Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Case Report - (2018) Volume 6, Issue 4
Subclavian artery aneurysms account for fewer than 1% of peripheral aneurysms, and spontaneous ruptured subclavian artery aneurysm is even rarer. We describe a 17-year-old man with spontaneous ruptured right subclavian artery aneurysm, which we successfully treated by endovascular repair.
Keywords: Subclavian artery aneurysm; Endovascular repair
Subclavian artery aneurysm (SAA) is rare and when it occurs, it is usually asymptomatic, yet it can be life-threatening when it ruptures and haemorrhages. Several treatments for SAA exist and their selection depends on patient status and surgeon experience. Usually an endovascular approach is attempted before more invasive open subclavian artery revascularization [1]. Endovascular treatment is increasingly used to treat subclavian artery aneurysm with favourable anatomy, especially in those patients who are not candidates for surgery [2]. Here we describe a 17-year-old man with spontaneous ruptured right SAA who was treated successfully with an endovascular stent graft. Follow-up at six months showed normal blood test results and good patency of the right subclavian artery, with no leakage.
A 17-year-old-male presented at the emergency department of our hospital with complaints of acute pain in the right shoulder and back during jogging. The patient had no history of trauma. The patient had normal vital signs, and there was no discomfort in the right upper limb. However, a pulsatile supraclavicular mass was detected, which was intensely painful to the touch. Computed tomography angiography revealed right subclavian artery pseudoaneurysms with peripheral hematoma formation and chronic inflammation in the upper lobe of both lungs (Figure 1). No other aneurysms were found. Since the patient was anaemic and symptomatic on the right shoulder and back, we decided to repair the ruptured right subclavian artery aneurysm to prevent it from worsening.
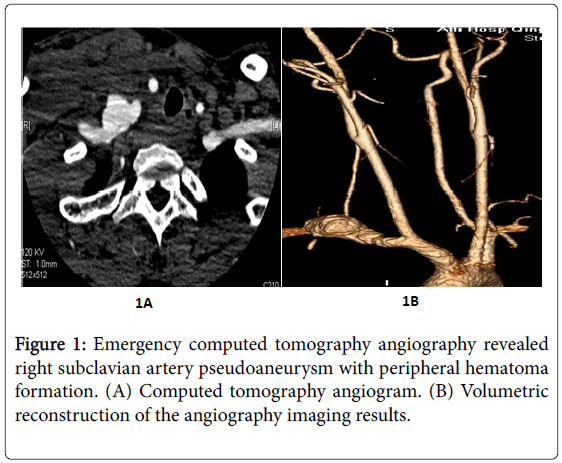
Figure 1: Emergency computed tomography angiography revealed right subclavian artery pseudoaneurysm with peripheral hematoma formation. (A) Computed tomography angiogram. (B) Volumetric reconstruction of the angiography imaging results.
The patient was offered endovascular stent grafting as an emergency operation, which solved the bleeding. During diagnostic angiography via the right common femoral artery, we discovered that the right vertebral artery was affected (Figure 2), so we blocked it. Post-stenting angiography showed that the stent was in good position, and the aneurysm did not develop (Figure 3).
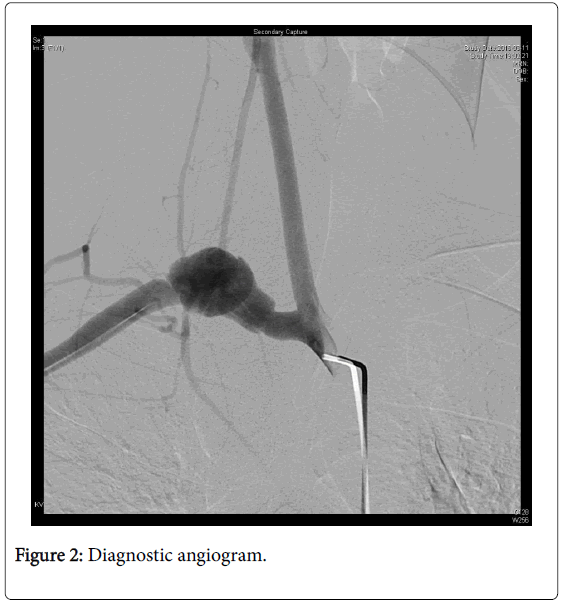
Figure 2: Diagnostic angiogram.
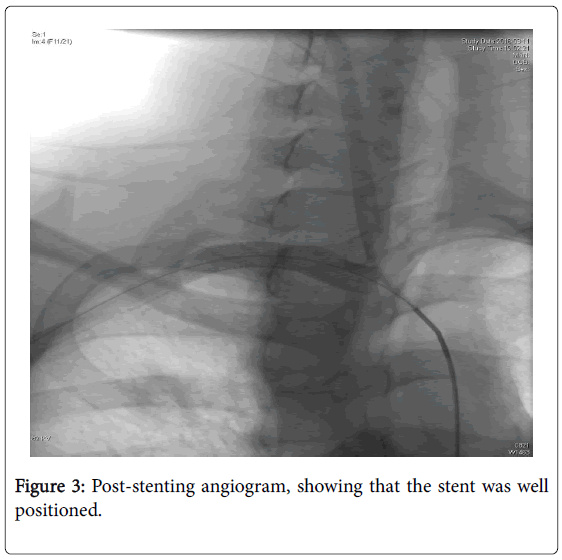
Figure 3: Post-stenting angiogram, showing that the stent was well positioned.
After the surgery, assays of procalcitonin, C-reactive protein, erythrocyte sedimentation rate (ESR), blood culture and rheumatic correlation gave no remarkable findings. Within three days after surgery, the patient developed fever, which resolved and then recurred. During both periods of fever, sputum culture tests were positive for Klebsiella pneumoniae. After checking drug sensitivity, the patient was given Sulperazone for 7 days. The patient was discharged with aspirin therapy. Follow-up at six months after surgery using computed tomography angiography showed that the stent remained well positioned with no endoleakage, and that the peripheral hematoma had disappeared (Figure 4). Follow-up of the patient continues.
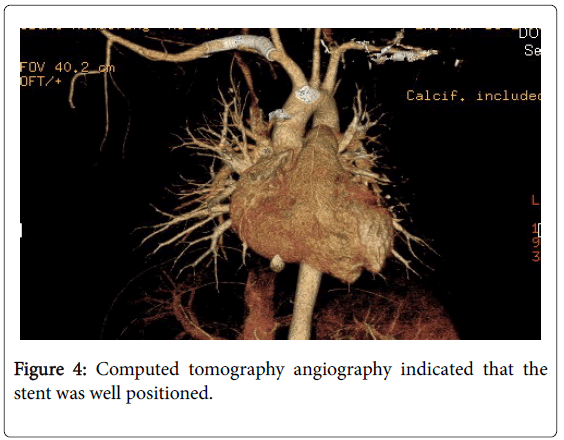
Figure 4: Computed tomography angiography indicated that the stent was well positioned.
The incidence of subclavicular aneurysm is quite rare: they account for fewer than 1% of peripheral aneurysms [3], and a case series at a large medical center in the US reported 31 patients in 20 years [4]. This rare disorder may be caused by arteriosclerosis, trauma, fibrodysplastic disease, degenerative connective tissue disorders, cervical ribs in association with thoracic outlet syndrome [5], syphilis, orrare congenital conditions such as Turner’s or Marfan syndromes [6]. In some cases, the likely cause of aneurysm cannot be identified [7]. We were unable to determine the cause of spontaneous ruptured right subclavian artery, even after surgery. Two positive sputum culture results for Klebsiella pneumonia lead us to suspect that the cause was infection. Consistent with this idea, the combination of antiinflammation treatment and endovascular treatment with a stent graft improved the patient's condition substantially.
An SAA is usually asymptomatic, presenting with a pulsatile supraclavicular mass. According to an analysis, pulsating mass and hematoma are the most common signs (27.5%), while any kind of neurological deficit of the arm was the second most common complaint (16.5%) [8]. Treatments include distal embolizations, thrombosis, compression of adjacent structures, or rupture [9]. Resection of the aneurysm and reconstruction by prosthetic graft or endovascular therapy has also been reported [10].
The conventional treatment for ruptured subclavian aneurysms is open surgical repair [11]. Endovascular treatment with stent grafting is considered less invasive and to confer lower risk than surgical treatment [12]. Open surgery and endovascular repair complement each other and each has its advantages. In our patient, the proximal subclavian aneurysm was located near the pleural cavity and difficult to access. In this situation, open surgery could easily cause excessive trauma. Therefore, we preferred to perform endovascular repair involving coil embolization and endovascular graft exclusion. We were careful to ensure intracranial blood supply and avoid severe ischemia in the after brain when the vertebral artery was isolated. Computed tomography angiography revealed a slender right vertebral artery and a dominant left vertebral artery. This made isolation of the right vertebral artery inevitable when we excluded the ruptured right subclavian aneurysm. After surgery, the patient did not show any symptoms of cerebral ischemia, and results were unremarkable for assays of procalcitonin, C-reactive protein, erythrocyte sedimentation rate (ESR) and rheumatic correlation.
Patients with inflammatory aneurysm should be given hormone or anti-inflammatory therapy before surgery to prevent vascular inflammation. In the case of our patient, he was in acute pain and required emergency intervention, so we initially focused on saving his life. Anti-inflammatory therapy was given after the sputum culture results came out.
Follow-up at six months showed that our patient was in good condition, and we will continue to monitor him. Perhaps through analysis of more cases, it will be possible to determine whether surgery caused the infection in our patient.
We successfully treated a patient with spontaneous ruptured right SAA using one stent graft without incurring endoleakage or reducing cerebral blood flow. This minimally invasive operation can avoid the technical issues and complications associated with surgical or hybrid procedures. SAA in case of spontaneous rupture is rare, and more case reports are needed to establish its characteristic features.