Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2015) Volume 3, Issue 4
Introduction: Malaria and HIV are the leading causes of mortality and morbidity in sub-Saharan Africa. The interaction of these two pathologies raises fundamental issues as well as therapeutic. This study seeks a better understanding of the clinical profile of coinfected biological and therapeutic HIV-Malaria in Children's Hospital Pediatrique du jour Day Centre Hospital Universitaire Souro Sanou (CHUSS) Bobo-Dioulasso.
Methodology: It about a cross-sectional study with prospective and retrospective aspects. Included, were patients infected with HIV and followed in the service whose clinical and laboratory diagnosis of malaria had been performed and/or patients with whom the diagnosis of co-infection was done with the regression of a medical consultation following the consent of the legal representative.
Results: The prevalence of coinfection was 3.09%. The clinical signs of severity were dominated by impaired consciousness, convulsions and dehydration. As for biological signs, anemia was found in 65% of patients; leukocytosis was found in 19.6% of coinfected and thrombocytopenia in 9.3% of cases. HIV-1 was the most encountered serotype and immunocompetent patients accounted for 70.7% of coinfected. Pharmaco therapeutic groups were mainly administered antimalarial (100% of cases), analgesics-antipyretics (79.6% of cases), ART (48.1% of cases), antibiotics, especially cotrimoxazole (21.3% cases).
Conclusion: Immunosuppression induced by HIV infection did not appear to be associated with the frequency of occurrence of malaria. Chemo malaria prophylaxis in children living with HIV is not necessary. Consequently, malaria as a reason for consultation could be a gateway for the recruitment of children infected with HIV.
Keywords: Malaria; HIV; Children; Bobo-Dioulasso; Burkina Faso
Malaria and HIV are nowadays two major public health problems in sub-Saharan Africa. They are among the leading causes of morbidity and mortality. Indeed they cause over 4 million deaths each year, mostly in developing countries. Each year there are at least 50 million pregnancies in women living in malaria-endemic areas, about half in sub-Saharan Africa. It is estimated that, in this part of Africa a million pregnancies per year occur with women carrying HIV-malaria co infection [1].
Co infection is much encountered in children in this part of the world, since the vertical transmission is the main route of HIV transmission in children. In fact according to statistics, a child is subject to at least one fit of malaria each season season. Malarial transmission is prevalent in the endemic epidemic mode with an increase in the rainy season (from July to October). With regards to HIV infection, there were 10,000 children infected with HIV living in Burkina Faso in 2008. Bobo-Dioulasso is part of Burkina Faso's cities where the prevalence of HIV infection is high. In 2007 it was estimated at 3%, while the national prevalence was 2%. The profound impact of these infections on the immune system is generating interest in the scientific community [2]. Indeed, previous studies reported that HIV infection would be responsible for an increased incidence of malaria attacks and an increase in parasitaemia [3-8]. However, this finding is not shared by all, in fact, some authors have been reporting a low malaria prevalence (11.4%) in children infected with HIV compared to HIV-negative children (27.6%) [9].
HIV-co infection malaria may also pose diagnostic problems. Indeed for some authors high parasitaemia is associated with a high prevalence of false positive enzyme immunoassays, especially with young subjects [10,11]. Furthermore, therapeutic issues were raised by some authors [12,13].
Thus the combination therapies based on artemisinin (ACT) would have potential interactions with Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) and protease inhibitors (PIs) that are metabolized by CYP450 [14]. Also, the co-administration of sulfadoxine-pyrimethamine combination (SP) with cotrimoxazole or nevirapine increases the risk of liver and skin side effects, and with zidovudine the risk of bone marrow toxicity.
Evolutionary interactions between these two diseases have been reported by other authors, in fact during the acute phase of malaria the viral load of HIV would rise, increasing the risk of transmission, following a decline in CD4 rate observed [15,16].
This study analyzed the clinical profile, biological and therapeutic HIV-malaria co-infection in children tracked HDJ of Bobo-Dioulasso CHU allow a better understanding of the interaction between these two major diseases in Burkina Faso.
The study was conducted in the Department of Pediatrics of the Centre Hospitalier Universitaire Souro Sanou of Bobo-Dioulasso in western Burkina Faso. Two types of studies were carried out from July to December 2013:
1- Prospective sectional study for children whose HIV status was unknown at the beginning;
2- A retrospective cross-sectional study for children infected with HIV and followed in the service.
The population 1 consisted of patients with HIV followed in service and whose clinical and laboratory diagnosis of malaria was made.
Population 2 concerned the patients who consulted the pediatric ward for a suggestive clinical picture of malaria confirmed by parasitological examination; those with positive HIV serology were included. The inclusion was made after obtaining the informed consent of the parents or legal guardian.
For population 1 data was collected from the physical and electronic patient records. And the population 2, the clinical diagnosis was provided by a clinician, and laboratory confirmation of malaria was made from thick blood gouts after colouring with Giemsa 10% and viewed by light* microscopy. Positive cases in search of Plasmodium sp had received HIV status rapid tests (Determine®). A confirmation and typifying test was done when the first test was positive. SD Bioline® was used for this purpose. Sociodemographics, clinical, biological, pharmacological therapy data were collected using a questionnaire.
Newborns were between 0 and 29 days old and infants aged between 1 and 30 months, the toddlers over 30 months to 5 years, as for late toddlers and teenagers their proportion of respective age was over 5 years to 10 years and 10 years to 18 years. We considered severe anemia a hemoglobin (Hb) less than 7 g/L, a moderate Hb between 7 and 9 g/L and a light Hb levels beyond 9 g and less than or equal A11G/L. As for CD4 rate, we have taken into account the recommendations of WHO (2010) putting under treatment to classify our patients as follows:
1. Children 0-59 months [0-750 [cell/.mu.l Immunocompromised=750 and=immunocompetent
2. Children 60 months and over: [0-350 [cell/.mu.l Immunocompromised=350 and=immunocompetent.
The statistical test used was the Chi square test at 5% significance level. For low numbers and in the case where one of the expected values in a cell was less than 5, the Yates' correction was applied.
Epidemiological aspects of HIV-Malaria co infection.
In population 1: These were the children infected with HIV and followed in the service. The number of visits during the study period was 3313 including 102 cases of malaria, a prevalence of co infection of 3.07%.
In population 2 Children who were diagnosed with malaria at the beginning and whose HIV status was determined to hospitalization. Out Of 181 cases, there were 6 patients infected with HIV and 4 patients exposed (patients less than 18 months who tested positive to the rapid test: Determine®) i e, a prevalence of 3.3% in this population.
The overall prevalence of co infection was estimated at 3.09%.
Distribution of coinfection per age
The prevalence was higher in the group of teenagers (43.5%), Figure 1 shows the distribution of co-infection per age.
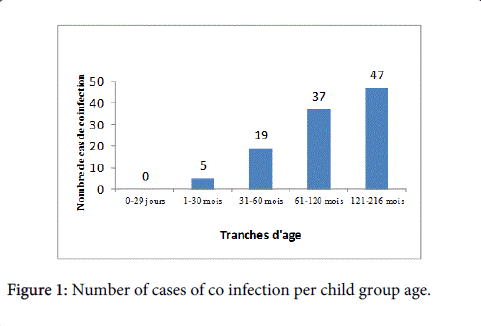
Figure 1: Number of cases of co infection per child group age.
Monthly dynamics of co infection
Malaria and HIV co-infection was more observed during the malaria transmission season (July-October). It was 12.9% (14 cases) in July, 20.4% (20 cases) in August, 20.4% (22 cases) in September and 27.8% in October i.e, 30 cases. Respective rates of 12% (13 cases) and 8% (9cas) were observed in November and December.
Clinical aspects of co infection
The most common clinical signs in the 2 populations were fever, headache and vomiting. Signs of gravity were dominated in the population 1 by consciousness disorders (3.9%), hemoglobinuria (0.98%), convulsion (0.98%) and jaundice (0.98% ), while in the population 2 we noted dehydration (50%), disorders of consciousness (33.3%), coma (16.7%) and seizures (33.3%).
Distribution of patients according to the type of malaria
Severe cases of malaria were 14% against 86% for simple malaria. All patients diagnosed HIV positive at the beginning had severe malaria, while with children infected with HIV and followed up at the Pediatrics Department, severe malaria concerned only 8.8% of cases of co infection.
Classification of patients according to the WHO clinical stage
Figure 2 shows the frequency of different clinical stages of HIV infection according to WHO classification. Patients in stage 1 represented the majority of cases (60.6%). There was a significant difference between clinical stage and evolution. The risk of death was higher in patients with advanced stages.
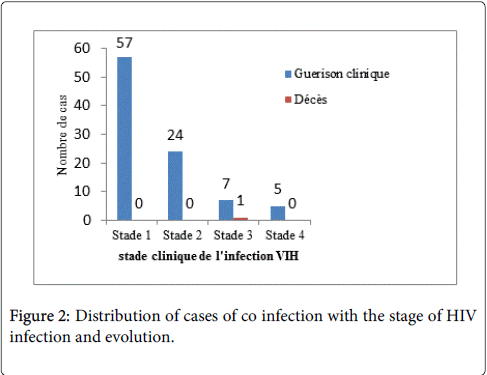
Figure 2: Distribution of cases of co infection with the stage of HIV infection and evolution.
Biological aspects of co infection
In both populations as shown in Figure 3, there was a higher incidence of mild anemia.
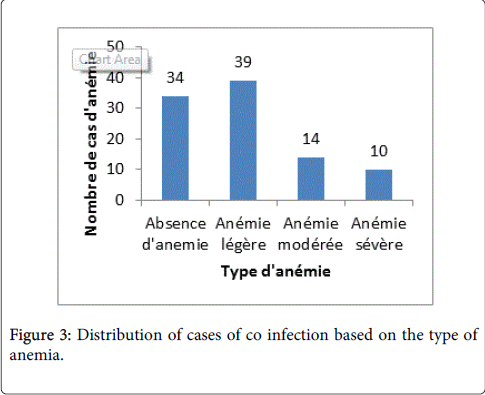
Figure 3: Distribution of cases of co infection based on the type of anemia.
In population 1, there was 66.7% of mild anemia; 22.8% of moderate anemia and 10.5% of severe anemia. In Population 2, severe anemia was found in 66.6% of patients with an equal distribution of the other two types of anemia ie, 16.7%.
Leukocytosis was found in 19 patients against 7 cases of leukopenia. With 71 patients no abnormalities of the leukocyte rate was observed.
In Population 2.50% of patients had leukocytosis against 17.6% in the population 1. thrombocytosis was present in 16 patients and thrombocytopenia in 9 patients.
The majority of patients showed no platelet defects (74.2%).
Distribution of patients according to their immunological profile
The frequency of HIV-1 infection was 97.2%. We reported a rate of 29.3% against 70.7% of immunocompromised immunocompetent. 60 months before there was a predominance of immunosuppression (71.4%), conversely after 60 months, immunocompetence predominated (75%).
Distribution of patients according to the CD4 count and type of malaria
Children under 60 months all had uncomplicated malaria. With the 60 months old and more , uncomplicated malaria had an almost equal distribution between immunocompetent and immunocompromised with rates of 90% and 88%. However severe malaria is met with greater frequency in immunocompromised (11.8%) against 9.8% in immunocompetent.
Pharmacotherapeutic support
Antimalarials were prescribed to all patients at respective rates of 86.1% (93/108) and 13.9% (15/108) for amodiaquine/artesunate and quinine, and 48.1% of patients were on antiretroviral therapy (ART).
Table 1 shows the distribution of pharmacotherapeutic groups used in coinfection.
| Pharmacological Groups | Fréquency | Percentages |
| Antimalarials | 108 | 100% |
| Antalgesics-Antipyrétics | 86 | 79,6% |
| ARV | 52 | 48,1% |
| Antibiotics and others Cotrimoxazole | 30 | 27,8% |
| Cotrimoxazole | 23 | 21,3% |
| Antiemetics | 12 | 11,1% |
| Antitussives | 12 | 11,1% |
| Antihistamines | 5 | 9,3% |
| Blood and derivetives | 4 | 3,7% |
| Iron | 3 | 2,8% |
| Oral solutes | 3 | 2,8% |
| Antispasmodics | 2 | 1,9% |
| Parasiteskillers | 2 | 1,9% |
| Anticonvulsants/sedatives | 1 | 0,9% |
Table 1: Frequency of therapeutic groups prescription.
As for ARV treatment, the combination of d4T-3TC-NVP represented the group of ARVs used mostly. The Figure 4 reports the distribution of the various combinations of used ART.
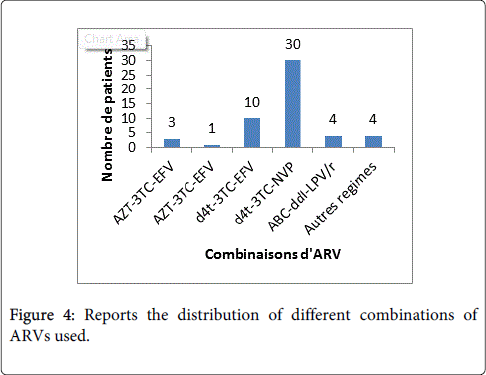
Figure 4: Reports the distribution of different combinations of ARVs used.
Prevalence of co infection
The overall prevalence was 3.09%. This rate is lower than those reported by Villamor, Tanzania (11.4%) and Whitworth, Uganda (11.8%) [9,17]. However, these two studies estimated the existence of parasitaemia or not with patients infected with HIV and not malaria disease and the prevalence of malaria in their respective studies could be lower because asymptomatic carriage of the parasite in the countries of stable malaria is common.
The low prevalence of malaria in children infected with HIV is also explained by the compliance by strengthening the medical care in these patients, and awareness of parents and guardians to early medical consultation at the slightest symptom of clinical suspicion of malaria. Kawo sharing our results in his study by relating a malaria prevalence four times higher with HIV-negative children compared to children infected with HIV [18].
Several hypotheses put forward to explain this finding include:
1. Co-trimoxazole prophylaxis, which would significantly reduce the risk of occurrence of malaria in children infected with HIV. In Mali, Thera reported a reduction in the incidence of malaria cases in children under chemo not infected with HIV prophylaxis [19]. Such a view shared by several other authors who reported their work in reducing the incidence of malaria attacks and mortality among HIV-infected patients receiving cotrimoxazole [12,16,20-22].
2. Oxidative stress created by the HIV infection in the erythrocytes that would be unfavorable to the development of Plasmodium [23].
3. Antiretroviral therapy would promote the control of malaria infections, firstly, by restoring the antimalarial immune response and on the other, by the effect of certain molecules that could have an antimalarial effect in vitro, so protease inhibitors such as ritonavir and saquinavir inhibit parasite growth in vitro at clinically effective concentrations [24,25]. ARV treatment also by non-nucleoside reverse transcriptase inhibitors is associated with a decrease in the incidence of malarial attacks without ruling out the involvement of the effects of immune restoration. [26] Thus Mermin brought through his work the impact of ARV treatment with co infected subjects. Indeed, the annual incidence of malaria without intervention was 50.8 episodes per 100 persons per year, which was reduced to 9 malaria episodes per 100 persons per year with chemoprophylaxis with cotrimoxazole only and 3.5 episodes per 100 person year with cotrimoxazole and antiretroviral treatment [20].
4. The reduction of HIV replication in human macrophages resulting from the presence of Plasmodium haemozoin in endothelial cells of the malaria cured patients or with chronic infection. In in vitro ,indeed,this reduction is associated with a restriction on the integration of the viral genome into the chromosome of the target host cells [26].
In population 1, the prevalence of co-infection was low with the less than 24 months. The administration of prophylactic cotrimoxazole being systematic in HIV-exposed children up to age 18 months to demonstrate the non HIV infection this could justify this finding.
However in Population 2, children 0-5 years old accounted for 83% of malaria population. The high incidence of malaria in this age group is well known in areas of endemic malaria prophylactic and extensive awareness campaigns are directed towards this target group in Burkina [27].
Temporal distribution of co-infection
The monthly dynamics of malaria transmission in Bobo-Dioulasso justify the increasing prevalence of malaria from July to October. Indeed in western Burkina Faso, malaria is endemic epidemic mode with a high prevalence during the rainy season (July to September) and a peak in early dry season (October) [28].
Clinical signs
Clinically, the three main reasons for consultation in the population 1 were pyrexia (97%), headache (61.8%) and vomiting (37.3%). Within this population signs of severity were pallor (3.9%), disorders of consciousness (3.9%), repeated convulsions (0.98%), hemoglobinuria (0.98%) and jaundice (0.98%). In Population 2, the signs of severity differed from those observed in the population 1 with higher proportions of dehydration (50%), repeated convulsions (50%), disorders of consciousness (33.3%) of pallor (33.3%), coma (16.7%). Regular monitoring of patients infected with HIV and the effectiveness of management protocols for these children explain the low levels of gravity signs in the population 1. Although these signs are often found in the symptomatology of severe malaria in without any HIV infection [29], this difference in distribution of gravity signs in children infected with HIV and followed, and children whose HIV status was discovered during suspected signs of malaria should be elucidated [30,31].
WHO clinical stage
The majority of patients were in stage 1 of HIV infection (56%) and death was significantly correlated with WHO clinical stage was higher with advanced stage of HIV infection. However, the accountability of malaria as a cause of death at this late stage of HIV infection predominantly opportunistic infections remains difficult.
Hematology data
In population 1, mild anemia, however, was predominant in the population 2, severe anemia was reported in more than half of this population (66.7%).
The strong association severe anemia, HIV infection and severe malaria (whatever parasite density) in a high transmission area of malaria is also reported by several other authors such as Oura and Otieno and could explain the high prevalence of severe anemia in the population where the severe form of malaria prevailed [27,32].
In both populations, leukocytosis was the most frequent quantitative abnormality of leukocytes. The majority of patients exhibited no quantitative platelet defects (74.2%).
Immunological data
HIV Serotype 1 was predominant and found in 97.2% in our study. The prevalence of this serotype in Africa is known and reported by several authors [17,18]. As it is clear from our series, a high prevalence of immunocompetent individuals (70.7%).
Yet many authors through their studies have reported a drop in CD4 rates during a malaria attack, it is Mermin and Whitworth in Uganda [17,33]. The unavailability of CD4 count before malaria in some of our patients (population 2), does not permit the establishment of any link of changes in CD4 levels before, during and after an attack of malaria. But no relationship was observed between the clinical form of malaria and immunological profile of patients.
Therapeutic profile
The most prescribed antimalarial the combination were amodiaquine/artesunate with a rate of 86.1%. This is explained by the predominance of the simple form of malaria, the diagnosis was made with 86% of our patients, indeed, in accordance with national guidelines in Burkina Faso, which is part of the strategic plan to fight against malaria (2011-2015), the treatment of uncomplicated malaria uses the combination therapy amodiaquine/artesunate or artemether/ lumefantrine oral, injectable forms of artesunate, artemether and quinine are reserved for severe forms which concerned only 14% our patients[27].
Co infection does not require changing the therapeutic protocol compared to the treatment of uncomplicated malaria and severe malaria, which is shared by Brentlinger [34], although for some authors a delay was found in the clearance of parasite in patients infected with HIV and treated with artemisinin, suggesting a metabolic disorder of antimalarials according to the immunological profile of the host [35].
This study showed a low prevalence of HIV-malaria co infection in children. But malaria can be a testing ground for HIV infection. Co infection involved more teenagers than infants with strong higher frequency during the malaria transmission season. Leukocytosis is the most common laboratory abnormality during this co infection. No relationship was observed between the clinical form of malaria and the immunological profile of patients.
Treatment of malaria during co infection followed national guidelines for the fight against malaria. Signs of severe malaria were less observed in children infected with HIV and followed in Pediatrics.
Therefore, a devolution of health structures monitoring children infected with HIV, involving Health Centers and Social Promotion (CSPS), combined with a strengthening of medical monitoring of therapeutic and technical capacities of children infected with HIV malaria is essential.