Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2018) Volume 7, Issue 2
Community based health insurance scheme is an emerging and promising concept to access affordable and effective healthcare, to protect households from out of pocket expenditure and impoverishment. Accordingly, this study examined access, use and quality of services after the introduction of the scheme in Ethiopia. To conduct this study, mixed research approach, descriptive, inferential and thematic analysis employed concurrently to collect data from participants. The study finding disclosed that by avoiding out of pocket payment, community based health insurance improve access and overall quality of service. Moreover, health services utilization improved from 0.33 visits of individual per year in 2011 to 1.44 visits in 2016. However, there were limitations in some quality indicator, moral hazards (miss utilizations) and adverse selections (inclusion of chronically ill, poor and indigents) during enrolment. Generally, the purpose of the scheme is threefold: increase access and use by making healthcare services more affordable and equitable, improve health status of population, and mitigate the out of pocket financial consequences of ill health by distributing the costs of healthcare across all members of a risk pool within the scheme.
Keywords: Healthcare; Communicable diseases; Treatment; Agroecological zones
High and middle income countries have achieved universal coverage by introducing different financing mechanisms for healthcare such, as tax-based financing and/or social health insurance schemes. On the other hand, low income and middle income countries have made little progress and out of pocket expenditure for healthcare becomes a major cause of impoverishment for poor and vulnerable families who often represent the majority of the population [1].
People in developing countries who have low access and receive poor quality of services account for 92% of global annual deaths from communicable diseases, 68% of deaths from no communicable conditions, and 80% of deaths from injuries, and globally, about 150 million people face catastrophic health expenditures every year and 100 million’s fall into deep poverty after paying for health care [2].
In Africa, population still rely mostly on out of pocket payments (accounting for 30%-85% of total health spending in the poorest countries, and 37% in Ethiopia), which are associated with incurring very expensive health expenditure and privation. As a result, health service utilization and quality of service in Ethiopian remain very low. For example, outpatient healthcare utilization per capita per year has increased only marginally from 0.27 visits in 2000 to 0.3 visits in 2011.
In responses to high out of pocket expenditure, low utilization and quality of services, the government of Ethiopia introduced two types of health insurance schemes in 2011. The first is community based health insurance scheme (CBHI) for rural households and people engaged in the informal sectors intended to cover 83.6% of the population and the second is social health insurance which is mandatory health insurance program for formal sector employees [3]. Accordingly, the pilot CBHI scheme was tested in 13 Districts located in four regions (Tigray, Amhara, Oromiya, and SNNPR) of Ethiopia in 2011.
Studies have been conducted regarding the role of CBHI on access, quality of care and change in healthcare seeking behavior. For example, a literature review study examines link between CBHI insurance and access and use; nine from ten showed a positive and significant impact.
In Ethiopian, general evaluative assessment on the impact of CBHI in the whole country found out that 45 to 64 percent increase in the frequency of visits to public providers. Similarly, a study conducted by Ethiopian Health Insurance Agency (EHIA) stated that 72.3 percent of CBHI members visited health facilities and the likelihood of visiting when feeling sick was 26.3 percentage points higher than that of nonmembers. Moreover, factors affecting healthcare seeking behavior were examined and socio-cultural barriers, income, age and sex were main determinants [4,5].
Despite the existence of studies on CBHI and health care seeking behavior in Ethiopian context, previously studies focused on healthcare access and use of a specific geographic community were not linked with the introduction of CBHI scheme (for example, Dereje and Getnet, and Fitsum et al. Other studies focused on the general health care seeking behavior of rural Ethiopia irrespective of their socioeconomic and cultural context) [6,7]. Consequently, this study examine health service provisions in terms of access, utilization and quality of healthcare service of rural households following the introduction of community based health insurances scheme particularly on Tehuledere District in South Wollo Zone. According to USAID, following the introduction of new health insurance strategy in 2010/11 in Ethiopia, the District was one of 13 pilot Districts where the community based health insurances schemes initiated at the national level. The average enrollment rate for Tehuledere District was 91% which is significantly higher acceptances rate of CBHI than the national average (52.4%) of the eligible households’ nationally.
To establish the theoretical foundation for this research, two theoretical models: first, the socio-behavioral which theorized predisposing factors, consisting of socio-demographic variables combined with attitudes and beliefs interact with enabling factors mainly of economic variables, membership to community based health insurance and distances from health care facilities to produce the conditions under which a person is or is not likely to seek healthcare services when need factors such as symptoms of illness experienced [8]. In general, results from this studies showed that most component of the model correlated with households access and use of healthcare services, but enabling factor such as being membership to CBHI scheme was more important than predisposing components and the need component was least important (Enabling>Predisposing>Need factors).
Second, health belief model used as a leverage to establish the existence of a dichotomy between before and after introduction of CBHI health services utilization behavior and to examine healthcare seeking behavior in relation to perceived suitability, cost of treatment, severity and access for information about health care seeking behavior [9]. Health insurances is a means of coping strategy for perceived illness, people will become a member of CBHI scheme if he or she believes he/she is susceptible to disease and individual’s perception of illness severity or people with chronic illness joins CBHI scheme to access healthcare (Figure 1).
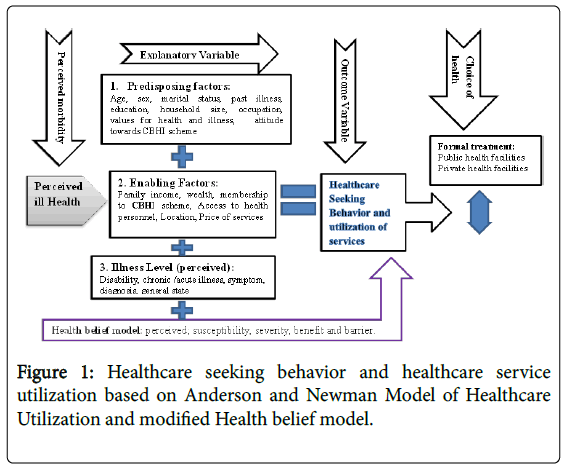
Figure 1: Healthcare seeking behavior and healthcare service utilization based on Anderson and Newman Model of Healthcare Utilization and modified Health belief model.
If a household does not perceive the illness as serious or low quality of services, they do not seek treatment or prevention and they have less possibility to become member of CBHI since individuals rationalize the cost of premium payment for the scheme and their health care visits or utilization episodes. Additionally, access to health information and members’ level of education provided impetus for prevention and health care utilization [10,11]. The absence of cues to action will reduce the likelihood of prevention and services utilization even though an individual is member of CBHI scheme. On the other hand, the absences of cost at the time of services increase health service utilization from modern health care facilities.
Study setting
The study was carried out in Tehuledere District which is one of the twenty two Districts in South Wollo Zone, Amhara Regional State in northeast Ethiopia located 430 kilometers from Addis Ababa on the main road to Woldiya and Mekelle. The District has total population of 110,226 among this, 59,238(53.74%) are males and the remaining 50.988(46.26%) are females. Majority of the population 107,055(97.12%) are rural population and only 3,171(2.88%) are urban population. Tehuledere District has 26 health posts and five public health centers, six small private clinics and three medium private clinics [12].
Study design
Cross-sectional study design employed to gather factual data from 344 head of household respondents and purposively selected informants. Relevant retrospective data on health seeking behavior for an illness episodes occurred in the past was also generated from March 4th to April 7th, 2017 [13]. Mixed research approach was employed to reconcile between the limitations with the representativeness from qualitative approach and reductionist nature of the quantitative approach. Household survey, FGDs, key informant and in-depth interviews were carried out.
Study population, sample size and sampling
Study participants were composed of rural households, CBHI scheme workers, health professionals, kebele administrative, religious leaders and elderly of the community. The study participants were recruited by employing both probability and non-probability sampling designs. The rural 21 Kebeles/tabias (the lowest administrative unit in Ethiopia) were the primary sampling units of the study District which were stratified in to three agro-ecological zones and member households taken (Dega, Woina dega and Kola) assuming varied distribution of diseases, illness episode, health risk factors, healthcare seeking behavior, psycho-social characteristics and ways of life in these agro-ecological zones. Lottery method was used to select one sample kebele from each agro-ecological zone [14].
Accordingly, in kebele 017 there were 887 payer insured households; in kebele 014 there were 749 payer insured households; in kebele 01 there were 835 payer households. Then, the total paying households with in the three kebeles become (N)=2471. Therefore, final sample size was 344 households from the total population of 2471 households. Then, 344 respondents were selected from insured households using simplified proportion sample size estimation formula; n=N/(1+N(e)2) provided by Yamane to determine the required sample size at a confidence level of 95%, and a 0.05 margin of error. Where; n is the sample size to be selected, e- is the acceptable sampling error, N-the population size and 95% confidence level, and p=0.5 were assumed.
After determining the sample size, the samples (344 head of households) were allocated in proportion for each kebele through (nk=(NK*n)/N)3. As a result, 121 sample households were selected from Segilen kebele, 104 and 116 sample households were selected from Wohelo and Bededo kebeles respectively. Where, nk=sample for each kebele, NK=total number of paying insured household in the population for each kebeles, N=total population (paying insured households for three kebeles), *=sign for multiplication.
The actual households for the survey were selected by employing systematic sampling technique based on the updated sampling frame acquired from District CBHI office. Finally, at household level either the head or spouses of the head of the households were randomly recruited for the study. The informants of qualitative research were recruited by using purposive sampling technique. Thus, six in-depthinterviews with patients were conducted [15]. Moreover, key informant interview had been made with three health extension workers, three kebele leaders, one CBHI scheme worker; seven health care professionals were interviewed. In addition, three FGDs had been made.
Data processing and analysis
The questionnaires completed by respondents were checked for completeness and consistency, then coded, and entered in to SPSS version 20 statistical software for final analysis. Descriptive statistics such as text, table, frequency, and percentage used to describe sociodemographic characteristics and health care seeking behavior of respondents. Statistical tests and models of such as, T-Test and one way ANOVA were employed to examine group differences and Pearson correlation used to see the relationships [16]. Each outcome variable was then investigated and 95% confidence interval was assumed. Results were considered significant at the p ≤ 0.05 significant level. The qualitative data were summarized and presented concurrently alongside with the quantitative data by using thematic analysis technique. Subsequently, based on the similarity of the themes, qualitative data were integrated with the quantitative ones concurrently based on themes in sequences of the study objectives.
Ethical considerations
The study was approved by ethical clearance obtained from Addis Ababa University and formal Letter from department of Sociology together with a permission letter approved by Thehuledere District administrative office, and all selected study kebeles. Each study participant was briefed on the study objective and verbal consent was granted and confidentiality was assured for any information provided.
Socio-demographic characteristics of participants
A total of 344 CBHI member households were included in the study. According to the data obtained from the survey, sociodemographically, most respondents were male (77%), majority (46%) respondents were with age group of 36-50, and significant majority (94.25%) belongs to the same religious category (Muslim), among the respondents, most of them (87.5%) are married. Regarding family size, half of respondents do have family size of 4-5 members and more than half respondents can’t read and write. Moreover, nearly half (46.2%) belongs to low income category [17].
The role of CBHI scheme on access to healthcare services
According to data obtained from respondents and informants CBHI scheme result better access to healthcare for excluded people especially, for the poor and chronically ill; hence, poor can benefitted by indigents entitlement and the chronically ill can be cross–subsidized by the healthy. Accordingly, by avoiding out of pocket payment CBHI scheme become instrument to achieve universal health coverage.
The role of CBHI scheme on healthcare seeking behavior
Most of respondents responded that CBHI scheme promotes access for healthcare from modern health facilities. Furthermore, respondents who though CBHI motivated households to seek modern health services were asked further why they motivate to seek modern healthcare frequently, and most of respondents assume that free of payment at the time of services and improvement in quality of services were prime reasons. To support the above responses, in-depth interview was used and one informant narrated his experiences as follow:
“After I became member to CBHI scheme, I did not worry to go to health facilities immediately. Before CBHI scheme, when someone in the family become sick, we can’t access money immediately; either we have to wait the market day or we have to borrow from someone … since money for rural people is hard to find. Now the only thing that you have to worry is having your card [CBHI membership card] and you will get any services any time you want. Consequently, I never left my card out of my pocket because it is my life insurance (male, age-44) .”
The impact of CBHI on delay and utilizations of healthcare service
As depicted on the Table 1, from perspectives of the rural dwellers (member households) and real actors or healthcare providers, health service utilization or numbers of visits of healthcare facilities for the last three months, nearly half (45.3%) of respondents have visited 1-2 times. Furthermore, considerable number of respondents (33.3%) did not visit health care facilities. Moreover, half of the respondents (50.4%) seek treatment without delay; only 5% delay more than a week [18].
| Services utilization and Delay | Frequency | Percentage (%) | |
|---|---|---|---|
| Health service utilizations or number of visit for the last three months |
0 (Zero) | 111 | 32.3 |
| 1-2 time/s | 156 | 45.3 | |
| 3-4 times | 56 | 16.3 | |
| 5-6 times | 15 | 4.4 | |
| 7 and more | 6 | 1.7 | |
| Total | 344 | 100 | |
| Number of days delayed after illness occurred |
0(No Delay) | 122 | 50.4 |
| 2-4 Days | 101 | 41.7 | |
| 5-7 Days | 7 | 2.9 | |
| 8-10 Days | 8 | 3.3 | |
| After 15 Days | 4 | 1.7 | |
| Total | 242 | 100 |
Table 1: Health service utilizations and delay.
Enabling factors and health services utilization
Enabling variables are among factor that promote or discourage health services utilization from modern health care facilities. Accordingly, from the enabling factors being membership to CBHI scheme tested through T-Test. As a result, being membership to community based health insurances is statistically significant at α=0.01 (Table 2).
| Enabling factors (characteristics) | Health services utilization or number of health facility visits | |||
|---|---|---|---|---|
| Frequency and Percentage | Test statistics | Sig(p) | ||
| Bing membership CBHI | Yes | 313(91.0%) | T-Test | 0 |
| No | 31(9.0%) | |||
| Level of Household Income | High | 50(4.5%) | One way ANOVA (F-Test) | 0.382 |
| Middle | 135(39.3%) | |||
| Low | 159(46.2%) | |||
Table 2: Enabling variables and health services utilization of Respondents.
However, the test statistics is not statistically significant at α=0.05 for groups who have different level of income. Hence, the prime role of CBHI scheme is to cross-subsidize households and reduce financial barriers so that every member can use health services any time; when services needed.
Impact of CBHI scheme on quality of healthcare provision
Based on measure of quality of services such as, drug availability, improvements in laboratory services, waiting time, referral system, staff motivation, availability of staff and cleanness of the health care facilities, the finding of the study disclose that majority respondents (59.9%) and most informants said that the introduction of CBHI has increased overall quality of health services both in inpatient and outpatient services, especially, laboratory services, referral system and cleanness of the facilities. However, beside increase in overall quality of services, due to high utilization and patient in flow, quality of services in some indicators such as, long waiting time, drug shortage and miss treatment by health care providers were considered challenges that brought less quality during service provisions.
As showed in Figure 2, of the total respondents, 206(59.9%) responded that overall quality increase, on the other hand, 73(21.2%) perceived that overall quality declines, 56(16.3) households view that there is no change in general services provision quality, and only 9(2.6%) did not know whether services provision increase, decrease or remain the same [19]. This claim supported by qualitative narrations. For example, one of the health professional key informants (with 11- years work experiences) in the visited healthcare institution [Sulula health center] asserted the beginning of CBHI scheme and its role in the improvements of overall quality of care as follows:
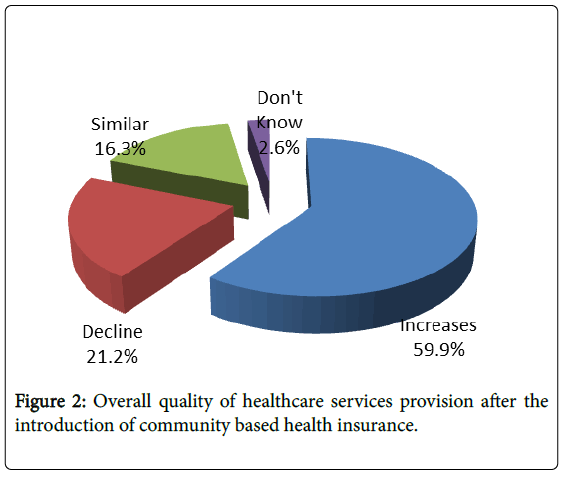
Figure 2: Overall quality of healthcare services provision after the introduction of community based health insurance.
“After the introduction of CBHI scheme we [health care professionals] have get some degree of freedom to prescribe the appropriate diagnostic test and drugs without any reservations about the ability of the CBHI member to pay. Prior to the introduction of CBHI we would either discuss with patients about their financial capability or write prescriptions based on what we thought the patients could afford, which is a relief professionally and key to improve the general quality of services.”
Over a century, many high and middle income countries have achieved universal coverage by introducing different financing mechanisms for health care such as tax-based financing and/or social health insurance schemes. On the other hand, low income and middle income countries like Ethiopia have made little progress in this aspect to cover people in the informal sector and rural population and out of pocket healthcare expenditure remain main cause of low healthcare utilization, low quality of services and impoverishments.
Furthermore, according to Tabor, health costs, if paid by selling assets, not only have the potential to reduce current assets, but also reduce farm productivity, nutrition intake, and future stream of income. Additionally, Msuya et al. asserted that nearly 55% of nonmember households relied on their own savings to finance their drug expenses compared to less than 11% for member households [20]. More than 20% of non-member households were obliged to cover the health expenses for sick individuals by selling crops, while this downs to less than 10% for member households.
The finding of this study examines the role of CBHI scheme on access, use and quality of healthcare services in line with various predisposing, enabling and need factors related to healthcare service utilization. Factors such as membership to CBHI scheme, sex, age, marital status and educational status are significantly affecting health service utilization and access to healthcare services.
Correspondingly, the finding of this study similar to other studies; for example, after the introduction of the CBHI, in the Democratic Republic of Congo the hospital admission rate among the insured increased dramatically, reaching 1.57 visits per individual per year and being five times (0.31) higher than among the non-insured. In Rwanda alike, the hospital admission rate among members was about 1.5 and only 0.06% among non-members [21]. Comparable, health services utilization in the study area increases from 0.33 visits per person in 2011 to 1.44 visits in 2016; which 4.4 times from the previous services used.
Moreover, Ranson stated that in risk-sharing schemes, the insurance premium is unrelated to the likelihood that all the insured will fall ill and benefits are provided on the basis of need; hence, payments go to the people who are most ill because people with lower incomes and those who are less educated tend to be in poorer health condition than those with higher incomes and those who are more educated [22].
Delay to seek medical services are now improved due to free access at the time of services it helps to remove barriers to access to health care, however, CBHI can also cause moral hazards, adverse selections and medical resistances, and inefficiency if no referral is required at hospitals: people will go directly to the hospitals to seek treatment even when suffering from minor ailments that could be taken care of at local health center or health posts [23].
After medical resistances created, the patient needed high cost of treatment or sometimes difficulties even for recovery at all. Moral hazards and unintended dysfunctions bring negative health outcomes. For example, a study by Jutting and Bennett found out that the moral hazard is common in CBHI scheme and provision of care is more expensive at the secondary level, the introduction of community based health insurance can worsen existing inefficiencies in the absence of a proper referral system.
Fundamentally, socio-economic feature of Ethiopia is predominantly rural/ agricultural and informal economy covering 83.6% of the population with low health services utilization rate and high user fee expenditure for healthcare. The low and falling healthcare utilization levels and healthcare seeking behavior, combined with poverty issues should call urgent need for Ethiopian ministry of health and stakeholders working on health and wellbeing to increased healthcare financing in Ethiopia through community based health insurance risk pooling system so that CBHI scheme become viable opportunity for the country’s need and socio-economic situation [24].
Furthermore, this research serves as an input for new policy approach formulation for organizations working on health such as, FMoH, NGOs and Ethiopian health insurances agency. Additionally, the finding of this study will provide factual data for stakeholders working on CBHI scheme. Moreover, this study will significant to instigate further researchers. Finally, EHIA and stakeholders should work together for the sustainability of the scheme and to minimize challenges such as adverse selections, moral hazards, drop outs and low enrolments.
Community based health insurance is no “magic bullet” to improve health care systems by itself rather proper design and implementation of major parameters are important. Like other empirical researches, the findings of this study discloses that community based health insurance has turned out to be a useful financial tool in the health sector reform in Ethiopia in general and in the study area in particular. Hence, out of pocket for healthcare services limited, CBHI scheme become realistic option to access health care for all, and to meet universal health coverage (UHC). Generally, impact of CBHI scheme on access to care and equity in services utilization is viable. Accordingly, the purpose of community based health insurance is threefold: increase access and use by making health care services more affordable and equitable, improve health status of population through increased access, quality and use of health care services, and mitigate the out of pocket financial consequences of ill health by distributing the costs of healthcare across all members of a risk pool within CBHI scheme. Accordingly, CBHI scheme needs to be an integral part of a national health financing strategy so that, addressing the inherent problem of health services provisions feasible.
The researcher would like to thank Addis Ababa University for its financial support to the realization of the study which this article is extracted. The researcher would also like to thank the study participants and data collectors who participated in this study.