Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2014) Volume 3, Issue 2
Background: Papillary thyroid carcinoma (PTC) exhibits a high index of cervical lymphatic dissemination. Methods: Retrospective study of 101 cases of PTC subjected to total thyroidectomy associated with cervical lymph node dissection. Results: The incidence of neck metastasis was 50.5%, and all the metastases wereipsilateral to the primary tumor. Although the participants with metastases (N+) hadmore dissected lymph nodes than the group without metastases (p = 0.01), the lymphnode size was not a determinant of malignancy (p=0.34). Uni and multivariate analyses showed tumor size ≥ 1.0 cm, angiolymphatic invasion, and multicentric diseases were associated with lymphatic dissemination (p < 0.05). Conclusions: Factors predictive of cervical lymph node metastasis were tumor size ≥ 1.0cm, multicentric disease and angiolymphatic invasion. All the metastases wereipsilateral to the primary tumor. Lymph node size was not a reliable predictor of thepresence or absence of metastasis.
<Keywords: Papillary thyroid carcinoma, Lymph node, Metastasis,Pattern, Predictive factors
Thyroid carcinoma is the most common endocrine neoplasm, corresponding to 95.0% of them, and they make up 2.0% of all malignant tumors. Thyroid carcinoma exhibits a high index of dissemination to the cervical lymph nodes [1]. Neck ultrasound identifies lymph node metastases in 20-30% of cases, especially in the areas closest to the thyroid gland, where their frequency is higher. However, those percentages correspond to fewer than half of the patients with lymph node metastasis [2]. Although the presence of neck metastases increases the rate of local recurrence, the risks of elective lymph node dissection should be assessed relative to its potential benefits, such as reduction of the number of reoperations. Thus, the indication for elective lymph node dissection is controversial for individuals with noclinically manifest metastases in the neck (N0) [3]. Although reduced patient survival has been reported in cases with patent neck metastasis, objections have been raised as to the methods applied by those studies [4-6]. The aim of the present study was to investigate the clinical and anatomo pathological variables associated with greater risk of cervical lymph node dissemination, as well as the characteristics and pattern of dissemination of metastases in individuals with PTC.
This was a retrospective study of 203 individuals with PTC subjected to surgery from 2005 to 2013. From that initial sample, 95 volunteers were excluded because lymph node dissection was not performed, three were excluded because they exhibited other concomitant head and neck malignant neoplasms, and four were excluded because they exhibited histological variants other than the classical and/or follicular ones. Therefore, the final sample comprised 101 individuals with histological diagnosis of classical PTC or its follicular variant, whose surgery was performed by the same surgeon at the Clinical Hospital of Federal University of Minas Gerais (Universidade Federal de Minas Gerais – UFMG) and Benjamin Guimarães Foundation/Baleia Hospital, Belo Horizonte, MG, Brazil. Eighty-two (81.2%) were female and 19 (18.8%) were male, and the average age of the sample was 42 years (range 10– 75 years). The participants were subjected to central compartment lymphadenectomy, i.e., bilateral dissection of levels VI and VII. In the cases with suspected lateral lymph nodes, lateral neck compartmental lymphadenectomy (levels II to V) was also performed (Figure 1). Figure 1 – Neck-lymphatic drainage levels Adapted from Porcaro- Salles et al. [7]. The non-parametric chi-squared test of independence was used in the analysis of the categorical variables of interest. In the case of variables represented by fewerthan five individuals, Fisher’s exact test was used. Student’s t-test was used to compare continuous variables, such as lymph node size and number of dissected lymph nodes. Multivariate analysis was performed by means of binary logistic regression, including the variables that exhibited p-values lower than 0.05 on univariate analysis. The significance level was established as 5% in all the tests. Analyses were performed using IBM-SPSS® v. 20. The study was approved by the research ethics committees of the participating hospitals.
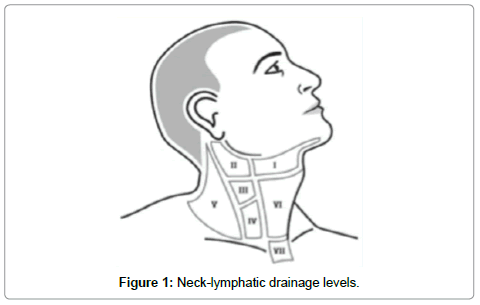
Figure 1: Neck-lymphatic drainage levels.
Among the 101 individuals assessed, 51 (50.5%) exhibited neck metastasis: 32/51 (62.7%) in the central compartment only and 19/51 (37.3%) in the central andlateral compartments. In no case were the metastases contralateral to a unilateralprimary tumor. Four cases of bilateral central compartment metastases occurred, all in individuals with multicentric disease affecting both thyroid lobes. The average number of dissected lymph nodes per patient was 7.8 ± 4.7 in group N0 (without metastasis) and 20.3 ± 16.3 in group N+ (with metastasis). In the latter, the average number of lymph nodes dissected exclusively in the central compartment was 12.8 ± 9.1. Comparison of the number of lymph nodes dissected in the central compartment between individuals from groups N+ and N0 revealed a significantly larger number in group N+ (p = 0.01). The lymph node size varied from 0.1 to 4.0 cm. The average lymph node size was 1.32 ± 0.9 cm in group N+ and 1.15 ± 0.4 cm in group N0 (p = 0.34). Univariate analysis found that angiolymphatic infiltration, multicentric disease, extra thyroid extension, tumor diameter (≥ 1.0 cm), and age (< 45 years) were associated with the occurrence of neck metastasis (p < 0.05) (Table 1). In contrast, gender and follicular variant were not associated with neck-lymphatic dissemination (Table 1). Univariate analysis comparing the groups with (N+) and without neck metastasis (N0). Multivariate analysis showed that the individuals with multicentric tumors or angiolymphatic invasion had increased risk of necklymphatic dissemination (respectively, p = 0.014, odds ratio (OR) = 4.113; p = 0.003, OR = 5.997). Tumors with diameter ≥ 1.0 cm had increased risk of neck-lymphatic dissemination (p = 0.043, OR = 3.098). The risk of neck metastasis of individuals with extra thyroid extension of the tumor or age < 45 years was not different from that of the other individuals (p > 0.05 for both) (Table 2). Multivariate analysis assessing the risk of neck metastasis (OR: odds ratio; CI: confidence interval).
| Variable | N+ | N0 | Total | p | |
|---|---|---|---|---|---|
| Gender | Male | 11 (57.9%) | 8 (42.1%) | 29 | 0.323 |
| Female | 40 (48.8%) | 42 (51.2%) | 82 | ||
| Age | < 45 years old | 34 (58.6%) | 24 (41.4%) | 58 | 0.045 |
| ≥ 45 years old | 17 (39.5%) | 26 (60.5%) | 43 | ||
| Size | < 1.0 cm | 9 (28.1%) | 23 (71.9%) | 32 | 0.002 |
| ≥ 1.0 cm | 42 (60.9%) | 27 (39.1%) | 69 | ||
| Extrathyroid extension | Present | 18 (75.0%) | 6 (25.0%) | 24 | 0.005 |
| Absent | 33 (42.9%) | 44 (57.1%) | 77 | ||
| Histological variant | Classical | 38 (50.7%) | 37 (49.3%) | 75 | 0.567 |
| Follicular | 13 (50.0%) | 13 (50.0%) | 26 | ||
| Multicentric disease | Single | 35 (44.9%) | 43 (55.1%) | 78 | 0.032 |
| Multiple | 16 (69.6%) | 7 (30.4%) | 23 | ||
| Angiolymphatic | Present | 28 (78.6%) | 6 (21.4%) | 28 | 0.001 |
| invasion | Absent | 29 (39.7%) | 44 (60.3%) | 73 |
Table 1: Univariate analysis comparing the groups with (N+) and without neck metastasis (N0).
| Variable | p | OR | (95%) CI |
|---|---|---|---|
| Angiolymphatic invasion | 0.003 | 5.997 | 1.816 -19.805 |
| Multicentric disease | 0.014 | 4.133 | 1.330 - 12.844 |
| Size ( ≥ 1.0 cm) | 0.043 | 3.098 | 1.036 - 9.262 |
| Extra thyroid extension | 0.389 | 1.760 | 0.486 - 6.378 |
| Age < 45 years old | 0.081 | 2.334 | 0.901 - 6.044 |
Table 2: Multivariate analysis assessing the risk of neck metastasis (OR: odds ratio; CI: confidence interval).
All the individuals included in the present study were subjected to cervicallymph node dissection, and the presence of micrometastases was established basedon histological examination. Whenever suspicious lateral lymph nodes were found,lateral compartment neck dissection was systematically associated with centralcompartment dissection. The fact that all the surgical procedures were performed bythe same surgeon reduced the bias associated with the surgical technique used. Neck metastases were found in 51/101 (50.5%) participants, in 19 (37.3%) ofwhom the lateral compartment was also affected, agreeing with other authors’ reports. No participant exhibited metastases contralateral to the primary tumor, which is also asomewhat rare finding in other studies (9.8–18.9%) [8-10]. The patients with neck metastasis had more dissected lymph nodes than theones without metastasis (p = 0.01), but the lymph node size did not differ betweengroups (p = 0.34). Therefore, it was not possible to identify suspicious lymph nodesbased on their size exclusively (p = 0.34). Macdonald et al. [11] compared the sizes ofmetastatic and non-metastatic lymph nodes, and although the ones larger than 1.0 cm were associated with higher risk of malignancy, a substantial fraction of theindividuals they assessed had metastasis in smaller lymph nodes. Unfortunately, it is a retrospective study did not have access to the size of all dissected lymph nodes, only the size of the largest surgical specimen. Thus, exclusive resection of enlarged lymph nodes in the transoperative period is not reliable for diagnosing and treating neck metastases. All metastatic lymph nodes were ipsilateral to the primary tumor. Therefore, ipsilateral central compartment dissection might suffice to remove most metastatic lymph nodes, except in case of multicentric tumors. The index of metastases in patients with tumor size smaller than 1 cm tumor was 28.1%. Indeed, some authors [12,13] recommend ipsilateral central lymphadenectomy as routine in N0 tumors, as, in theory, the risk of surgical complications is reduced, without posing a threat to theaccuracy of the procedure.
All the instances of lateral neck metastasis were systematically associated with the presence of metastatic lymph nodes in the central compartment. This finding gives further support to the routine practice of central compartment dissection of the neck whenever the lateral compartment lymph nodes are dissected. Younger patients are usually given a better prognosis based on systems such as TNM [14] or MACIS [15]. Even so, the incidence of neck metastasis is higher in young patients, particularly in children, compared to older ones [16,17], regardless of prognosis. In the present series, the incidence of neck metastasis was higher in the patients <45 years old compared to the older ones (p = 0.045). This risk could not be quantified on multivariate analysis (p = 0.081). Angiolymphatic invasion was associated with a higher incidence of neck metastasis. However, its identification is performed only on histopathological examination of the surgical specimen, and thus, it might bear implications for the adjuvant treatment of disease. As concerns the histological subtypes, there was no statistically significant difference between neck-lymphatic dissemination in classical PTC and the follicular variant, in agreement with previous findings [18].
The participants younger than 45 years and those with multicentric tumors ≥ 1.0 cm in diameter exhibited a higher incidence of central neck metastasis (p < 0.05).
It is worth noting that both of these variables can be identified before surgery. Extra thyroid extension is a weak prognostic factor in PTC relative to the risk of local recurrence, and by itself, it indicates at least stage T3 in the TNM staging system. In addition, some studies have found that patient survival was shorter when the tumor extended beyond the thyroid capsule. In the present study, although univariate analysis showed that the participants with extra thyroid extension had a greater incidence of neck metastasis (p = 0.005), the corresponding risk could not be quantified on multivariate analysis. The impact of microscopic neck metastasis and elective cervical lymph node dissection is uncertain [3]. Some authors suggest performing elective cervical lymph node dissection ipsilateral to the tumor to remove most of the probably affected lymph nodes with less risk of surgical complications [12,13,19]. The results of the present study lend further support to that suggestion, as no instance of metastasis contralateral to the primary tumor occurred. In conclusion, the factors predictive of neck lymph node metastasis were age <45 years, tumor diameter ≥ 1.0 cm, multicentric disease, extra thyroid extension and angiolymphatic invasion. The neck metastases were all ipsilateral to the primary tumor. Lymph node size was not a reliable predictor of the presence or absence of metastasis, indicating that histopathological examination of the surgical specimen is necessary to establish a diagnosis of metastatic disease.