Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2015) Volume 5, Issue 2
A 68 years old woman was admitted for abdominal pain, acute pancreatitis complicated with peripancreatic fluid collections. She has received steroid treatment during 12 months for pulmonary fibrosis, 60 mg/day Prednisone in the last months. Three weeks before her admission calcitonin treatment was introduced for osteoporotic vertebral fracture. The pancreatitis followed a benign clinical course; oral diet was reintroduced in two weeks. Some days later, calcitonin treatment was also reinitiated, followed by a recurrence of abdominal pain on the third day, accompanied by a second increase in blood pancreatic enzymes. On the fourth week of the acute exacerbation of pancreatitis the patient presented fever: bacterial infection of the demarcated fluid collections was confirmed by fine needle aspiration. The infected pseudocysts were drained percutaneously, guided by CT scan, with favorable evolution, almost complete disappearence of them in two weeks. The patient died three months later, as a consequence of her pulmonary disease. The acute pancreatitis developed in the second week after initiation of calcitonin treatment and an acute recurrence was observed after a three-day “accidental rechallenge”. No other known etiology of acute pancreatitis was detected. We conclude that calcitonin should be considered as a probable cause of a drug-induced pancreatitis
<Keywords: Acute pancreatitis, Calcitonin, Rechallenge, Infected pseudocyst
Several drugs are supposed to produce acute pancreatitis, but a clearcut cause-effect relationship is only rarely demonstrated. Pancreatitisis a very rare side effect of the drugs; the pathomechanism is generally unknown (or sometimes partially known) even if it is considered clearly proven. In addition, a rechallenge is rarely acceptable for obvious ethical reasons. In consequence, our knowledge comes mostly from anecdotal case-reports. However, the accumulation of these individual reports gave the possibility to identify several drugs, which can induce an acute pancreatitis with variable probability and frequency, sometimes acting as cofactor. They were classified in three categories on the base of the probability of their causative role: I. definite, II. probable, and III possible association with pancreatitis [1]. Later on, thisclassificationwas modified and now, four classes of drugs are accepted, on the base of the literature data: being the strongest relation if pancreatitis after a consistent latency period was published at least in one case report, with evidence of a positive rechallenge [2-4], and exclusion of other causes of AP.
In the present paper we report the case of an acute pancreatitis observed after a three-week treatment with salmon calcitonin and a second relapse after an “accidental rechallenge”.
A 68 years old woman was admitted for a colicky abdominal pain accompanied by elevated amylase (476 U/l –normal <100) and lipase (284 U/l, normal <60) serum level. She had severe respiratory problems for several years. Pulmonary biopsy was performed 15 months earlier and pulmonary fibrosis was confirmed. Steroid treatment was immediately initiated, with oral Prednisone therapy in a dose of 1 mg/kg/day (60 mg) in the first three months. The gradual decrease in the dose to 40 mg/day was followed by worsening of her disease, thus the steroid-dose was increased again and continued with some minor variations. One year later, a severe osteoporosis developed complicated by a painful destruction of the vertebral body L5. Calcitonin treatment (nasal spray, 200 IU/day) was introduced. The patient presented moderate abdominal pain from the second week of the treatment. Finally, worsening in her complaints, vomiting made necessary her hospital admission. Acute pancreatitis was the clinical diagnosis, confirmed by elevated amylase and lipase and by CAT-scan, which revealed an enlargement of the pancreas accompanied by multiples peripancreatic fluid collections, corresponding to an acute pancreatitis in evolution.
The abdominal pain diminished quickly with conventional treatment (nil by mouth, intravenous hydration). Enteral nutrition via nasojejunal feeding tube was followed by a well-tolerated oral diet from the tenth day of hospitalization. Calcitonin treatment was reintroduced from the 17-th day, followed by recurrence of abdominal pain on the 3-d day. Calcitonin was immediately discontinued, further dietary restrictions were introduced, but the pain progressed in intensity in the next few days and was accompanied by a moderate second elevation of serum amylase (198 U/l), lipase (248 U/l) and CRP (76 mg/l). The clinical symptoms were controlled in 3 days without additional variations in the therapy, amylase and lipase activity returned into normal range (Figure 1), CRP diminished again.
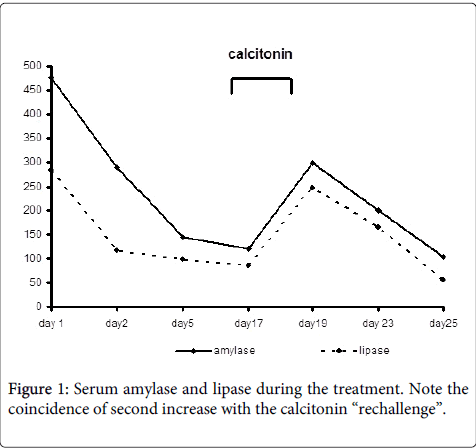
Figure 1: Serum amylase and lipase during the treatment. Note the coincidence of second increase with the calcitonin “rechallenge”.
The patient was discharged, and hospitalized again two weeks later for fever, respiratory difficulty. The fever persisted in spite of antibiotic treatment and ameliorated respiratory symptoms, CPR value was highly elevated. Infection of pseudocyst fluid was demonstrated: Escherichia coli were detected in the cyst content by fine needle aspiration. Percutaneous drainage of the two mayor peripancreatic collections (Figure 2a) was performed guided by CAT-scan, and enteral nutrition was reinitiated via a long nasojejunal feeding tube.
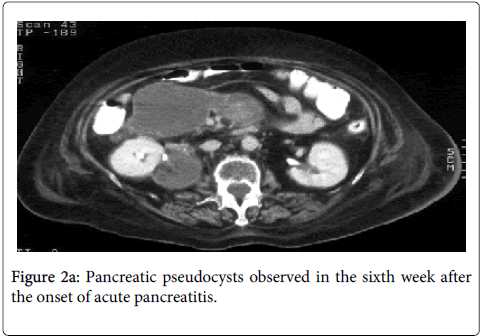
Figure 2a: Pancreatic pseudocysts observed in the sixth week after the onset of acute pancreatitis.
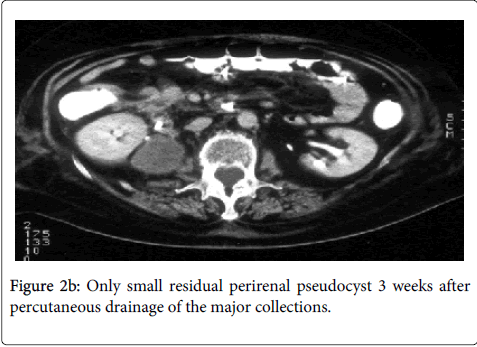
Figure 2b: Only small residual perirenal pseudocyst 3 weeks after percutaneous drainage of the major collections.
Finally the patient was stabilized and discharged with good tolerance to the oral diet. At the last tomographic control only one small perirenal pseudocyst was seen (Figure 2b).
In the next some months she had no abdominal complaints, but presented recurrent episodes of cardiac arrhythmia, respiratory insufficiency, and finally she died with the complications of her pulmonary disease.
Calcitonin administered as intramuscular injection, nasal spray or suppositories, is one of the best possibilities to treat osteoporosis of different etiology [5,6]. Later on, its use has become less important, but calcitonin still continues to be one of the widely accepted possibilities of the treatment [7]. A significant decrease in spontaneous fractures was described during one year calcitonin treatment when compared to placebo [5]. Its beneficial effect was also demonstrated in asthmatic patients requiring chronic steroid treatment [5]. The frequency of side effects was lower if it was administered as nasal spray [8]. The side effects published include allergic reactions, mainly cutaneous manifestations, rush, but a case of a severe anaphylactic reaction was also reported [9]. Abdominal complaints without precise organ-damage are relatively common amongst the known side effects. However, only one abstract (from the former group of one of the authors, Z.B.) suggested the possibility that Osteochin®, a drug which acts via mobilization of endogenous calcitonin, could produce mild pancreatitis in two patients [10]. We did not find any other publication which would suggest the possibility of a calcitonin-induced pancreatitis. On the contrary, calcitonin was proposed for treatment of acute pancreatitis [11,12], although later on, lack of its beneficial effect was demonstrated [13] but without observing pancreatic damage due to calcitonin.
In our present case, calcitonin was initiated to treat steroid-induced osteoporosis, painful spinal vertebral collapse, with a rapid, good clinical response. Acute pancreatitis developed after three weeks of calcitonin treatment, and it was initially considered as idiopathic. Biliary etiology was excluded by normal hepatic function test and abdominal ultrasound. The role of steroid treatment was unlikely, since the acute pancreatitis occurred after about 15 months of steroid treatment without any significant variation in the steroid-dose. In addition, steroids are not unequivocally considered as a possible cause of pancreatitis [14]. The acute pancreatitis was initially considered as idiopathic. Calcitonin was thus reintroduced after a benign clinical course, good tolerance to the oral nutrition, in the third week of the pancreatitis. At this time, only three days of treatment reproduced similar clinical symptoms accompanied by a second increase in blood level of pancreatic enzymes. This second administration fulfilled the criteria of a rechallenge, although far to be intentional. We have no explanation, how calcitonin could produce an acute pancreatitis. An allergic reaction could have been hypothesised on the basis of the fact that the second administration produced a bout after a considerably shorter period (3 days vs. 2-3 weeks). However, we did not observe any other manifestation of a supposed allergic reaction, and the presence of the pseudocysts also could explain this increased sensibility of the pancreas. Hypercalcemia is one of the possible causes of acute pancreatitis, some drugs produce acute pancreatitis acting via modification of serum calcium level. One could speculate that when calcitonin decreases serum calcium level [15], could modify the calcium concentration in the pancreatic tissue, which in turn could trigger the autodigestive chain reaction.
Although the pathomechanism is not clear it seems quite probable that calcitonin administration was responsible for the acute pancreatitis in our patient. Pancreatitis developed after a short calcitonin-treatment, other likely causes were not demonstrated, the clinical symptoms and laboratory alterations ameliorated after discontinuing the calcitonin and finally, an “accidental rechallenge” reproduced a second relapse of pancreatitis.
We suggest adding calcitonin to the long list of drugs which can induce pancreatitis with a certain probability, at least as a cofactor, probably in the second category of drugs (i.e. probable association). However, our case fulfills the criteria class I/a: probable cause effect relation with temporary coincidence with positive rechallenge. As far as we know, our case is the first to observe pancreatitis as probable side effect of calcitonin treatment. We recommend determining serum-level of pancreatic enzymes in all patients presenting abdominal complaints during calcitonin treatment. An abdominal CT scan should be performed if these enzymes are even slightly increased.