Angiology: Open Access
Open Access
ISSN: 2329-9495
![]() +44 1478 350008
+44 1478 350008
ISSN: 2329-9495
![]() +44 1478 350008
+44 1478 350008
Research Article - (2018) Volume 6, Issue 1
Purpose: To evaluate the presentation, clinical course and outcome of carotid-cavernous fistula (CCF) cases with endovascular treatment in our institution during the last 10 years.
Methods: It is a prospective, protocol- based study of 45 consecutive cases who had presented in our Neuro-ophthalmology department from 2005 to 2015. Detailed history and complete neuro-ophthalmic examination along with relevant investigations and treatment was done. The patients were followed up immediately after the procedure and at three monthly intervals for one year and then yearly.
Results: In our study the age range is from 3 to 63 years. Of the total 45 cases 42 had direct CCF while 3 cases were of dural CCF . Orbital and neuro-ophthalmological symptoms and signs were most common clinical presentation at diagnosis. All the cases but one responded well to transfemoral balloon/coil embolization in our institute Conclusion: CCF mostly have classical presentation but few cases can cause a diagnostic dilemma and so the ophthalmologist have to be observant about the disease. Early diagnosis results into least morbidity. Timely intervention with endovascular coiling results in successful closure of the fistula .
Keywords: Carotid-cavernous fistula; Neuro-ophthalmology; Endovascular procedure; Visual Loss; Endovascular coiling
Carotid cavernous fistula (CCF) is an abnormal communication between the cavernous sinus and the carotid arterial system. A large number of cases of Direct CCF are caused by rupture of preexisting aneurysm of cavernous segment of internal carotid artery. In few cases the aneurysms have been previously diagnosed due to its mass effect on the structures of cavernous sinus whereas in other patients CCF is the first sign of aneurysm. We encountered two cases in which CCF was diagnosed first and subsequently in these patients aneurysms were detected. Our aim is to evaluate the presentation, clinical course and outcome of carotid-cavernous fistula (CCF) cases with endovascular treatment in our institution during the last 10 years.
It is a prospective, protocol- based study. We have 45 consecutive cases who presented in our Neuro-ophthalmology outdoor patient department from 2005 to 2015. Detailed history and complete neuroophthalmic examination was carried out for all cases. Diagnosis was made on the basis of clinical suspicion, radiological evidence (Computerized Tomography / Magnetic resonance imaging or both) and positive angiographic findings. Follow up examination was done immediately after the procedure and at three monthly intervals for one year and then yearly.
The procedure is performed by a trained radiologist in the department of interventional radiology. The procedure was carried out under General anesthesia. The vascular access is through the right femoral artery. In most cases a diagnostic cranial angiogram is done before planning a therapeutic procedure, diagnostic angiogram is done with the help of 5 F diagnostic catheter and detailed anatomy is evaluated which includes the identification of the site and size of rent in ICA (Internal Carotid Artery) and also the cross-flow adequacy is judged just in case ICA need to be scarified during therapeutic procedure. Therapeutic procedure is done using 6 or 7 F guiding catheters, through which continuous heparinized saline flush is connected, using micro catheter the fistula site and the cavernous sinus is cannulated and using multiple coils or detachable balloon it is sealed off. Post procedure low molecular weight heparin is given for few days.
In our study the age range is from 3 to 63 years (mean, 27.11). There were 34 males and 21 females. The interval from onset to presentation ranged from 5 days to 15 years. History of trauma was positive in 42 of 45 cases (93.3%). Trauma was in the form of fall in 15 cases while 27 cases had road traffic accident. 3 cases had no history of trauma and were of indirect type. Orbital and neuro‐ophthalmic symptoms were ipsilateral to the fistula in 40 patients, bilateral in 3 and contra lateral to the fistula in 2 patients.
Of the total 45 cases 42 had direct CCF while 3 cases were of dural CCF. Orbita and neuro-ophthalmological symptoms and signs were most common clinical presentation at diagnosis (Figure 1) and (Table 1).
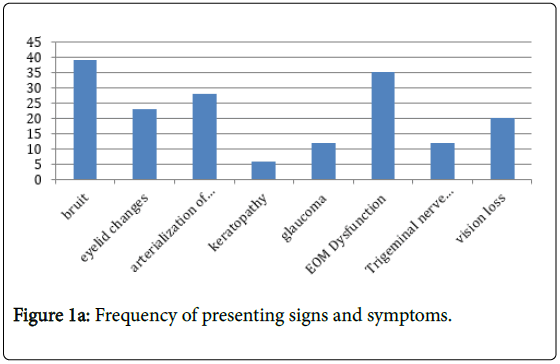
Figure 1a: Frequency of presenting signs and symptoms.
| No. of Cases | 45 |
|---|---|
| Proptosis | 0.933 |
| EOM Dysfunction | 0.777 |
| Glaucoma | 0.266 |
| Visual loss | 0.444 |
| Eyelid Changes | 0.511 |
| Keratopathy | 0.133 |
| Traumatic optic atrophy | 0.177 |
Table 1: Frequency of presenting signs and symptoms.
Visual Loss in CCF was reversible in 12 of 20 cases who had optic nerve dysfunction either due to ischemia or compression of the optic nerve or chiasma by a distended cavernous sinus. Irreversible vision loss was due to traumatic optic neuropathy in 8 of our cases.
Endovascular embolization was undertaken in 42 of 45 cases. Three cases showed spontaneous recovery which were of indirect type. One of our patients had superior ophthalmic vein thrombosis after procedure which subsequently resolved while one case had developed ocular ischemic syndrome.
All the cases responded well to transfemoral balloon/coil embolization in our institute. Of the one failed case, subsequent craniotomy with clipping of Internal Carotid Artery proximal to the origin of ophthalmic artery was undertaken.
Once the fistula was successfully closed the symptoms and signs resolved or improved. The extent and rate of improvement of signs and symptoms were related to their severity and length of time the fistula was present.
All these patients were followed up to one year post procedure. 50% of these patients have been followed up for a period of 4 years.
Bruit and congestion disappears immediately after the procedure. Also, intraocular pressure returned to normal on the same day post procedure while resolution of chemosis and proptosis occurred within few days to weeks.
None of our patient had recurrence. Timely intervention with endovascular treatment of CCF is the procedure of choice and is quite effective.
CCF mostly have classical presentation but few cases can cause a diagnostic problem and so the ophthalmologist have to be vigilant about the disease and in diagnosing these cases. Early diagnosis resulted into least morbidity. Timely intervention with endovascular coiling is the key to success.
Case 1
A 63-year female presented with tortuous, dilated conjunctival vessels and mild chemosis, complete ptosis on left side following trauma. Clinical diagnosis of CCF was confirmed by DSA. The, patient underwent endovascular embolisation at our institute. Immediate postoperative period was uneventful, but the patient developed worsening of features on 2ndpost-op day. There was increase in proptosis and congestive signs. Prominence of Superior ophthalmic vein (SOV) was noted suggestive of SOV (Figure 2a and 2b). Thrombosis which was confirmed on imaging. SOV Thrombosis is a known complication of endovascular procedures. The patient was treated with anticoagulants and on subsequent visits the patient recovered completely.

Figure 2a: Figure 2a shows preoperative image of the patient with prominent superior ophthalmic vein.

Figure 2b: Figure2b shows postoperative image of the patient with prominent superior ophthalmic vein.
Case 2
A 60 years old female had sustained a road traffic accident following which she developed 3rd and 6th nerve palsy with minimal episcleral congestion in right eye for last 3 weeks. Applanation tonometry showed intraocular pressure of 28 mm hg RE and 12 mm LE. Exophthalmometry revealed 1mm proptosis in the right eye. Fundus examination revealed disc cupping 0.6 mm in RE and 0.3 mm in LE. CCF was suspected and was confirmed by DSA. This case reveals that proptosis may not always be the presenting feature of CCF especially in posteriorly draining cases. Glaucoma in CCF may be associated with early cupping. Raised episcleral venous pressure with concurrent ischemia is the major reason. The patient then underwent coiling procedure. Post treatment the ocular motility has recovered and intraocular pressure recorded on last follow up was 12 mm hg in both eyes.
Case 3
A middle aged female presented to us with pulsatile proptosis and lateral rectus palsy in LE × 15 days. There was no history of trauma. Her visual acuity (BCVA) RE and LE was 20/30. Exophthalmometry displayed 2 mm proptosis in left eye without any signs of congestion. DSA revealed left CCF from rupture of Left ICA aneurysm (Figure 3). Embolization was planned but patient showed spontaneous recovery and DSA showed closure of fistula before the procedure. This case suggests that CCF may develop following rupture of intracavernous carotid aneurysm.
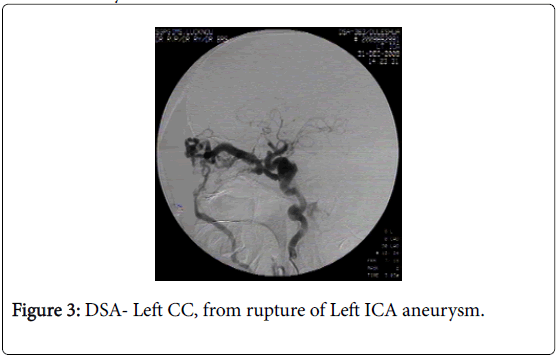
Figure 3: DSA- Left CC, from rupture of Left ICA aneurysm.
Case 4
A 35 years old female presented to us with acute onset left sided proptosis and chemosis following road traffic accident 4 days back. DSA was done which revealed CCF. Patient was advised to undergo coiling procedure. Due to financial constraints treatment was deferred. Three months later patient presented with enophthalmos, ptosis, extraocular muscle palsy and mild right frontal headache.If the treatment is delayed then the involved eye may become phthisical Hence prompt management is the key to success.
Carotid cavernous fistula (CCF) is an abnormal communication between the cavernous sinus and the carotid arterial system. A CCF can be due to a direct connection between the cavernous segment of the internal carotid artery and the cavernous sinus, or a communication between the cavernous sinus, and one or more meningeal branches of the internal carotid artery, external carotid artery or both. These fistulas may be categorized by etiology (spontaneous or traumatic) or anatomy (direct and dural). The dural fistulas usually have low rates of arterial blood flow and may be difficult to diagnose without angiography while direct fistulas are of high flow type and present with conspicuous symptoms [1].
A sizable number of cases of Direct CCF are caused by rupture of preexisting aneurysm of cavernous segment of internal carotid artery. In few cases the aneurysms have been previously diagnosed due to its mass effect on the structures of cavernous sinus whereas in other patients CCF is the first sign of aneurysm [2]. We observed two cases in which CCF was diagnosed first and subsequently in these patients aneurysms were detected.
The clinical presentation of CCFs is varied according to the anatomy, hemodynamics and size of the CCF. Presenting symptoms and signs are related to the angiographic drainage of CCFs. Posterior draining fistulas may cause isolated ocular motor nerve paresis and proptosis may not always be the presenting feature of CCF as in our second case who presented with 3rd and 6th nerve palsy with minimal episcleral congestion in the involved eye.
The most severe ocular manifestations occur in patients with anterior redirection of arterial blood through normal orbital venous channels. These expressions are caused by combination of diminished arterial flow to the cranial nerves within the cavernous sinus, arterial and venous circulation stasis within orbit and an increased episcleral and orbital venous pressure [3].
Patients with CCF may initially present to an ophthalmologist with decreased vision, conjunctival chemosis, external ophthalmoplegia and proptosis. Corkscrew blood vessels in association with conjunctival chemosis, proptosis and bruit should raise the possibility of a diagnosis of arteriovenous fistula especially if the patient has history of trauma [4].
Patients with any associated visual impairment or ocular conditions, such as glaucoma, need to be identified and treated. Secondary glaucoma is a frequently observed ocular manifestation of CCF, and closure of the fistula is the primary condition required for favourable intraocular pressure (IOP) control [5]. We had 12 cases who had raised IOP at the time of presentation. We had put these patients on topical antiglaucoma medications and subsequently after embolization process the intraocular pressure returned to normal in all the cases.
Although glaucoma is usually associated with increased episcleral venous pressure, yet it may be due to iris neovascularization as a result of retinal ischemia [6].
Glaucoma in CCF may be associated with early cupping as seen in 3 of our cases although the duration of the disease was short. Raised episcleral venous pressure with concurrent ischemia is the major reason.
Venous and arterial stasis may result in decreased ocular and retinal perfusion. Retinal and choroidal changes include venous dilatation, retinal hemorrhage, central retinal vein occlusion, central retinal artery occlusion, cotton wool spots and even serious retinal detachment. In addition, there may be anterior segment ischemia due to decreased perfusion to intra-cavernous sinus cranial nerves, resulting in ophthalmoplegia and diplopia mimicking Graves' ophthalmopathy [7]. The visual loss may be secondary to corneal, retinal or optic nerve changes or may result from the accompanying glaucoma.
Radiological features may be helpful in confirming the diagnosis and determining possible intervention. Suspicious cases should undergo Magnetic Resonance Angiography or Computerized Tomography Angiography. Duplex carotid ultrasonography can be used to detect the fistula and determine its flow rate. The ultimate diagnostic test for direct carotid-cavernous sinus fistulas is cerebral arteriography of both the internal and external carotid arteries.
Ophthalmologist may be the first person to encounter these cases and hence the clinician should be vigilant to diagnose these cases [8].
Based on patient's signs and symptoms, timely intervention is mandatory to prevent morbidity or mortality as in one of our patient who could not get the treatment on time and later on when she followed up after few months her affected eye had become pthisical. Misdiagnosis of CCFs is frequent due to its diverse clinical manifestations. CCFs should be suspected in patients with refractory red eyes, intraocular pressure elevation, proptosis and/or ophthalmoplegia, and a meticulous history-taking, thorough physical examination, and adequate imaging may minimize the misdiagnosis.
Some of the differential diagnoses for CCF include vascular lesions such as arteriovenous malformation and cavernous sinus thrombosis, cavernous sinus tumors, orbital tumors, skull base tumors and mucocele [9]. Infections such as orbital cellulitis, mucormycosis and tuberculosis may also present as CCF. Thyroid eye disease; orbital pseudotumor; and orbital vasculitis resulting from Wegener's granulomatosis, polyarteritis nodosa, intracranial sarcoidosis and Tolosa-Hunt syndrome may mimic CCF [7].
Most CCFs are not life threatening, but the involved eye is at risk. Main indications for treatment include glaucoma, diplopia, intolerable bruit or headache, and severe proptosis causing exposure keratopathy. Spontaneous closure from thrombosis of cavernous sinus is unlikely (especially those that occur after trauma or in high flow fistulas). Dural fistulas (Indirect type) may undergo spontaneous closure, especially if the feeding arteries are very small. We had two cases that showed spontaneous closure.
The optimum treatment of a direct CCF is the closure of abnormal arterivenous communication with preservation of the internal carotid patency. Endovascular closure is practiced by embolization using a variety of agents like platinum coils and detachable balloons.
Manual compression of the ipsilateral carotid artery multiple times a day may prove useful in indirect type CCF with reported closure rate of 20-60%. Radiosurgery is also an option but is not of much use in direct type. In indirect dural type of CCF it might prove useful with a time delay of 8-22 months.
Regardless of the treatment used, the dural fistula can be closed completely in most cases, resulting in restoration of normal orbital and intracranial blood flow [10]. In rare cases transvenous approach is needed where reaching the fistula via arterial route is not possible, this mostly happens in indirect type of CCF.
Complications may include transient worsening of ocular signs especially proptosis, ophthalmoparesis and pain. We did not encounter any major complication in our case series. One of our patients had Superior Ophthalmic Vein Thrombosis which was confirmed on imaging. SOV Thrombosis is a known complication of endovascular procedures where the superior ophthalmic vein is enlarged before the treatment procedure.
The ophthalmologist should be able to monitor the course of the disease, including extraocular changes, fundus changes and IOP measurements. In addition, the ophthalmologist should participate in the selection of patient who may be candidates for embolization treatment and possibly assist at surgery by helping isolate the ophthalmic vein at the time of surgery.
These patients are followed up by ophthalmologists for persistence of any of their symptoms and continuous management if indicated.