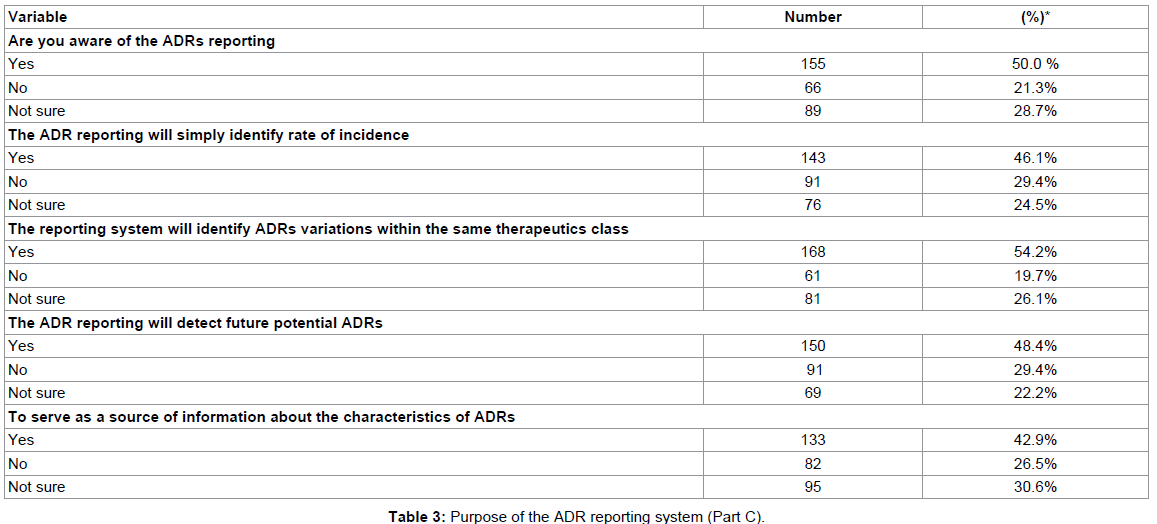
Table 3: Purpose of the ADR reporting system (Part C).
Attitude towards the ADR reporting system
70% of professionals were agreeing with the professional role of a pharmacist in reporting ADRs. 62.65 professionals believe that the science of monitoring drug safety is important. 79.4% professionals want to be sure that the ADRs is related to the drug before reporting. 69.4% professionals had experienced ADR in their professional practice. 73.5% thought that ADR reporting was an indication of taking patients’ complaints seriously. 70.9% professionals stated that they always report ADRs as a part of their tasks. And 71.3% thought that consulting the physicians is important before reporting ADRs. 67.1% professionals stated that ADR reporting should be compulsory. 47.1% professionals had come across ADR in last one month and they wished to report it. 33.2% professional had submitted ADR to Ministry of health whereas 21.65 had submitted to Pharmaceutical Company. Majority of professionals (41.6%) think that reporting ADR was the responsibility of pharmacist whereas according to 30.6% professionals ADR reporting should be done by physicians (Tables 4a and 4b).
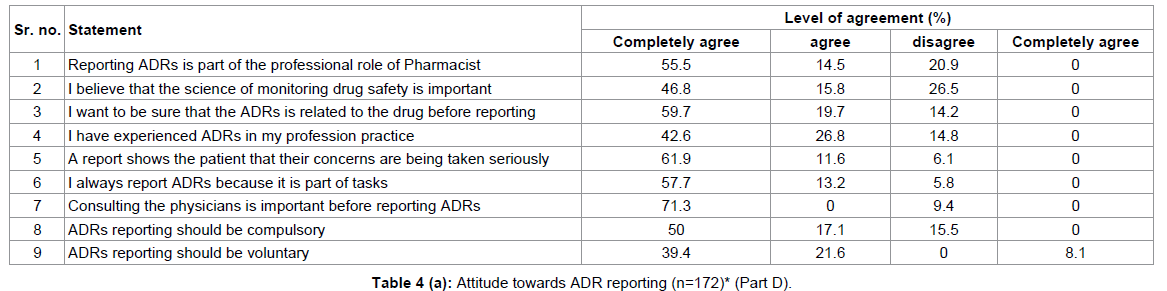
Table 4a: Attitude towards ADR reporting (n=172)* (Part D).
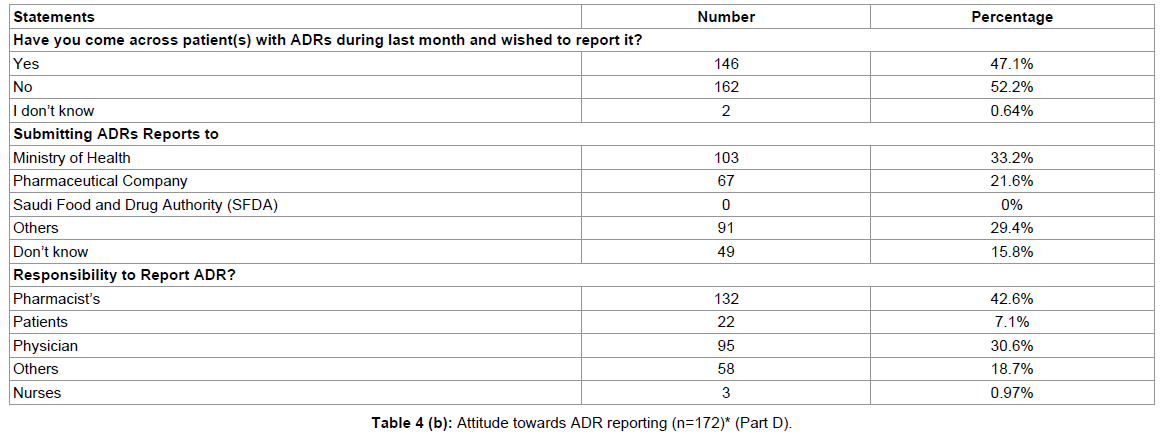
Table 4b: Attitude towards ADR reporting (n=172)* (Part D).
Constraint of ADRs reporting
Constrains in reporting of ADRs were also evaluated. It was found that according to 66.8% professionals ADR reporting forms were not available whereas 55.1 professionals didn’t know how to report ADR. 62.6% professionals agreed that they didn’t know the reporting address of ADR.
According to 50.4% professionals reporting form was too complicated whereas 58.1% believe that reporting ADRs was time consuming. One of the major constrain in reporting of ADR was insufficient clinical knowledge (64.9%). 52% of professionals believe that all ADR were already known. Finally, 57% of health professionals stated that the lack of ADRs reporting may reflect the fear to report such events (Table 5).
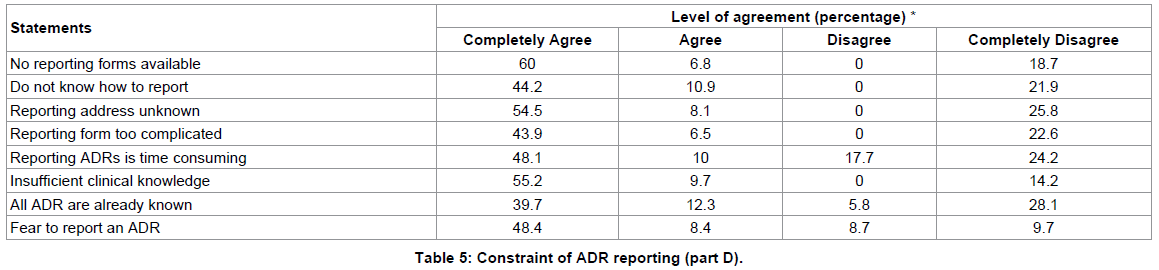
Table 5: Constraint of ADR reporting (part D).
The present study was conducted with the aim to investigate attitude and awareness of an ADR system among the health professionals of Makkah. Total 310 health professionals from seven hospital participated in the study. 70.3% of professionals were male. Most common age group of professionals in the study was 31 to 40 years. About 2/3rd of the professional were of non Saudi nationality. Maximum participants were physicians (66.1%) followed by pharmacist (15.8%). More than 90% of participants were having professional experience between 6 to 20 years. Most of professionals stated that they spent some time on continuing education per month. Majority of professionals spent 6 to 20 hours per month on continuing education. Non availability of internet facility and references was also observed. Only 35.2% of professionals were trained to report ADRs [10].
Familiarity with the ADR reporting system was also accessed (Table 2) in the present study. It was observed that the majority of health professional expressed an inadequate knowledge and awareness of the ADRs reporting program. These findings suggest that more cooperations are needed between the health professionals in the hospitals and central authorities to ensure that an awareness of ADR reporting is actually carried out. The low participation in the study and the failure to respond to some questions, especially for the definition of Pharmacovigilance and ADR, may be a consequence of poor knowledge of ADR. Purpose of ADR system was also analyzed in the present study. The study showed a positive attitude of the majority health professional towards ADR reporting. Most of the professionals were of opinion that ADR would identify safe drug and also variations within the same therapeutics class. 150 professionals stated that the ADR reporting will detect future potential ADRs.
While studying attitude towards ADR reporting, it was observed that most of the professionals believe that the science of monitoring drug safety is important. And reporting ADRs is part of the professional role of Pharmacist. Most of the professionals had experienced ADR and reported ADR in their practice. According to 67.1% professionals ADR reporting should be compulsory. The overall positive attitude of professionals was observed for reporting ADRs.
Confusion was observed regarding where ADR report should be submitted and who should be responsible for submitting ADR report. This problem could be corrected by simply providing more workshops and more courses by the NPC in SFDA to create a workforce which are qualified as ADRs reporters.
Major constrain in reporting of ADR was non availability of forms. Most of the professionals considered the process as being too time consuming. Insufficient clinical knowledge was observed in 64.9% whereas 56.8% professionals stated that they fear to report ADR. To overcome these problem regular continued education programmes should be held so that knowledge of professionals will be up to date and they will not fear to report ADR.
Rockville [11] and Bawazir [9] in their study found that underreported ADR was not by only pharmacists but by other health professionals as well. And the findings were consistant with the present study. Davis and Coulson [12], Bäckström et al. [13] and Toklu and Uysal [14] all of which assessed ADR reporting found that the reluctance to report ADRs included a lack of awareness of the specified medication in causing of ADR. According to Van Grootheest et al. [3], Al-Sultan and Bawazir [15] and Ghosh et al. [1], the awareness and attitudes of the respondents to ADRs may help develop a database of problems and can be utilized for improving ADR reporting system.
In the end we can conclude that most of the professionals were aware of ADR and importance of reporting ADR. Importance and purpose of ADRs reporting was also satisfactory in the professionals. But quite confusion was observed about who and where ADR reporting should be done. Major constrain in ADR reporting was lack of knowledge about ADR reporting procedure and shortage of prescribed forms. Improvement of communication and co-operation between health professionals and health organizations should encourage a reduction in the ‘gaps’ of awareness of ADR reporting among medical professionals. An improvement in training, using workshops and courses of continuous education relevant to ADRs reporting, would facilitate a better reporting culture [16-18].
The authors would like to thank the Saudi Cultural Bureau for providing a PhD Scholarship for Naif Al-Hazmi and all the health professionals in the Makkah hospitals who gave their time in providing data for this study.