Journal of Pollution Effects & Control
Open Access
ISSN: 2375-4397
ISSN: 2375-4397
Review Article - (2014) Volume 2, Issue 2
The aim of this review is to summarize epidemiological studies on the relationship between air exposure to benzene and respiratory health among children and adolescents. To the best of our knowledge, no previous review on this topic has been published. An exhaustive search in on-line bibliographic databases (PubMed and Web of Science) was carried out in April 2014. We selected observational analytical studies with individual data analyzing outdoor, indoor and personal exposure to benzene, and their association with at least one respiratory health outcome in children aged up to 18 years old. Fourteen papers published between 1999 and 2014 were selected (five for indoor, six for outdoor and three for personal exposure). In general, benzene exposure levels found in the studies were low, ranging between 1.5 and 24.8 μg/m3. Indoor exposure was higher than outdoor and personal exposure. Overall findings suggest that an increase in benzene exposure could impair respiratory health (asthma, lung function and pulmonary infections) in children aged up to 18 years old. However, since great diversity in methods and study designs exist, comparisons between results are hampered. Further research is needed to broaden knowledge on the effects of benzene on respiratory health during childhood.
Keywords: Air pollution; Benzene; Respiratory health problems; Children; Adolescents
Seven million premature deaths in the year 2012 could be attributable to air pollution, according to the World Health Organization (WHO) in its last Burden of Disease report [1]. Around 4.3 out of 7 million were caused by ambient air pollution and 3.7 million by household air pollution. In recent years, evidence regarding air pollution effects on the child respiratory system are growing considerably and they are observable at normal levels [2,3]. An impairment of respiratory health during childhood has been related with both indoor [4,5] and outdoor [6,7] air pollution.
Respiratory diseases are among the main causes of child morbidity and mortality. Currently, pneumonia along with diarrhea is the major cause of death in children under five years old [8]. Moreover, because of their physiologic and behavioral features, children are more exposed to air pollutants than adults and their vulnerability to respiratory illnesses is also higher [6,8-10]. Consequently, studies conducted to broaden knowledge about risk factors for respiratory child health are relevant.
Benzene, which is a volatile organic compound (VOC), is a constituent of petroleum and a well-known solvent. Therefore, traffic vehicles, gas station emissions, some industries, tobacco smoke, and some cleaning products are the main emission sources of this pollutant [11]. The potential of carcinogenic and immunologic effects after chronic exposure is well known [11-13]. Furthermore, chronic benzene exposure has also been related to respiratory problems, such as asthma and lung infections in children [14,15] and/or adults [16,17].
A wide variety of reference levels for benzene exposure exists worldwide. In the US, the Integrated Risk Information System (IRIS) of the Environmental Protection Agency (EPA) established 30 μg/m3 as reference concentration for inhalation (RfC) [18]. In addition, the Agency for Toxic Substances and Disease Registry (ATSDR) proposed as the minimal risk level (MRL) for benzene inhalation the levels of 0.009 ppm (2.8 μg/m3) and 0.006 ppm (1.9 μg/m3) for an acute and intermediate term exposure, respectively. In occupational exposure, the National Institute for Occupational Safety and Health (NIOSH, [19]) also established 0,1 ppm (31.3 μg/m3) as recommended exposure limits (REL) for a 10-hour exposure to benzene. More recently, a European regulation established an annual boundary value in ambient air for benzene ensuring human health of 5 μg/m3 (CE 50/2008 [20]). However, due to the sufficient evidences for categorizing benzene as a carcinogen, WHO has not considered any threshold level devoid of risks for exposure to this compound [13]. A level of 1.7 μg/m3 is considered by this organization as a guideline not to be exceeded since it has been associated with an increase of 1/100000 in the lifetime risk of suffering cancer [21].
Summaries of the scientific knowledge could help to update the state-of-the-art and to address preventive and regulatory measures. Previously, other reviews have already summarized indoor and outdoor exposure to air pollutants in relation with respiratory health in children and adults, including a general section for VOCs within the pollutants assessed [4,15,22]. However, to the best of our knowledge, no review studies have been carried out to summarize the relationship between benzene exposure and respiratory health in child populations. The aim of this review is to summarize the epidemiological studies on the relationship between air exposure to benzene, directly measured, and respiratory problems among children.
We carried out a literature search from 20th to 30th April 2014 (Figure 1). The study period covered papers published in the last 16 years (1999-2014). Eligibility criteria were:
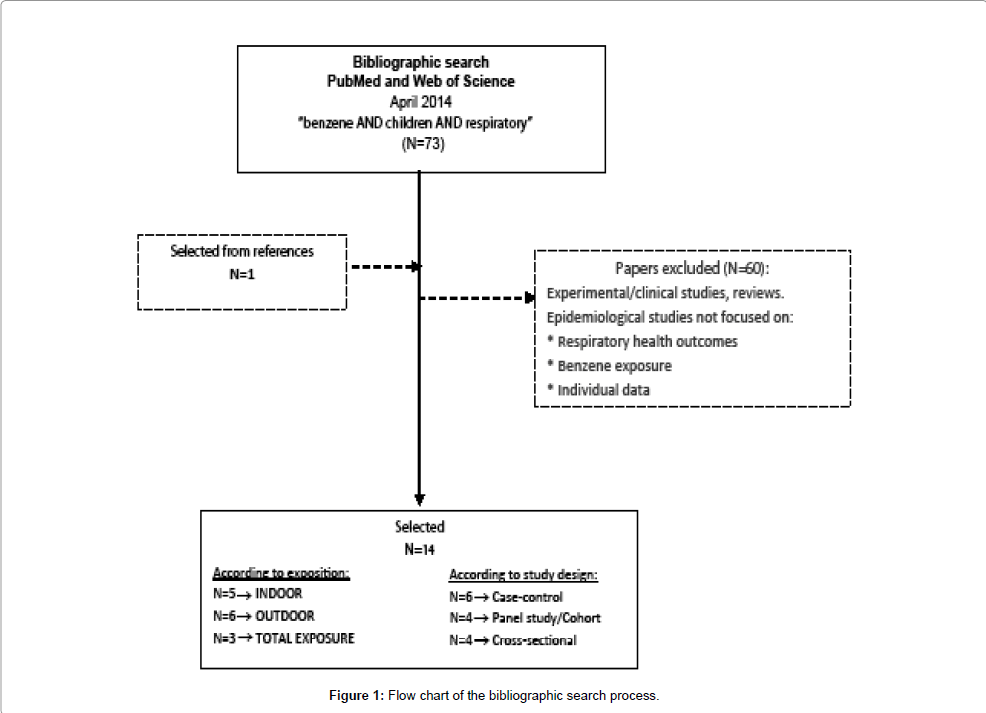
Figure 1: Flow chart of the bibliographic search process.
• Literature published on-line in the bibliographic databases PubMed and Web of Science. Terms used were “benzene” AND “children” AND “respiratory”. After that, we also combined the following MeSH terms (“benzene”, “child”, “respiratory tract infections”, “respiratory sounds”, “signs and symptoms, respiratory”). However, the resulting papers were duplicated and were fewer than in the previous search.
• Relevant studies found on reference lists of the selected papers if fulfilling the eligibility criteria.
• Studies on associations between indoor, outdoor and personal exposure to benzene and respiratory problems in children up to 18 years old.
• Observational analytical studies based on individual data (i.e.: cohort, panel study, case-control and cross-sectional reports) were selected.
In a first phase, the information was assessed by reviewing the titles and abstracts. Then, the whole content was carefully read and references were checked.
Information was summed up in tables. Eight main rubrics were considered: Paper reference (Author, year of publication), year of study and location, study design, population according to age and sample size, outcome and tools used, benzene exposure assessment (divided into data source, levels found and interpolation method, when applied), other pollutants measured in the study apart from benzene, adjusted variables in the analysis, and results (that is associations between benzene and respiratory outcomes). We classified all papers into three categories according to benzene exposure assessment: those analyzing indoor air (Table 1), outdoor air (Table 2) and personal exposure (Table 3). All benzene exposure levels reported were converted to the same unit (μg/m3) and presented graphically (Figure 2) in order to enable comparisons between levels obtained from different studies.
| REFERENCE |
YEAR OF STUDY AND LOCATION | STUDY DESIGN | POPULATION | OUTCOME (INSTRUMENTa)) |
BENZENE EXPOSURE ASSESSMENT | OTHERd POLLUTANTS | ADJUSTEDe VARIABLES | RESULTS | |||
| AGE | SAMPLE SIZE | DATA SOURCEb | LEVELSc Median (range) in μg/m3 |
Unit of benzene increase | OR (95%CI) | ||||||
| INDOOR EXPOSURE | |||||||||||
| Rive et al. [23] |
1999-2000 Clermont-Ferrand (France) |
Case-control | 13-14 years | Case (asthmatics) 32 Controls (non-asthmatic) 31 |
Asthma symptoms (ISAAC Q) |
Passive samplersLiving room1 week | Total 2.4 (0.5,53.5) Cases 3.9 (0.8,53.5) Controls: 1.9 (0.4,14.5) (p<0.05) |
Urinary S-PMA | Age Sex ETS Atopic status Familial allergy |
High exposure (>2,4 μg/m3) in reference to low exposure | Woken up by a breathlessness crisis 10.10 (2.06-49.78)Urinary S-PMA levels higher in asthmatic children and correlated with benzene. |
| Gordian et al. [17] |
2008-2009 Anchorage (Alaska) |
Cross-sectional | Children (0-19 years)Adults |
1484 458 |
Asthma symptoms (ISAAC Q) | Passive samplersLiving room1 week | Median (min, max): 9.3 (<1.28, 186.0) |
Other VOC | - | High exposure (> 28.7 μg/m3) in reference to low exposure (< 9.6) |
Severe asthma 2.49 (1.22, 5.07) |
| Hulin et al. [24] |
2003-2004 – Urban area2006-2007 – Rural areaClermont-Ferrand (France) |
Case-control | 10-14 years | Urban area Case (asthmatics) 32 Controls (non-ast) 31Rural area Asthmatic 24 Non-asthmatic 27 |
Asthma (ISAAC Q) |
Passive samplersLiving room1 week | Acetaldehyde 13.6 (5.9,158.7) Benzene: 1.8 (0.3,53.5) Toluene: 20.2 (2.1,522.5) |
NO2 PMOther VOC |
Age Sex Familial allergy ETS Allergic rhinitis Location Season |
Benzene (for >1.8 µg/m3) |
Asthma 1.30 (0.40-3.80) |
| Rumchev et al. [25] |
1997-1999 Perth (Australia) |
Case-control | 6 months to 3 years |
Case (asthmatic) 88 Controls (non-asthmatic) 104 |
First diagnostic of Asthma (emergency department) |
Passive samplersLiving room2 weeks each season (winter and summer) |
Cases 24.8 (0.01,81.9) Controls 11.8 (0.01,58.9)p<0.01 |
Other VOC | Age, sex, atopy, socioeconomic statusSmoking indoors, presence of air conditioning and house dust mites | 10mg/m3 | Asthma 2.92 (2.25-3.80) |
| Diez et al. [26] |
1995-1996 Leipzig (Germany) |
Cohort | 6 weeks 1 yearsChildren with allergic risk factorsf |
475 | Pulmonary infections Wheezing (Q) |
Passive samplers Dwellings4 week Period: pregnancy |
Smoker dwellings 6.1 (SD: 5.3)Non smoker dwellings 4.7 (SD: 4.8) |
StyreneOther variables by Q: Restoration, smoking |
Gas cooking Heating Flat size New furniture Domestic animals |
>5.6 µg/m3 | Pulmonary infections In week 6: 2,40 (1,30-4,50)Analysis for benzene were not done for the first year of life |
Table 1: Summarized results from studies analyzing the relationship between indoor exposure to benzene and respiratory health in children.
REFERENCE |
YEAR OF STUDY AND LOCATION | STUDY DESIGN | POPULATION | OUTCOME (INSTRUMENTa) |
BENZENE EXPOSURE ASSESSMENTb | OTHERc POLLUTANT | ADJUSTEDd VARIABLES | RESULTSe | ||||
| AGE | SAMPLE SIZE | DATA SOURCE | INDIVIDUAL ASSIGNMENT | LEVELS Mean (SD) in μg/m3 |
Unit of benzene increase | OR (95%CI) | ||||||
| OUTDOOR EXPOSURE | ||||||||||||
| Zora et al. [27] |
2010 El Paso, Texas (USA) |
Panel study | 6-12 years Asthmatics |
36 | Asthma (asthma control questionnaire score –ACQ-) |
Passive samplers In the roof or in fenced area in 2 elementary schools near/far of major roadways 5 days | - Individual exposure according to nearest sampler | School 1 1.5 (0.5) School 2 0.5 (0.2) |
PM BC NO2 Toluene O3 |
Relative humidity Temperature School | IQR (0.8 mg/m3) |
ACQ increase 0.03 (-0.07,0.13) Daily ICS increase: 0.17 (0.04,0.31) |
| Aguilera et al. [28] |
2003-2008 Asturias Gipuzkoa Sabadell Valencia (Spain) |
Cohort | 12-18 months | 2199 | Diagnosed LRTI Wheezing (Q) |
Passive sampler Ambient air 4 weeks Period: pregnancy |
LUR models Residential predictions temporally adjusted for trimesters pregnancy and first year of life | Pregnancy estimates 1.6 (0.9) 1st trimester 1.6 (1.2) 2nd trimester 1.5 (1.1) 3rd trimester 1.5 (1.1) First year estimates 1.6 (0.9) |
NO2 | Breastfeeding, Child care attendance, Siblings at birth, Familial history of asthma and allergies Maternal age at delivery BMI Prepregnancy Cotinine |
1 mg/m3 | RR (95%CI) 2nd trimester pregnancy LRTI 1.10 (1.01,1.20) Wheezing 1.02 (0.96,1.09) POSTNATAL LRTI 1.01 (0.94,1.09) Wheezing 0.97 (0.90,1.05) |
| Penard-Morand et al. [29] |
1999-2000 Bordeaux, Clermont-Ferrand, Créteil, Marseille, Strasbourg and Reims (France) |
Cross-sectional | 9-11 years | 6683 | Exercise induced asthma –EIA (Spirometry) Asthma symptoms and diagnosis (ISAAC Q) |
Active sampler Central Site measurements Annual mean concentrations (3 years averaged) |
Dispersion model Predictions for 108 school addresses | More and less contaminated cities Marseille 3.3 (min: 2.2, max: 5.1) Reims 1.5 (1.3,2.0) |
Other VOC CO NO2 NOx PM10 SO2 |
Age, Sex Older siblings Family history of allergy Parental education Mother’s origin Smoking at home Mould or dampness Natural gas used for heating, cooking or for water-heater at home, and pets at home |
IQR (2 mg/m3) |
EIA 1.32 (1.03,1.82) Asthma current 1.36 (1.00,1.96) Asthma ever 1.25 (1.08,1.43) |
| Delfino et al. [30] |
1999 Los Angeles (United States USA) |
Panel study | 10-16 years | 21 Asthmatic children |
Lung Function (Spirometry) Asthma severity (Daily diary) |
Active sampler Central Site measurements 24 hours | - Mean exposure levels obtained by samplers in the same day as symptom reports | Ambient 5.7 (2.7) In Breath in ng/L 2.2 (2.7) Correlations Breath-Ambient air 0,3 (p<0,01) |
Other VOC O3 NO2 SO2 CO VOC In EBC |
Respiratory infections Temperature Two pollutants models |
(mean concentration) | Breath benzene Asthma severe symptoms 2.06 (0.85,4.96) Ambient benzene Asthma severe symptoms 5.93 (1.64,21.4) PEF deficit -26.3 l/min (-51.4,-1.3) When other ambient pollutants were introduced in the models the association became non significant for benzene. |
| Nicolai et al. [31] |
1995-1996 Munich (Germany) |
Cross-sectional | 5-7 years 9-11 years |
7509 | Asthma symptoms (ISAAC Q) |
Passive samplers 18 heavy traffic sites 16 low-to-medium traffic sites –schools- in the city. 4 weeks |
Non-linear regression model, taking into account traffic variables Residential predictions | City 8.7 (2.4) Schools 2.6 (0.6) |
Daily traffic counts Soot NO2 |
Age Sex Socioeconomic status Family history of asthma Hay fever, or eczema. |
1 mg/m3 | Current asthma 2.05 (1.23,3.41) Current wheeze 1.65 (1.06,2.55) Cough 1.42 (1.01,2.01) Current asthma with Benzene+ETS 2.41(1.24,4.69) |
| Hirsch, et al. [32] |
1995-1996 Dresden (Germany) |
Cross-sectional | 5-11 years | 2796 | Asthma symptoms (ISAAC Q) Bronchitis (ISAAC Q) Lung Function (Spirometry) |
Active sampler Monitored in 182 points in a 1kmx1 km grid over the area. Annual immission | - Residential and school exposure according to nearest sampler | 4.0 (min:1.9, max:8.7) | SO2 NO2 CO O3 |
Sex Age group Birth weight Parental education Maternal smoking Season of testing Central heating Furry pets Damp housing Carpets Floor level |
1 mg/m3 | Exposure at home: MORNING COUGH 1.15 (1.04,1.27) No-atopics 1.26(1.08,1.46) ASTHMA 1.11(0.97,1.25 FEF25-75 1.27(1.03,1.58) BRONCHITIS 1.11(1.03,1.19) Exposure at school: MORNING COUGH 1.21(1.04,1.40) ASTHMA 1.21 (1.01,1.45) FEF25-75 1.27 (1.03,1.58) BRONCHITIS 1.16 (1.04,1.29) |
Table 2: Summarized results from studies analyzing the relationship between outdoor exposure to benzene and respiratory health in children.
| REFERENCE | YEAR OF STUDY AND LOCATION | STUDY DESIGN | POPULATION | OUTCOME (INSTRUMENTa) |
BENZENE EXPOSURE ASSESSMENT b | OTHERe POLLUTANT | ADJUSTEDf VARIABLES | RESULTS | ||||
| AGE | SAMPLE SIZE | DATA SOURCE | PERSONAL ASSIGNMENT | LEVELS in μg/m3 |
Unit of benzene increase | OR (95%CI) | ||||||
| PERSONAL EXPOSURE | ||||||||||||
| Smargiassi et al. 2014 [33] |
2009-2010 Montreal (Canada) |
Panel study | 7-12 years Asthmatics |
72 | Lung Function (Spirometry) |
Passive sampler Personal monitoring (samplers in backpack) 24 hour |
- Personal exposure according to sampler levels |
Mean (SD)= 2.8 (2.3) |
SO2 PM2.5 NO2 PAH |
Age Sex Height Ethnicity Level of education Caregiver Temperature Humidity Use of bronchodilators Steroids Hay fever Eczema Allergies Asthma Mother smoker |
IQR (2.4 mg/m3) |
Mean change in FVC: -1.80 (-15.90, +12.20) -0.70 (-14.70, +13.20) -1.20 (-15.20, +12.70) -2.50 (-16.40, +11.50) Mean change in FEV1, FEF25-75 are neither significant. |
| Martins et al. 2012 [34] |
2006-2007 Viseu (Portugal) |
Panel study |
6-8 years Wheezing children |
51 | Wheezing (ISAAC Q) Need of rescue medication (Q) Lung Function (Spirometry) |
Passive samplers OUTDOOR Mobile laboratories: -In the city center -School courtyards INDOOR -Houses (bedroom) -Schools (classroom) 4 weeks |
Dispersion model Personal exposure estimations based on time-activity patterns | Mean (min, max) Visit 1: 2.9 (1.2,25.7) Visit 2: 1.0 (0.5,3.5) Visit 3: 10.7 (3.6,39.2) Visit 4: 1.6 (0.7,13.9) |
OUTDOOR: Other VOC O3 NO2 PM10 INDOOR: Other VOC O3 NO2 |
Sex, Age Atopy, Height, Weight, Older siblings, Parental education Parental smoking, Temperature, Humidity, Pets at home, Fireplace at home, and Mould or Dampness at home |
10 μg/m3 | Regression coefficients Wheezing -0.23 (-1.07, + 0.61) Rescue medication + 0.76 (-0.11, +1.62) Change in FEV1% -4.33(-7.13,-1.53) Change in FEV1/FVC -1.71(-3.24,-0.18) Change in FEF25-75 -5.89(-10.16, -1.62) Change in FEV1% +2.79 (+0.92, +4.65) |
| Hwang et al. 2011 [35] |
2008 Seoul (South Korea) |
Case-control | 8-9 years 10-13 years | 33 Case (asthmatics) 40 Controls (non-asthmatics) |
Asthma (ISAAC Q) |
Passive samplers Personal Exposure (attached to respiratory area) Indoor exposure (in living room) Outdoor exposure (in veranda) In 3 working days |
NS Time-activity patterns | GM (GSD) Personal: 2.4 Cases 2.5 (2.6) Controls 2.3 (3.2) Indoor: 2.2 Cases 2.8(2.6) Controls 1.7(2.7) (p<0.01) Outdoor: 2.1 Cases 2.7(2.1) Controls 1.6(2.9) (p<0.01) |
Other VOC | Age Sex Income background Level of education Passive smoking |
NS | Asthma 1.00 (0.90,1.20) |
Table 3: Summarized results from studies analyzing the relationship between personal exposure to benzene and respiratory health in children.
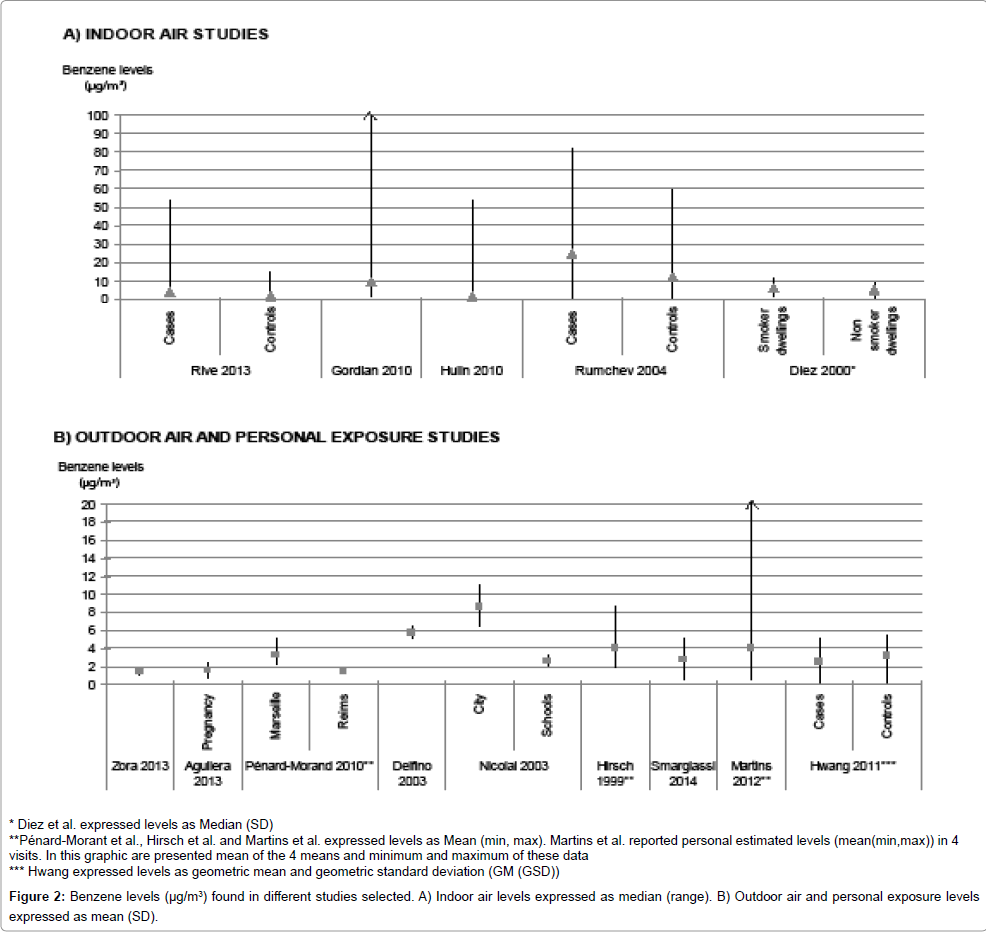
Figure 2: Benzene levels (μg/m3) found in different studies selected. A) Indoor air levels expressed as median (range). B) Outdoor air and personal exposure levels expressed as mean (SD).
After the literature search, 75 papers were retrieved and 14 of these were selected according to eligibility criteria (Figure 1). Five articles were found for indoor air [17,23-26] (Table 1), six for outdoor air [27-32] (Table 2) and another three for personal exposure [33-35] (Table 3). Regarding study design, cohort and panel study design were the most commonly found followed by cross-sectional and case-control studies (n=6 and n=4, respectively).
Study population
With regards to population age, the largest amount of studies was carried out on schoolchildren, i.e. between 6 and 12 years old (60% of the total). A couple of studies were done on infants and another on preschool children (2-5 years old). Only one of the studies focused on adolescents (13-14 years old) and another study was carried out in all childhood ages (0-19 years old). Population size ranged considerably. Classifying sample size into three categories, low (up to 100 children), medium (100-500 children) and large (more than 500 children), approximately a third of studies would be at each category. Most of the studies were carried out in Europe (three in Germany, three in France, one in Spain and one in Portugal). Other studies were conducted in North America (three in USA (Alaska, Texas and Los Angeles) and one in Canada), one in Asia (South Korea), and one in Oceania (Australia).
Respiratory outcomes
The most often studied health problem was asthma (n=11), assessed by different outcomes. Asthma symptoms (e.g. those related to wheezing, cough -particularly dry cough at night-, shortness of breath or chest tightness) or asthma diagnosis were found in 7 articles. Asthma control questionnaire score (ACQ) and rescue medication were the outcomes studied in one paper each. Two remaining papers were case-control studies and they defined asthmatic cases as children having doctor-diagnosed asthma, having had wheezing in the past 12 months or having already taken medications for onset of asthma. The questionnaire was the most frequently used instrument to measure those outcomes (n=10). Of those, the one most widely used was that developed by the International Study of Asthma and Allergies in Childhood (ISAAC) (n=7) [36]. In one case, daily diaries were used by children to report asthma. Apart from asthma, lung function, pulmonary infections and bronchitis were studied in four, two and one paper, respectively. Wheezing was analyzed as an isolated symptom in three articles.
Benzene exposure assessment
The methodology for benzene exposure assessment was similar among the reports on indoor air pollution. In general, benzene concentrations were measured continuously and passively for 1, 2 or 4 weeks using different devices. Samplers in dwellings were located in living rooms in four studies. Diez et al. [26] did not specify the sampler location indoors.
Studies on outdoor compared to indoor exposure used a wider range of methods for benzene exposure assessment. Three studies used either passive or active samplers. Only half of the papers predicted levels by estimation methods (non-linear regression models taking into account traffic variables, land use regression models -LUR-, and dispersion models).
The three studies assessing personal exposure used passive samplers. However, each one assigned personal exposure using different methods. Smargiassi et al. [33] put the passive samplers in a backpack carried by children for 24 hours. Personal exposure was assigned by means of the mean level registered on the passive sampler for each child. Martins et al. [34] distributed passive samplers among outdoor and indoor spaces. Monitoring points were located over 4 weeks in the city center and school courtyards in order to assess outdoor air. The living rooms of houses or classrooms in schools were the locations for indoor air monitoring. Spatial levels were modeled by a dispersion model. Subsequently, personal exposure was assigned based on children timeactivity patterns reported by questionnaire. Finally, Hwang et al. [35] installed passive samplers near to the respiratory area of the children for 3 days to assess personal exposure. During this period, they also placed indoor (living room) and outdoor (veranda) samplers in the children’s house. They registered child time-activity patterns. However, the methodology for personal assignment is not stated in the text.
Benzene exposure levels
Benzene levels were expressed as different central tendency measures in the studies reviewed. Median benzene exposure levels ranged between 1.8 and 24.8 μg/m3 in indoor air (Table 1). In outdoor and personal exposure, mean benzene levels were in a range of 1.5-8.7 μg/m3 and 2.8-4.0 μg/m3, respectively (Tables 2 and 3).
Apart from benzene, other pollutants were assessed in the articles but results are not shown in this review. Excluding the study by Delfino et al. [30] in which two model pollutants were conducted, the rest of articles did not adjust associations by other air pollutants.
Associations
The associations between benzene exposure and respiratory outcomes were quantified and expressed mainly as odds ratio or as change in the outcome per increase of the pollutant. Excluding one study [17], most authors adjusted associations between exposures and respiratory outcomes by child sex and age, socio-demographic variables, family history of asthma or allergy, atopic status and other exposures (e.g. environmental tobacco smoke or redecoration activities in the dwellings).
Four out of the six papers on indoor air found statistically significant associations between benzene exposure and health outcomes, specifically, asthma symptoms [17,23], first diagnosis of asthma [25] and pulmonary infections [26]. Regarding outdoor exposure, almost all papers reported statistically significant relations between benzene exposure and respiratory health, explicitly, asthma [27,29-32], lung function [30,32] and bronchitis [32]. Aguilera et al. [28], found suggestive associations between benzene and pulmonary infections or wheezing, being stronger for exposure in the 2nd trimester of pregnancy. Studies on personal exposure to benzene, reported statistically significant associations between exposure and lung function [34], albeit not significant for asthma [35].
Benzene in indoor air
Three case-control studies on asthma assessing indoor air obtained different results for benzene exposure. Thus, a case-control study [23] carried out in adolescents from six French cities in 1999-2000 found a higher risk of asthma symptoms, specifically, woken up by a breathlessness crisis (OR[95%CI]: 10.10 [2.06-49.78]), related to a benzene exposure higher than 2.4 μg/m3. Urinary S-phenylmercapturic acid, a benzene metabolite considered as a benzene exposure biomarker, was higher in asthmatic children and was correlated with benzene exposure. Other asthma symptoms were not significantly related to benzene exposure. Conversely, another study conducted some years later (2003-2007) [24] in the same French region reported non statistically significant associations between benzene exposure (levels higher than 1.8 μg/m3) and asthma in schoolchildren aged 10-14 years old. The main limitation for the first study was its sample size (n=32 cases; n=31 controls). The second study almost duplicated the sample size (n=113; 63 living in urban and 51 in rural areas) and adjusted by additional variables, monitoring season and children location. The third case-control study [25] was conducted in preschool children (n=192) living in Perth (Australia). Authors reported a statistically significant increase in asthma risk (OR[95%CI]: 2.92[2.25-3.80] associated with every 10 μg/m3 increase in benzene exposure in child bedrooms. In two last case-control studies [24,25] asthma was associated with exposure to other VOCs (acetaldehyde, toluene and total VOCs) (data not shown).
The LARS cohort study in Leipzig (Germany) [26] assessed benzene exposure in dwellings during pregnancy. They found a statistically significant increase in pulmonary infections at 6 weeks of age (n=475) associated with an increase of 5.6 μg/m3 in benzene levels (OR[95%CI]: 2.40 [1.30-4.50]). Wheezing at first year of life was not related to prenatal exposure to benzene. Other VOCs were related with asthma and pulmonary infections. Despite the adjustment by other exposures, they neither adjusted by socioeconomic status nor family history of allergies. In a cross-sectional study [17], asthma was associated with high benzene exposure levels measured in living rooms of children between 0-19 years old (n=458; OR[95%CI]: 2.49 [1.22-5.07]; higher exposure than 28.7 μg/m3 in reference to lower exposure than 9.6 μg/ m3). The important limitations of this cross-sectional study were the study design and lack of adjustment for co-variables and confounders.
Benzene in outdoor air
In a panel study conducted by Zora et al. [27], passive samplers were installed outside two schools and individual exposure was assigned according to the nearest sampler. They found low levels of exposure, also for the school near to major roadways (1.5 μg/m3). No significant associations between benzene and other pollutants with an increase in ACQ score were found. However, an increase in 0.17 ACQ score units (95%CI: 0.04-0.31) was related with an increase in benzene levels of 0.8 μg/m3 among subjects inhaling corticosteroids daily. They did not adjust for socio-economic variables or other possible exposures. In the INMA Spanish cohort, Aguilera et al. [28], found an association between an increase in 1 μg/m3 of benzene exposure estimated in the second trimester of pregnancy and lower respiratory tract infections (LRTI) in a large sample of infants (n=2199). Delfino et al. [30] conducted a panel study on 21 asthmatic children aged between 10- 16 years old. They assigned individual benzene levels from nearer central site measurement the same day symptoms were reported. They found statistically significant associations between an increase in mean concentrations of benzene (5.7 μg/m3) and both asthma and lung function. But when other pollutants were added to the models, the statistically significant association was diluted. They did not adjust by socioeconomic status, other exposure or history of asthma or allergies.
Three cross-sectional studies on outdoor air exposure [29,31,32] were retrieved and asthma related outcomes were studied in all of them. Additionally, Hirsch et al. [32] studied bronchitis and lung function. In the later study, 182 grid-points for monitoring annual levels of benzene by means of active samplers were distributed over the area. No modeling methods were used to predict spatial levels in the study area. Residential and school exposure levels were assigned from the nearest sampler. An increase of 1 μg/m3 in both benzene exposures, residential and school, was associated with morning cough (more significant for non atopic children), bronchitis and asthma. In addition, residential exposure to benzene was associated with lung function. As part of phase II of the ISAAC project, Penard-Morand and Nicolai et al. [29,31] conducted similar studies in different countries (France and Germany, respectively) to assess outdoor exposure to benzene and asthma symptoms and obtain similar results. The first was conducted in 1999-2000 in schoolchildren (children between 9-11 years old, n=6683) within the French Six Cities Studies [29]. An increase of 2 μg/m3 in benzene exposure levels was associated with exercise-induced asthma, asthma current and asthma ever. Another study was conducted in 1995- 1996 in two groups of German schoolchildren (5-7 and 9-11 years old, n=7509) [31]. An increase of 1 μg/m3 in exposure levels was associated with current asthma, current wheeze, cough and current asthma when also considering ETS. Despite some similarities, the methodology used for benzene exposure assessment was different in the two articles (Table 2). While Pénard-Morand et al. [29] obtained annual mean concentrations of benzene from central sites measurements actively monitoring quality air, Nicolai et al. [31] monitored different levels by means of passive samplers located in 18 heavy traffic and 16 lowto- medium traffic points for 4 weeks. Additionally, Pénard-Morand et al. [29] spatially modeled benzene annual mean levels and exposure levels were predicted for each school address and Nicolai et al. [31] also modeled exposure levels but with a non-linear regression model and taking into account traffic variables. Individual assignment was done for residences. Hirsch et al. [32] monitoring annual levels of benzene by means of active samplers distributed in 182 grid-points over the area. No modeling methods were used to predict spatial levels in the study area. Residential and school exposure levels were assigned from the nearest sampler. An increase of 1 μg/m3 in both benzene exposures, residential and school, was associated with morning cough (more significant for non-atopic children), bronchitis and asthma. In addition, residential exposure to benzene was associated with lung function.
Personal exposure to benzene
There are some scientific evidences showing higher levels of personal exposure to air pollutants than those for indoor or outdoor exposure [22,37,38]. Nevertheless, this pattern was not obtained in the results of this review. Possible explanations are due to (1) the heterogeneity in methods assessing different types of exposures, and (2) spatial and temporal variability between studies. In general, personal exposure levels were lower than indoor exposure and similar for outdoor exposure. In a panel study conducted in asthmatic schoolchildren (n=72) from Montreal (Canada) no association between personal exposure to moderate levels of benzene and lung function-related outcomes was found [33]. Asthma association for schoolchildren (n=73) from Seoul (South Korea) was also not significant [35]. It should be pointed out that interpolation methods, as well as increased benzene level assessed, were not stated in this study. Only Martins et al. [34] reported a significant relationship for personal exposure to benzene. They carried out a study in wheezing children (n=52) from Viseu (Portugal), monitored indoor and outdoor benzene levels for 4 weeks, estimated levels spatially using dispersion model and assigned personal exposure based on time-activity patterns according to the estimations. They found significant associations between an increment in 10 μg/ m3 of benzene with all lung function-related outcomes assessed also when adjusting for confounding factors such as degree of dust mites infestation. However, no significant associations were obtained for wheezing or need of rescue medication. The very low sample size of the studies hindered detection of the potential respiratory effect of benzene exposure.
The literature reviewed shows the interest in studying the role played by exposure to benzene on respiratory problems in children. However, very few studies were found. Summing up globally the results from the studies selected, benzene exposure among children was associated with asthma [17,23,25,29-32], lung function [30,32,34], pulmonary infections [26,28] and bronchitis [32]. Overall findings in this literature review seem to indicate that benzene exposure is related with respiratory health in children and adolescents.
This review was focused on children up to 18 years old. We did not remove studies carried out on the adolescent population (13 to 18 years old) to increase the number of studies analyzing the relationship between benzene exposure and respiratory health. Some studies have analyzed associations between the presence of benzene sources in the dwellings [39-44] or living near to petrochemical industries [45-47] with respiratory health in children. They found significant associations between being exposed to these sources and suffering from wheezing episodes, asthma, obstructive bronchitis or impaired lung function. However, taking into account the fact that these sources are also sources for other pollutants as well as not providing us with reliable information about direct connection between benzene exposure and respiratory health, we excluded them from the review. We selected only papers that measure benzene levels quantitatively, in order to minimize misclassification exposure bias.
In general, benzene exposure levels in these studies were low compared with RfC for inhalation reported by IRIS (30 μg/m3) [18], however, they varied within a similar range to MRL recommended by ATSDR for acute and intermediate exposure terms (2.8 and 1.9 μg/m3) [48]). Benzene exposure levels indoors were higher than both personal and outdoor levels. Some additional studies have found a slightly different trend: personal exposure levels higher than indoor levels and this, in turn, higher than outdoor levels [22,37,38]. Comparisons between benzene exposure levels found in this review are untrustworthy due to three main reasons: methodological diversity, studies conducted in different years and geographical areas, and very scarce personal exposure studies. Comparisons should have been made with caution also when three measures, indoor, outdoor and personal exposure levels, were carried out in the studies. Taking into account boundary levels for ensuring human health established by European Regulation (5 μg/m3 [20]) and WHO guidelines (1.7 μg/m3 [21]), indoor exposure levels were moderate-high, outdoor levels were moderate-low and personal levels were moderate. In this case, it is also important to note that reference exposure levels were defined in different units (annual means) and methodologies (measured in outdoor ambient air by means of active samplers). Briefly, benzene exposure levels found were low, ranging in μg/m3 and higher for indoor air.
Major findings in heath respiratory effects were for indoor and outdoor air and were scarce for studies assessing personal exposure. The number of studies was very low. Related symptoms and problems seem to be related more to benzene exposure in indoor air than outdoor air, since magnitude associations were higher indoors. It is not due to higher levels of exposure being found indoors but to the higher levels of increase assessed in the association models (2.4-28.7 μg/m3 for indoor air versus 0.8-5.7 μg/m3 for outdoor air). There is no clear consistency between studies on the association between benzene exposure and different respiratory diseases in children [28,30,32-34], but, a more clear pattern between these contaminant and asthma has been found [17,23,25,27,29-32]. If a variety of studies using different designs and methodologies found significant associations with a health problem and air pollutant exposure the likelihood of making the same mistake is minimized. However, additional studies are needed to confirm this association.
Regarding time latency effects, most of the articles studied a chronic disease, asthma [24,25,29,31,32,35]. Nevertheless, some of them assess short-term effects outcomes related to exacerbation of asthma or severe asthma symptoms in case-control and panel control studies [23,27,30,34]. Panel studies, together with time-series studies, have been used widely to assess short-term effects of air pollution [49-51]. Individual availability of the data on exposure and heath are the major strengths for panel study designs. Additional panel studies in this review assessed lung function and wheezing as respiratory indices and symptoms that could be affected by short-term exposure to air pollution [30,32-34], but only in a couple of those the respiratory problems were negatively related to benzene exposure [30,32]. Apart from asthma, effects, bronchitis and pulmonary infections were related in the longterm with benzene exposure [28,43]. Despite the fact that the results varied considerably, findings of this review suggested adverse effects of benzene exposure in the short and long-term.
Studies reviewed used a wide range of approaches relying on study design, children’s age studied, outcomes analyzed, benzene exposure assessment methods and association measures used. This fact prevented comparisons from being made between results. Regarding the methodology used among the studies, by sampling exposure levels in different ways we could obtain different results (e.g., all types known of passive samplers are effective and reliable collectors under real-life conditions [52,53], but they could be different regarding uptake rates and detection limits [50]). Another limitation lies in the four crosssectional studies included. This type of studies, based on a punctual picture of the matter and usually with a single exposure measure, holds limitations to the etiologic study of a health problem and did not allow us to establish the temporality of exposures [54]. However, in one of the cross-sectional studies found [29], authors considered time of residence in the study area in the association analysis in order to minimize time exposure bias. The strength for including cross-sectional studies in this review was their statistical power due to their large sample size (ranging from 458 to 7509 individuals). Another deficiency of some of the studies selected rests on the lack of some adjusting variables. One of these reports [17] did not include any covariables in the association models. More than half of the studies did not adjust by socio-demographic status. Some studies neither adjusted by other exposures or familial history of allergies [27,30,32,35,43].
Since different methodologies were applied in the studies and a low number of studies were found, the evidences are scarce and inconclusive. Additional research on this topic is needed to broaden knowledge on the relationship between benzene and respiratory health in children. In our opinion, more studies on personal exposure assessment would be crucial, as these measurements are the most reliable to determine real exposure to air pollutants. Besides, more studies should be addressed at improving exposure assessment considering time-activity patterns as well as the use of prospective designs. Additional studies based on multicenter projects using common methodology are needed. Some examples of these multicenter studies could be ESCAPE [55], HELIX [56], ENRIECCO, CHICCOS, GA2LEN, MeDALL [57] in Europe, National Children Study in the United States or ISAAC [36,58] and ICAPPO [59] worldwide projects. Finally, it is important to consider in the analyses adjusting factors related with other exposures (tobacco smoke, combustion sources in the household and other variables about lifestyles [13]), social factors [60-63], annual variability in VOC levels [64],preterm birth and low birth weight [65,66].
In conclusion, the effect of benzene exposure on children’s respiratory health at usual current levels has still not been confirmed. However, some considerations for preventing hazards from benzene exposure could be recommended [67]. In indoor air, it is important to maintain high rates of ventilation at home during benzene-emitting activities (e.g. redecorating, painting works) or avoiding tobacco smoke. In outdoor air, a useful recommendation included using ecologic transport (e.g. bicycle, public transport or electric cars). All these recommendations are of course also good for improving air quality in general. Further research is needed to broaden knowledge on the effects of benzene on respiratory health during childhood.
This work was supported by grants from the Health Institute Carlos III (PI13/02032, PI12/00610, PI11/02591). The first author wants to thank to Dr. Maria-Jose Lopez-Espinosa for writing assistance.