Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
![]() +44 1478 350008
+44 1478 350008
ISSN: 2329-8790
![]() +44 1478 350008
+44 1478 350008
Research Article - (2016) Volume 4, Issue 4
Introduction: To evaluate a new enhanced IPI proposal by the National Comprehensive Cancer Network (NCCNIPI) in DLBCL patients, we compared the IPI, R-IPI, and NCCN-IPI in DLBCL patients treated with rituximab, cyclophosphamide, hydroxydaunorubicin, vincristine, and prednisone (R-CHOP).
Methods: From June 2008 to January 2012, we retrospectively evaluated 146 DLBCL patients treated with RCHOP- 21 referred for cancer treatment in a single institution in Brazil. Patients' clinical data were assessed to calculate the IPI, R-IPI, and NCCN-IPI.
Results: Patients' median age was 58.9 years (range 16-86); 85 (57.8%) were female. According to IPI, risk categories were low (n=41, 28.1%), low-intermediate (n=43, 29.5%), high-intermediate (n=37, 25.3%), and high (n=25, 17.1%). Using R-IPI, risk categories were very good (n=19, 13%), good (n=65, 44.5%), and poor (n=62, 42.5%). According to NCCN-IPI, risk categories were low (n=12/147, 8.2%), low-intermediate (n=52/147, 35.6%), high-intermediate (n=62/147, 42.5%), and high (n=20/147, 13.7%). The median follow up was 42.8 months (0.6-71.2) with an overall survival (OS) at 48 months of 73.8% and 84.3% of PFS. Using IPI, the OS at was higher for low and low- intermediate risk than high and high-intermediate risk patients (85.9% vs. 59.2% p<0.001). The RIPI showed significant differences in OS (100% vs. 83.2% vs. 57.5% p<0.001) but not for PFS (p=0.67) among very good, good and poor risk groups. The NCCN-IPI demonstrated significant differences in OS (p<0.001) among lowintermediate, high-intermediate, and high-risk groups, with the high-risk group exhibiting worse OS (35% at 48 months) but not for PFS (0.166). According to IPI, the OS in high-intermediate and high-risk patients was 59.2%. Conclusion: In our study, the NCCN-IPI (but not the IPI or R-IPI) was able to discriminate a group of patients of higher risk of DLBCL treated with R-CHOP with worse median OS.
Keywords: Diffuse large B-cell lymphoma; Rituximab; Polychemotherapy; Prognosis; Brazilian patients
Currently, the most used prognostic index to predict overall survival (OS) and progression-free survival (PFS) and to identify high-risk patients for non-Hodgkin lymphoma (NHL) is the International Prognostic Index (IPI), which is based on five clinical characteristics: age, performance status (PS), Ann Arbor stage, extranodal involvement, and lactate dehydrogenase (LDH) level [1,2]. However, the IPI was developed before chemotherapy with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (RCHOP) became the standard treatment for diffuse large B-cell lymphoma (DLBCL) [3,4]. Since the advent of rituximab therapy, many efforts have been made to validate the IPI for patients with DLBCL treated with R-CHOP by constructing more powerful and more accurate models to discriminate different risk groups. The goal is to identify at earlier stages patients with a lower chance of cure by standard therapy and select them as possible candidates for more intensive therapy (such as autologous hematopoietic stem cell transplantation, ASCT) as first-line treatment.
Sehn et al., created the revised IPI (R-IPI) in a DLBCL population treated with R-CHOP at the British Columbia Cancer Agency (BCCA) and showed that patients with no risk factors presented a very good prognosis, while 1-2 risk factors resulted in good prognosis and 3-5 risk factors resulted in poor prognosis. The authors concluded that RIPI was a better predictor of outcome than standard IPI for patients treated with R-CHOP. However, R-IPI was not able to identify a true high-risk group, because the OS in this patient cohort exceeded 50% at 4 years [5].
In addition to clinical features, biological factors (e.g., gene signature of malignant cells; tumor expression of MYC, Bcl-2 and Bcl-6, by molecular or immunohistochemical analysis) have been proposed as prognostic indicators for DLBCL [6-8]. However, these outcomes have been contradictory, and molecular techniques are unavailable in clinical care because they are expensive and timeconsuming [9]. Likewise, the features related to reproducibility are an important and unsolved issue related to the routine implementation of immunohistochemistry [10].
The National Comprehensive Cancer Network (NCCN) recently proposed an enhanced IPI (NCCN-IPI) for DLBCL patients treated with R-CHOP [11]. The NCCN identified five prognostic factors that, when combined, resulted in four clear risk groups: age, PS, stage, LDH, and sites of lymphoma involvement. NCCN-IPI scoring ranges from 0 to 8. Patients are classified as low risk (0-1), low-intermediate risk (2-3), high-intermediate risk (4-5), or high risk (6-8). The NCCN-IPI elucidates better low- and high-risk subgroups (5-year overall survival [OS] for low vs. high risk: 96% vs. 33%) than the IPI (5 year OS for low vs . high risk: 90% vs. 54%). The NCCN-IPI demonstrated that, when combined with PS and disease stage, the stratification of serum LDH [into >1-3 (1 point) and >3 (2 points)], age range [>40-60 years (1 point), >60-75 years (2 points), and >75 years (3 points)], and the involvement of extranodal sites in major organs (bone marrow, central nervous system, liver/gastrointestinal tract, or lung) were more powerful than the IPI factors for predicting survival in DLBCL patients treated with R-CHOP. The authors suggest that this new NCCN-IPI more accurately recognizes patients that are unable to be cured with RCHOP, and therefore might benefit identified high-risk patients by enabling clinicians to offer them a more intensive therapy [11].
In order to evaluate the NCCN-IPI in the era of rituximab treatment, we compared the IPI and R-IPI with this enhanced NCCNIPI in a population of patients with DLBCL followed in a referral center for cancer treatment in Brazil.
Study participants
After we received approval from the local ethical committee, from June 2008 to November 2011 we retrospectively evaluated 146 de novo DLBCL patients (median age 58.9 years, range 16-86 years) treated uniformly at the Clinical Hospital/Sao Paulo Cancer Institute of the Sao Paulo University Medical School (FMUSP). Two experts in hematopathology from the FMUSP Department of Pathology reviewed the tumor histology for all patients.
Assessments
Baseline clinical and disease features, including age, sex, Ann Arbor stage, number of involved extranodal sites, LDH level, PS, B symptoms, bulky disease (tumor size ≥ 10 cm or cardiothoracic index >1/3) were obtained from patients’ medical records by a specific researcher. Hepatitis B virus, hepatitis C virus, and human immunodeficiency virus (HIV) serology; kidney, liver, and biochemical laboratory values; electrocardiogram; echocardiogram; bone marrow biopsy; computed tomography (CT) of the neck, chest, abdomen, and pelvis; and wholebody positron emission using tomography 18-fluorodeoxiglicose (18- FDG-PET/CT) were assessed at diagnosis for all patients. Patients with Waldeyer’s ring involvement also underwent stomach endoscopy.
Therapy and follow-up
The IPI, R-IPI, and NCCN-IPII were calculated for all patients as previously described [1,5,11]. Patients were treated with 6 to 8 cycles of R-CHOP-21 [Day 1: intravenous rituximab 375 mg/m2, cyclophosphamide 750 mg/m2, vincristine 1.4 mg/m2 (maximum 2 mg), and doxorubicin 50 mg/m2; Days 1 to 5: oral prednisone 100 mg/ day]. Patients with stage I/II non-bulky disease were treated with 4 cycles of R-CHOP-21+radiotherapy.
Patients with Waldeyer’s ring involvement or bulky disease in the sinuses, bones, testes, or breast underwent 3600 cGy radiation at the end of R-CHOP-21. Patients with involvement of testes, ovaries, breast, sinuses, or the paravertebral region received four intrathecal injections of methotrexate 12 mg and dexamethasone 2 mg as prophylaxis against relapse in the central nervous system (CNS).
Patients were re-evaluated after four cycles of R-CHOP-21 with CT and after the last cycle of chemotherapy with CT, PET/CT, as well as bone marrow biopsy for cases that exhibited bone marrow involvement at diagnosis. The response of the end of treatment was categorized as complete remission (CR), partial remission (PR), or progressive disease (PD) using the criteria of Cheson [12]. Patients in CR were followed every 2/3/6 months in the first four years and subsequently annually from the fifth year. The refractory and relapsed patients received the modified IVAC (ifosfamide, high dose cytarabine and etoposide) regimen [13] as salvage therapy, followed by ASCT. Patients with HIV or severe congestive heart failure were not included in the study.
Statistical analysis
The overall response rate (ORR), CR, PR, PD, OS, and PFS were defined according to standard criteria (Cheson 2007). The survival curves were estimated using the Kaplan–Meier method [14]. Cox’s proportional hazards regression [15] was used for multivariate analysis of OS and PFS. SPSS 14.00 software was used for statistical analysis; p<0.05 was considered statistically significant.
Overall response
The distribution of clinical features of the 146 patients evaluated is displayed in Table 1. The median age of patients was 58.9 years (range 16-86 years), and 85 (57.8%) were female. Forty-two percent of patients were older than 60 years and 23% were older than 70 years. The majority of patients (n=96, 65.8%) were diagnosed with advanced stage (III/IV) disease. B symptoms were observed in 80 patients (65%) and PS ≥ 2 in 33 cases (22.6%).
| Characteristics | N (147) | (%) |
|---|---|---|
| Age (years) | ||
| Median | 58.9 (16 – 86) | |
| Sex | ||
| Female | 85 | 57.8 |
| Male | 62 | 42.2 |
| ECOG1 | ||
| =1 | 113 | 77.4 |
| =2 | 33 | 22.6 |
| Extranodal localization2 | ||
| Yes | 56 | 38.3 |
| No | 90 | 61.6 |
| B symptoms3 | ||
| No | 43 | 35.0 |
| Yes | 80 | 65.0 |
| Clinical stage4 | ||
| I | 13 | 8.9 |
| II | 37 | 25.3 |
| III | 22 | 15.1 |
| IV | 74 | 50.7 |
| Bulky disease5 | ||
| Yes | 46 | 31.7 |
| No | 99 | 68.3 |
| LDH | ||
| Normal | 73 | 49.7 |
| Elevated | 74 | 50.3 |
| LDH above superior limit | ||
| >1 to 2 times | 50 | 34.0 |
| >2 to 4 times | 15 | 10.2 |
| >4 to 6 times | 5 | 3.40 |
| >6 to 8 times | 2 | 1.40 |
| >8 times | 2 | 1.40 |
1,2,4: Ignored variable in 1 patient;3 : Ignored variable in 24 patients; 5: Ignored variable in 2 patients.
Table 1: General characteristics of patients with DLBCL.
The ORR was 87.7%, with 69.7% CR and with a median follow-up of 42.8 months (0.6-71.2), the OS at 48 months was 73.8% and 84.3% of PFS.
IPI classifications
According to the IPI, the OS at 48 months did was significantly higher for patients with low (n=41) and low-intermediate risk (n=43) (85.9%) than patients classified as high-intermediate risk (n=37) and high-risk (n=25) (59.2%) (p<0.001) (Figure 1A). The 30-month PFS was 88.5% for patients of low and low-intermediate-risk and 75.4% for patients classified as high and high-intermediate risk (p=0.034).
R-IPI classifications
The R-IPI classified patients as very good risk (n=19, 13%), good risk (n=65, 44.5%), or poor risk (n=62, 42.5%). The OS at 30 months of very good risk was 100% and of 83.2% and 57.5% for good risk and poor risk, respectively (p<0.001) (Figure 1B). However the PFS was not significantly different among the three subgroups of risk (p=0.67).
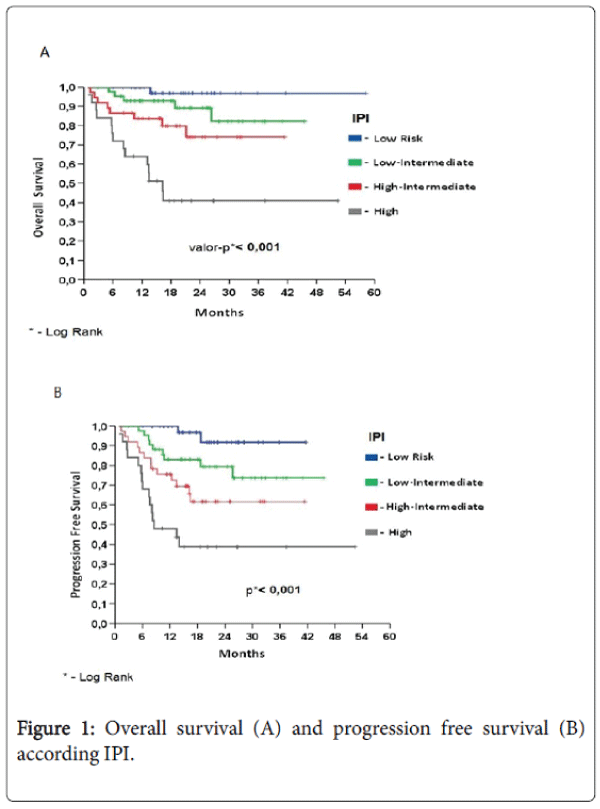
Figure 1: Overall survival (A) and progression free survival (B) according IPI.
NCCN-IPI classifications
The NCCN-IPI classified patients as low-risk (n=12/147, 8.2%), low-intermediate risk (n=52/147, 35.6%), high-intermediate risk (n=62/147, 42.5%), or high-risk (n=20/147, 13.7). The 48-month OS was 100% for patients classified as low-risk, 91.52% for patients classified as low-intermediate risk (mean follow-up 54.9 months; 95% CI: 51.4, 58.5), 68.4% for patients classified as intermediate-high risk, and 35% for patients classified as high-risk (p<0.001) (Figure 2A). The 48-month PFS was 100% for patients classified as low-risk, 87% for patients classified as low-intermediate risk, 78% for patients classified as intermediate-high risk, and 73% for patients classified as high-risk (p=0.166) (Figure 2B).
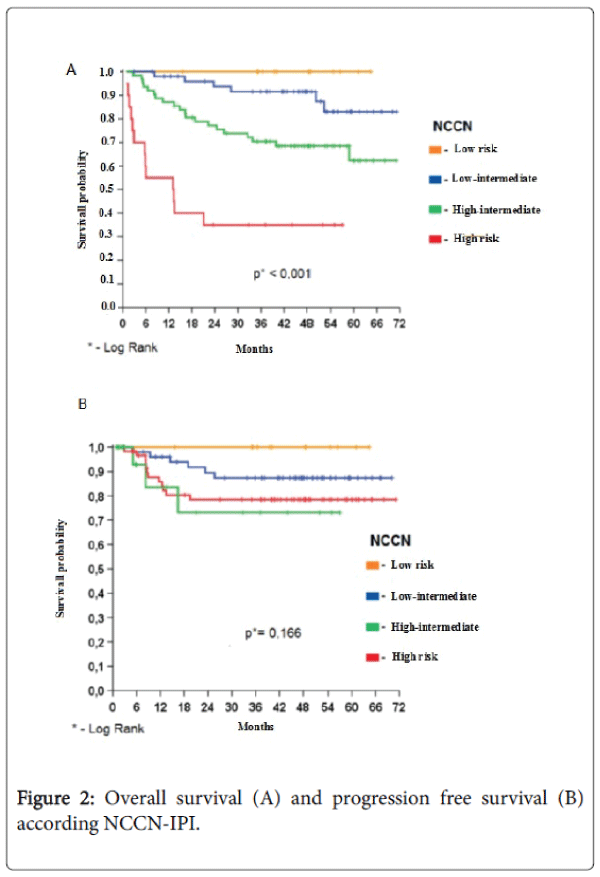
Figure 2: Overall survival (A) and progression free survival (B) according NCCN-IPI.
These findings demonstrate that the NCCN-IPI as previously described by Zhou et al., is able to accurately discriminate a high-risk group of DLBCL patients treated with R-CHOP-21 in Brazil. These patients exhibited a median OS and PFS of 14.9 months and 16.2 months, respectively, and 30% of patients exhibited OS>30 months. However, when the same patient population was classified using the IPI, the median OS and median PFS of patients in the intermediatehigh and high risk groups combined [11] were 35.2 and 35.4 months, respectively; 64.5% and 44%, respectively, exhibited OS >30 months. Similar results were observed when the R-IPI was employed [5]: patients classified as poor-risk exhibited a median OS of 31.1 months and a median PFS of 35.4 months, and 62.9% of patients exhibited OS>30 months.
These results clearly show a dramatic difference in terms of median OS for high-risk DLBCL patients identified by the NCCN-IPI vs. the IPI (16.2 vs. 35.4 months) and the NCCN-IPI vs. the R-IPI (16.2 vs. 35.4 months). In contrast, the same distinction was not observed for high-risk groups as classified by the IPI vs. the R-IPI (35.4 vs. 31.2 months). Therefore, it is reasonable to believe that IPI is not capable of identifying the truly high-risk patients.
Interestingly, the NCCN-IPI classified 20 patients (13.7%) as highrisk. This result was closer to that observed in the external validation cohort (BCCA) (14%) than that obtained in the NCCN cohort (8%) [11]. These authors associated the higher number of high-risk patients in the BCCA cohort compared with the NCCN cohort with a predominance of older and poor PS patients in the BCCA cohort. The median age of our casuistic was 58.9 years (range 16-86 years), older than in the NCCN cohort (57 years) and younger than in the BCCA cohort (63 years). However, in our study, almost one-half of patients were older than 60 years and 23% were older than 70 years. We also had a high percentage of patients with poor PS (2-4; 22.6%), which is higher than the NCCN cohort (11%). Furthermore, our casuistic showed a high percentage of patients with advanced stage III/IV disease (n=96, 65.8%). In our opinion, this data may justify the greater percentage of patients in the high-risk group observed in our casuistic compared with the NCCN cohort [11].
Our results are in agreement with previous studies that have demonstrated that although the IPI was considered the most important predictor of survival and the strongest index for recognizing high-risk patients before the advent of rituximab therapy, this potential has been lost in the rituximab era [5]. Indeed, we can assume that the IPI and the R-IPI should be interpreted as correspondent models to predict prognosis for patients with DLBCL that have undergone R-CHOP therapy. Although recently described, the NCCN-IPI appears to be a powerful, easy, and low-cost tool to better discriminate high-risk patients in the context of rituximab treatment.
Likewise, 12 patients (8%) and 40 patients (28.1%) were classified as low-risk by the NCCN-IPI and the IPI, respectively. The 48-month OS was 100% among patients characterized as low-risk by the NCCN-IPI, and 92.8% among patients characterized as low-risk by the IPI. This outcome was better than that obtained by Zhou et al., (96% by NCCNIPI and 90% by IPI). We suppose that the shorter follow-up (17.7 months) in our study in comparison with the NCCN-IPI study (3.1 years) explains this discrepancy, although in rituximab-treated patients relapses in DLBCL are seen more frequently during the first year posttherapy [16].
We believe that the ability to accurately detect the effects of aging and of different LDH values on the prognosis of DLBCL patients during the rituximab era is the hallmark of the new NCCN-IPI. Otherwise, the IPI dichotomized patients’ prognoses according to whether patients were older or younger than 60 years. However, the proportion of elderly patients (older than 65 years of age) in clinical trials has increased since the creation of the NCCN-IPI. In addition, the global population has also aged [17]. Therefore, we believe that the NCCN-IPI appears to be closer to real life. Likewise, as shown in the NCCN-IPI, higher LDH was associated with more aggressive disease. Zhou et al., showed that LDH level more than 3-fold higher than normal was statistically significant to predict prognosis in multivariate analysis in comparison with LDH levels that were 1 to 3 fold higher than normal [11]. Corroborating this data, the poor prognostic double hit lymphoma (characterized by chromosomal translocations involving both the MYC and BCL-2 genes) has been associated with high LDH levels [18,19]. In the present study, we also found that LDH >2-fold greater than normal was an independent factor for worse OS in multivariate analysis (p=0.07; hazard ratio (HR)=4.7; data not shown).
The NCCN-IPI strengthened the impact of PS as a strong prognostic factor for DLBCL. Similarly to the IPI, the NCCN-IPI confirmed that PS>2 was associated with worse prognosis. However, the NCCN-IPI did not improve the impact of the number of involved extranodal sites on OS and PFS among lymphoma patients. Surprisingly, only involvement of specific organs (e.g., bone marrow, CNS, liver/gastrointestinal tract, or lung) was predictive of prognosis. In contrast, our study results demonstrated that only lymphoma in testis was statistically significant for poor OS (p=0.043) in comparison with other extranodal sites (data not shown). In fact, we did not have any DLBCL cases with secondary CNS involvement at diagnosis, and 27 patients (48.2%) had primary gastric disease (data not shown). Shih et al., also demonstrated the poor prognosis of testis involvement in DLBCL [20]. The prognosis related to bone marrow involvement in lymphoma has also been controversial [21,22], and liver and lung involvement have been associated with worse prognosis [23].
The NCCN-IPI is easier to calculate because it uses clinical variables that are commonly accessible in clinical practice. Although based on a substantial number of patients, this was a retrospective analysis and we believe other groups should confirm it. To our knowledge, this study provides the first data outside the NCCN and the BCCA, and although it was also of a retrospective design, we used patients treated in clinical practice. To increase the reliability of our outcomes, our data were collected from medical records by a specific research that assessed the laboratory values and imaging results; two experts in hematopathology centrally reviewed the tumor histology.
In conclusion, when applied to a population of patients in Brazil, the new NCCI-IPI (but not the IPI or R-IPI) was able to discriminate a group of high-risk DLBCL patients with shorter OS after patients had undergone R-CHOP-21. We believe that the NCCI-IPI can be used to identify patients that are unlikely to be cured with the standard RCHOP regimen. This poor risk group can then be offered admission in clinical trials that employ new drugs or more intensive therapy.