Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
![]() +44 1478 350008
+44 1478 350008
ISSN: 2329-9509
![]() +44 1478 350008
+44 1478 350008
Review Article - (2015) Volume 3, Issue 3
Recently much attention has been given to the possible relationship between the use of bisphosphonates and some low-energy femoral fractures. These fractures were named “atypical fractures” to distinguish them from “typical fractures” that occur in the neck and trochanteric region of low energy trauma in the elderly and in the femoral shaft. Atypical fractures are stress fractures that occur in the femur (subtrochanteric or diaphyseal region) and are closely related to chronic use of bisphosphonates. Although the pathogenesis of atypical fracture of the femur remains unclear, several pathological mechanisms have been proposed. It is believed that prolonged use of bisphosphonates decrease osteoclast activity by reducing bone’s ability to remodel and leading to an accumulation of micro damage with reduced bone strength. There is a prodrome period of pain before the fracture is complete. The patients using bisphosphonates should be advised about the appearance of symptoms that might indicate a possible atypical femoral fracture. The emergence of pain in the groin or thigh should be investigated. Conventional radiography is usually the initial imaging procedure, followed by magnetic resonance imaging (MRI), computed tomography (CT) or bone scan. Symptomatic patients with an incomplete fracture can be treated conservatively or can have a prophylactic fixation indicated. For patients with atypical fractures or a stress reaction, the bisphosphonates must be stopped and adequate supplementation of calcium and vitamin D should be started. Alternatively, the use of parathyroid hormone (PTH) or others bone anabolic agents can be used in some cases.
<Keywords: Atypical femoral fractures; Bisphosphonate; Osteoporosis; Bone remodeling
Osteoporosis is an important public health problem that contributes substantially to morbidity and mortality in an ageing world population. The lifelong risk of having a fracture related to osteoporosis is approximately one in two for women and one in four for men. Bisphosphonates (BP) are the most commonly used drug in the treatment of osteoporosis and have an excellent safety profile. Bisphosphonates, including alendronate, risedronate, ibandronate, and zoledronic acid, have proven efficacy in reducing the incidence of spine, hip, and all non-spine fractures [1-6]. Nowadays, randomized controlled trials demonstrate that each of this BF reduces the incidence of vertebral and non-vertebral fractures by about 50% [2-5].
Recently, much attention has been given to the possible relationship between prolonged use of BP and some low-energy femoral fractures. These fractures were named “atypical fractures” (AFF) to distinguish them from “typical fractures” that occur in the neck and trochanteric region of low energy trauma in the elderly and in the femoral shaft that occur in high-energy trauma, such as accidents transit or falls from a height in young adults. The first report on a possible relationship between prolonged use of BP and “atypical fractures” of the femur was Odvina et al. [1]. They described nine patients who had femoral shaft fractures, proximal femur, sacrum, ischium, pubis and ribs. Most patients presented delayed healing accompanied by suppressed bone remodeling. All patients were treated with alendronate; some of them received estrogen and glucocorticoid (known suppression of bone remodeling agents). After this first article, numerous case reports and reviews about atypical fractures characterized the clinical and radiological findings. Several retrospective case-control studies and epidemiologic papers were published later.
In this review article we address the atypical fractures and the association with the chronic use of bisphosphonate as the features, epidemiology, pathogenesis and management.
Atypical fractures are stress fractures that occur frequently in the femur (subtrochanteric or diaphyseal region) and are closely related to chronic use of bisphosphonates. However, the risk of atypical fracture decreases rapidly after discontinuation of treatment, what suggests acute effects of bisphosphonate during its use [2].
Features described in case reports and series differentiating AFF from the common low energy osteoporosis related hip fractures included: Prodromal pain described as discomfort, weakness, or actual pain involving the thigh or lower limb for weeks or months preceding the fracture, use of another anti resorptive or steroid therapy, in addition to the bisphosphonate, lack of trauma precipitating a fracture, bilateralism (either simultaneous or sequential), transverse or short oblique fractures, cortical hypertrophy or thickness, stress reaction on the affected and/or unaffected side, poor fracture healing and normal or low bone mass but not osteoporosis in the hip region [2-6].
Some radiographic features in AFF associated with BFF use: transverse or short oblique, not comminuted, with the presence of bone spicules, subtrochanteric or femoral shaft [3-5]. We can observe either an increase in the cortical region of the stress fracture.
Due to diagnostic difficulties the American Society for Bone and Mineral Research (ASBMR) established some criteria to try to define atypical femoral fractures, and all the major criteria must be present to designate a fracture as atypical and distinguish it of an osteoporosis fracture. Smaller criteria also have association with atypical fractures, but they are not necessary for diagnosis [6] (Table 1).
| Major Features | Minor Features |
|---|---|
| No history of trauma or associated with low-energy trauma. Fracture located anywhere from distal to the lesser trochanter to proximal to the supracondylar area. Transverse or short oblique fracture configuration. Noncomminuted fracture. Medial spike in complete fractures; incomplete fractures involve only the lateral cortex. |
Localized periosteal thickening of the lateral cortex. Generalized thickening of the femoral cortices. Prodromal symptoms. May be associated with bilateral fractures or symptoms. Evidence of delayed fracture-healing. Comorbid conditions or the use of some medications(rheumatoid arthritis, rickets and osteomalacia, renal osteodystrophy, and the use of bisphosphonates, glucocorticoids, or proton pump inhibitors). |
Table 1: Major and minor features for diagnosing atypical femoral fractures (*All major features, accompanied by none or some of the minor features, are required to diagnose atypical femoral fractures) (ASBMR).
There is an evolution in the epidemiological studies published to AFFs from its first recognition to the present time. Nieves and Cosman published a summary of epidemiological studies that contribute to our knowledge of AFFs in 2010 [5]. They classified the report on case studies, case series and epidemiological studies. These reports are before the first Task Force Report ASBMR 2010.
The first case report was published in 1997 describing a subtrochanteric stress fracture of the femur after total knee arthroplasty [7]. The clinical entity remained difficult to identify until the mid- 2000s. Reports and case series have emerged from 2005 [8] and 2009 [9,10]. Odvina et al [11] published the first case series of AFFS in which five of the ten reported cases were of femoral fracture.
Wang et al [12] found a decrease in age-adjusted rates for typical hip fractures 31.6% among women and 20.5% among men from 1996 to 2007. This contrasted with an increase of 20.4% in failure subtrochanteric fractures among women, but no trend in men during the same period. At the same time there was an increasing trend in the use of BPs. It is also noted that women were the predominant users of BPs, and the vast majority of cases of subtrochanteric fractures.
Some studies have attempted to predict the risk of fracture of the femur with cortical lesions stress. Based on their findings (a transverse black line in the X-ray) those with AFF incomplete, especially if symptomatic, have a high risk of progression to complete the fracture (42-80%) while those with no black line stress injuries healed with conservative treatment [13].
Although the pathogenesis of atypical fracture of the femur remains unclear, several pathological mechanisms have been proposed. The localized cortical thickening hints of a “fatigue fracture” caused by excessive repetitive load in a normal bone, while an “insufficiency fracture” indicates a normal load in an abnormal or insufficient bone. On a fatigue fracture micro cracks that arise are not repaired and accumulate. Over time the micro cracks generate a defect of critical size precipitating a complete fracture [14]. It is believed that due to prolonged use of bisphosphonates there is a decrease in osteoclast activity, reducing the ability of bone remodeling leading to an accumulation of micro damage and reduced bone strength. Usually there is a prodrome period of pain before the fracture is complete.
Bisphosphonates inhibit bone resorption by suppressing the activity of osteoclasts. Although clinical trials clearly sustain the beneficial effect of bisphosphonates in preventing osteoporotic fractures there is a concern that prolonged therapy may lead to severe suppression of bone remodeling (“frozen bone”) and increase skeletal fragility [1,15]. Beyond the risk of atypical fracture in bisphosphonates use, there are some reported cases that associate the use of Denosumab and AFF too. Denosumab is a fully human monoclonal antibody to the receptor activator of nuclear factor kappa B ligand (RANKL), an osteoclast differentiating factor. It inhibits osteoclast formation, decreases bone resorption, increases bone mineral density (BMD), and reduces the risk of fracture [3,4].
Usually the cases described are younger women treated with bisphosphonates for several years without trauma with pain prodrome in the middle of the thigh and atypical radiographic images for usual subtrochanteric fractures. Such as cortical thickening and a transverse orientation of fracture in plain radiographs obtained before the fracture [16,17].
Although the long-term use (average of 7 years) of bisphosphonates increases the relative risk of atypical fractures the absolute risk is low (3.2 to 50 cases per 100,000 person-years) increasing with the exposition time. Results from a recent population-based case control study, again without adjudication of X-rays, showed a significant increase in risk of subtrochanteric and shaft fractures in women with long term bisphosphonate use (≥ 5 years) compared to those with shorter-term use (odds ratio, 2.74; 95% CI: 1.25, 6.02) [18]. A patient with an atypical femur fracture in one side is at risk of a fracture on the other femur. With the removal of the bisphosphonate the risk decreases. Patients usually have prodromal symptoms of pain in the groin or thigh. In retrospect can be noted cortical thickening in plain radiographs obtained before the break. The evaluation is recommended in patients with early pain after starting the use of bisphosphonates especially for over 3 to 10 years [19].
Chronic oral bisphosphonates therapy represents a potential risk of atypical femoral fracture. A report with 62 cancer patients who received intravenous bisphosphonates (IVBP) identified 6 cases of AFF, which was associated with a greater number of total IV BP doses and longer treatment duration. But prospective studies should be conducted to evaluate the association of IV BP and AFF [20] .Recent results from a phase II study of the potent IV BP suggest that intravenous administration of this agent may be an effective therapy for osteoporosis. Thus, in postmenopausal women, a single intravenous dose of 4 mg zoledronate produced changes in bone density 1 year later that were equivalent to those observed in women treated with lower doses of the same agent more frequently and comparable with those seen in response to potent oral BP. If these studies demonstrate anti-fracture efficacy, the clinician will have a greater range of proven therapeutic options available for fracture prevention. If these studies demonstrate anti-fracture efficacy, the clinician will have a greater range of proven therapeutic options available for fracture prevention. In the coming era of anabolic agents for osteoporosis, it remains to be determined whether any of the bisphosphonates might confer greater benefits than other members of the class when used in combination or sequence with drugs that stimulate bone formation.
The patients using bisphosphonates should be advised about the appearance of symptoms that might indicate a possible atypical femur fracture. The principal and early symptom is pain. The emergence of pain in the groin or thigh should be investigated. Conventional radiography is usually the initial imaging procedure, followed by magnetic resonance imaging (MRI), computed tomography (CT) or bone scan is indicated. Symptomatic patients with an incomplete fracture diagnosed by imaging methods can be treated conservatively with full or partial weight support of affected limb with accessory devices (crutches or walker) or have a prophylactic fixation (Figure 1) [14].
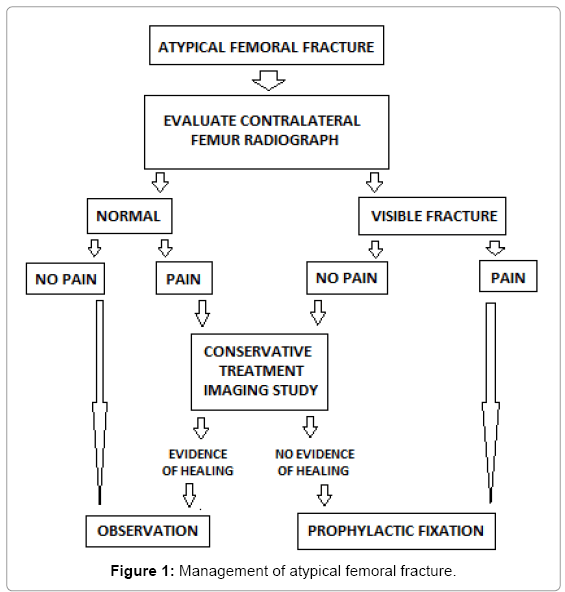
Figure 1: Management of atypical femoral fracture.
When fracture has been diagnosed, use of bisphosphonates should be halted. The idea of vitamin D and calcium supplementation should be evaluated and must be maintained; introduction of bone anabolic agents should be considered (denosumab or teriparatide). Laboratory tests can be used to identify any predisposing metabolic conditions. The contralateral side should be evaluated, (risk of bilateral involvement is 28-44.2%), and the best fixation method chose. No controlled studies comparing fixation using plates and screws with intra medullar fixation have been conducted. Stems have the theoretical benefit of healing through endochondral repair. There is a preference for using nails for treating atypical femoral fractures [6,19-21]. Despite the better knowledge available, the prognosis for these fractures is still poor, with descriptions of reoperation in up to 44% of the cases in some series. The healing time changes between 12 to 60 months [19-21].
The screening for evaluating bone abnormalities in all patients receiving bisphosphonates is inadequate because of the low incidence rate of these fractures and because radiological abnormalities are often unidentifiable [15,17,20-21]. Nevertheless, in view of the presence of pain of mechanical pattern in patients who make chronic use of bisphosphonates, careful assessment needs to be made using serial x-ray, bone scan and magnetic resonance imaging, in order to institute early diagnosis and treatment.
Many questions related to atypical femoral fractures still do not have answers. Further studies aiming toward better histomorphometric and bone biomechanical evaluations and the relationship of these fractures to certain medications are paramount. Moreover, discussion toward creating a national and international register of atypical femoral fractures will ensure better understanding and discussion of these cases.
The available literature shows that many of the younger patients with osteopenia without risk factors does not need treatment and may be wise wait until more precise data be available. However, in elderly patients with osteoporosis or with failure fractures, the benefit of the use of BPs on the basis of available evidence is high. All these patients should be properly assessed and treated promptly. A treatment period of 5 years is safe but patients should be advised to reassess if pain in the hip or thigh appears.
None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of any aspect of this work.