Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Editorial - (2012) Volume 1, Issue 1
Completion thyroidectomy should be offered to those patients for whom a near-total or total thyroidectomy would have been recommended had the diagnosis been available before the initial surgery. This includes all patients with thyroid cancer except those with small (<1 cm), unifocal, intrathyroidal, node-negative, low-risk tumors. Therapeutic central neck lymph node dissection should be included if the lymph nodes are clinically involved. Ablation of the remaining lobe with radioactive iodine has been used as an alternative to completion thyroidectomy. It is unknown whether this approach results in similar long-term outcomes. Consequently, routine radioactive iodine ablation in lieu of completion thyroidectomy is not recommended.
Although reoperative thyroid surgery carries a higher risk of operative complications than initial thyroid surgery, experience has demonstrated that it can be performed safely by several different techniques. Nevertheless, thyroid surgeon in their practice should be aware of how to minimize the need for reoperative thyroid surgery and strictly adhere to detailed preoperative work-up and individual risk assessment before initial operation. Nothing less than a unilateral lobectomy with isthmusectomy should be performed as well as the surgeon must make every effort to preserve all encountered parathyroid glands and protect the recurrent laryngeal nerve at initial operation. Several adjuncts to thyroid surgery like intraoperative nerve monitoring or intraoperative iPTH assay may be of help in improving outcomes of individual performance. Such a strategy plays an ever increasing role in improving quality of thyroid surgery worldwide.
<Keywords: Completion thyroidectomy; Revision thyroidectomy; Well-differentiated thyroid cancer; Recurrent laryngeal nerve injury; Intraoperative nerve monitoring; Hypoparathyroidism; Intraoperative parathyroid hormone assay
Completion thyroidectomy should be offered to those patients for whom a near-total or total thyroidectomy would have been recommended had the diagnosis been available before the initial surgery. This includes all patients with thyroid cancer except those with small (<1 cm), unifocal, intrathyroidal, node-negative, lowrisk tumors. Therapeutic central neck lymph node dissection should be included if the lymph nodes are clinically involved [1]. Ablation of the remaining lobe with radioactive iodine has been used as an alternative to completion thyroidectomy. It is unknown whether this approach results in similar long-term outcomes. Consequently, routine radioactive iodine ablation in lieu of completion thyroidectomy is not recommended.
Completion thyroidectomy may be necessary when the diagnosis of malignancy is made following lobectomy for an indeterminate or nondiagnostic biopsy [1]. The most common indication for completion thyroidectomy is a frozen section analysis of a thyroid lesion that is interpreted as benign follicular adenoma. On subsequent final pathology report, areas of invasion are identified and the diagnosis is changed to follicular carcinoma. Thus, in general frozen section is not indicated in such cases as its accuracy is low and the result is often misleading. The need for completion thyroidectomy after unilateral thyroidectomy for indeterminate follicular lesion used to occur in 20% to 30% of the time in the eighties. However, the obligatory iodine prophylaxis that has been used worldwide resulted in remarkable decrease in prevalence of follicular thyroid cancer among all follicular thyroid tumors and recently grossly invasive follicular thyroid cancer represents not more than 5% to 10% of all follicular lesions, and is particularly prevalent among tumors larger than 4 cm in diameter. Some patients with malignancy may require completion thyroidectomy to provide complete resection of multicentric disease [2], and to allow RAI therapy. Incidental thyroid cancers have been detected in 3% - 16.6% of apparently benign goiters in numerous studies [3-5]. Though the majority of reported incidental thyroid cancers are micropapillary or micro-invasive follicular cancers, about one third of cancers are follicular cancers, and multicentric or large papillary cancers. Such patients need further surgical treatment after subtotal thyroidectomy, while a total thyroidectomy can be considered an adequate surgical procedure. There are many data which support this observations, as a significantly higher number of patients requires revision neck surgery for cancer following subtotal vs. total thyroidectomy [4-6]. The major indication for completion thyroidectomy in these patients is a positive fine-needle aspiration (FNA) result suggestive of papillary thyroid cancer originating from a 5 mm or larager lesion revealed by ultrasound within the remnant thyroid tissue during follow-up visits (multicentric papillary thyroid cancer), followed by suspicion of grossly invasive follicular or Hürthle cell thyroid cancer. Thus, completion thyroidectomy is undertaken to provide complete resection of multicentric disease, and to allow radioiodine ablation therapy according to the recommendations of the Revised American Thyroid Association Management Guidelines for patients with thyroid nodules and differentiated thyroid cancer [1]. It also makes it possible to follow the patients with thyroglobulin levels and identify metastatic disease by whole body scan with higher accuracy. Most [7-9] but not all [2] studies of papillary cancer have observed a higher rate of cancer in the opposite lobe when multifocal (two or more foci), as opposed to unifocal, disease is present in the ipsilateral lobe. There are no data to demonstrate that the completion thyroidectomy has any impact on recurrence or survival due to lacking prospective studies. Thus the decision should be individualized. On one hand, if the patient is at low-risk group (e. g. a 35-year old woman with a 1 cm minimally invasive follicular cancer) it is reasonable to maintain the patient with levothyroxine suppression and not perform completion thyroidectomy. On the other hand, if the patient is at high-risk group for tumor recurrence and mortality completion thyroidectomy should be undertaken. In evaluation for completion thyroidectomy the adverse histological features found on final report (e. g. tall or columnar cell carcinoma, diffuse sclerosing variant, extension beyond the thyroid capsule, or areas of undifferentiated carcinoma) militates towards completion thyroidectomy. Some authors consider Hürthle cell carcinoma to be more aggressive which warrants completion thyroidectomy. However, the most important prognostic factor in Hürthle cell tumor is the extent of capsular invasion. Minimal capsular invasion indicates excellent prognosis, while patients with widely invasive Hürthle cell carcinoma do poorly.
The surgical risks of two-stage thyroidectomy (lobectomy followed by completion thyroidectomy) are similar to those of a near-total or total thyroidectomy [10,11]. However, the risk of completion thyroidectomy following subtotal thyroidectomy is much higher and, if required, this should be attempted by experienced hands not later than 3-4 days after initial operation to avoid dangerous preparation within the inflamed tissues, or if not possible at least 8-12 weeks later when recognition of vital anatomical details is easier. In the latter case I personally prefer a lateral approach to avoid midline scarring, exposing the thyroid between the sternocleidomastoid and strap muscles. The postero-lateral aspect of the lobe should have not been scarred by previous dissection and surgery should be no more difficult than a primary operation. On the other hand, if only ipsilateral lobectomy with isthmusectomy was performed at initial operation and the contralateral lobe was not mobilized, dissection at completion thyroidectomy should be no different from that at first hemithyroidectomy as there is usually only minimal tissue reaction. Nevertheless, the technique of capsular dissection with careful identification of the recurrent laryngeal nerves and parathyroid glands is highly recommended as it reduces the risk of complications in secondary thyroidectomy [11].
Thyroid surgeon in their practice should be aware of how to minimize the need for reoperative thyroid surgery. This can be achieved by strict adherence to detailed preoperative work-up and individual risk assessment before initial operation.
Wide use of fine needle aspiration (FNA) biopsy for preoperative assessment of thyroid nodules has allowed for remarkable increase in percentage of patients with the preoperatively suspicious diagnosis of thyroid cancer among all patients qualified for thyroid surgery. FNA result allows to the surgeon to plan the appropriate operation properly. For example, total thyroidectomy plus level VI lymph node clearance should be undertaken in cases with high-risk papillary thyroid cancer. On the other hand, patients with unilateral follicular tumor or Hürthle cell lesion of indeterminate malignancy potential should undergo nothing less than a unilateral lobectomy with isthmusectomy and then await permanent pathological determination. This approach will result in a completion thyroidectomy only when the lesion ultimately turns out to be a cancer that necessitates total thyroidectomy. The need for completion thyroidectomy for indeterminate lesions occurs approximately 5% to 25% of the time. The morbidity of such completion thyroidectomy is minimized when the contralateral lobe has not yet been explored [11]. In addition to this, unilateral thyroid lobectomy is usually considered the appropriate surgical treatment of minimally invasive follicular carcinoma or some low-risk papillary thyroid cancer and need for future surgery is eliminated [1,12]. For conditions such as Plummer’s disease or Grave’s disease or even nontoxic multinodular bilateral goiter removing one lobe and performing a subtotal thyroidectomy on the contralateral side (Dunhill operation) is better than leaving macroscopic thyroid tissue remnants on both sides of the neck. If revision thyroid surgery is indicated, only one recurrent laryngeal nerve and two of parathyroid glands will be at risk of injury. It is important to stress that the surgeon must make every effort to preserve all encountered parathyroid glands and protect the recurrent laryngeal nerve at initial operation. In tertiary referral centers for thyroid surgery more and more total thyroidectomies have been performed for bilateral benign thyroid disease in recent years [1,3-5,13]. Such an approach minimizes the risk for future revision thyroidectomy to almost zero if incidental thyroid cancer is diagnosed. Similarly the risk of recurrent benign goiter following total thyroidectomy is extremely low but this can happen rarely as a result of microscopic thyroid tissue remnants missed in the operative field within one of the following sites: a piramidal lobe, tubercle of Zuckerkandl, or ectopic thyroid mass [5,13].
The preoperative physical examination and preoperative laryngoscopy is also helpful in minimizing need for reoperative thyroid surgery. A fixed thyroid mass or recurrent laryngeal nerve palsy should alert to the possibility of T4 malignancy. Such patients should undergo CT or MRI imaging and should be referred to experienced high-volume thyroid surgeon rather than be treated as a regular case scheduled for operation in a low-volume center. This approach may reduce need for reoperative surgery as a result of inadequate initial operation because the surgeon had to back out because of being not prepared for such extensive surgery [1,12].
Operative risks of revision thyroid surgery can be considerably minimized by thorough knowledge of surgical anatomy, knowledge of several different techniques to approach the thyroid gland, identify the recurrent laryngeal nerve and preserve parathyroid glands.
Preoperative workup
Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer are helpful in critical assessment of indications for reoperation [1]. However, one should remember that not all thyroid cancer requires a total thyroidectomy and many patients could be offered individualized treatment options.
Both the operative notes and pathology reports following the initial thyroid surgery should be carefully reviewed. It is important to identify before reoperation if patient is at increased risk of parathyroid insufficiency (e. g. patients who underwent parathyroid reimplantation as well as patients with inadvertently removed parathyroid glands at initial operation which were identified in final pathology report). Information about injury of the anatomical integrity of the recurrent laryngeal nerve injury is rarely reported in operative notes. Thus, it is of highest importance to perform laryngoscopy in all patients before reoperation. Unrecognized recurrent laryngeal nerve injury can be identified in as many as 5% of asymptomatic patients after initial thyroidectomy [14]. Recognizing recurrent laryngeal nerve injury preoperatively allows for both the surgeon and the patient to be prepared for the possible need for tracheostomy at completion thyroidectomy, should the contralateral nerve be injured.
Outcomes of revision thyroid surgery have been reported to be better in experienced hands (prevalence of permanent complications below 2% - 4%). Thus, such patients should be referred to specialized high-volume centers of thyroid surgery to avoid increased risks of reoperation undertaken in low-volume units.
At last, but not least one should remember about the optimal timing for completion or revision thyroid surgery. To avoid technical difficulties resulting from postoperative inflammation surgical intervention should be undertaken within first 4 days of the initial operation, or after 3 months to ensure the inflammation is decreased and tissue planes easier for dissection. However, a recent study of Tan et al. [11] has demonstrated that, provided sound surgical principles are adhered to, the timing of completion thyroidectomy may not have any impact on the incidence of permanent complications. First, it is recommended to perform a complete ipsilateral lobectomy with isthmusectomy at the initial operation. If the contralateral lobe is not mobilized , dissection at completion thyroidectomy should be no different from that at first hemithyroidectomy as there is minimal tissue reaction. Second, the technique of capsular dissection with careful identification of the recurrent laryngeal nerves and parathyroid glands reduces the risk of complications in secondary thyroidectomy [11].
Some surgeons recommend use of magnification loops (from 2.5x to 3.5x) to allow better visualization of vital anatomical structures in the scarified neck.
Value of intraoperative monitoring of laryngeal nerves in revision thyroid surgery is outlined later in this review.
Lateral approach
The lateral approach is one of the most commonly used approaches in revision thyroidectomy. With this approach, the thyroid gland is reached and dissected through previously undisturbed plane on the medial aspect of the sternocleidomastoid muscle. The anterior border of the sternocleidomastoid is mobilized lateral to the strap muscles and reflected laterally (Figure 1).
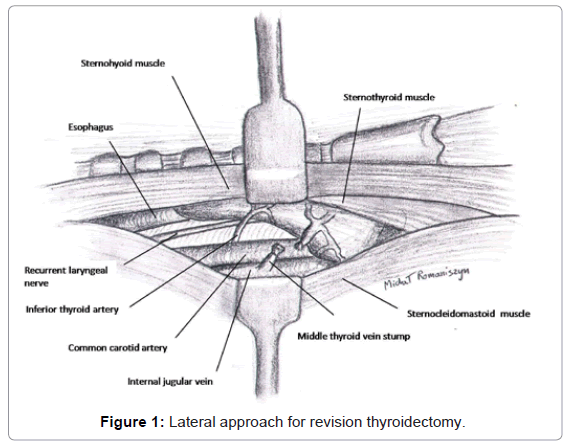
Figure 1: Lateral approach for revision thyroidectomy.
The omohyoid muscle and the sternohyoid muscle are reflected medially, whereas carotid sheath is reflected laterally. Such a dissection allows for exposure of the paratracheal space lateral to the inferior pole of the thyroid lobe. This plane is seldom disturbed from the previous thyroidectomy. The trachea and the esophagus can be smoothly identified. On the left side of the neck the recurrent laryngeal nerve is usually localized in the tracheoesophageal groove. However, on the right side, the recurrent laryngeal nerve ascends more oblique from lateral to medial towards the tracheoesophageal groove. Before identification of the recurrent laryngeal nerve it is not advised to divide the strap muscles as the nerve can be adherent to the posterior aspect of the sternothyroid muscle. Once the nerve is visualized the strap muscles can be divided inferior to the inferior pole of the thyroid to facilitate medial retraction of the thyroid lobe. The nerve should be then followed up into the previous dissected area by medial retraction of the thyroid gland and freeing the nerve from scarified tissue.
Ligation of the superior pole vessels in this approach should be proceeded by additional division of strap muscles at this level and followed by meticulous capsular dissection technique to take each of these vessels as they enter the thyroid capsule.
The exposure of the recurrent laryngeal nerve in a previously undissected plane is a major advantage of this approach. However, less experienced surgeons can find it more difficult to orient themselves in the anatomical detail much different from the standard anterior approach. Additional problems can be encountered in a case of big goiter when exposure of the superior pole of the thyroid is more time consuming. Similarly to this, parathyroid glands are more vulnerable to this technique as they can be inadvertently removed en-block with the scarified thyroid lobe and strap muscles. Thus, it is recommended to check the specimen for parathyroid glands, and if present they should be reimplanted.
Low anterior approach
In the low anterior approach the strap muscles are divided in the midline and retracted laterally as in a standard thyroid surgery. Careful dissection should lead to identification of the inferior thyroid artery and the recurrent laryngeal nerve below the artery in an area which is usually minimally scarified from the initial surgery. With this approach the recurrent laryngeal nerve should be searched for as low in the neck as possible to avoid unnecessary surgery through the scar. Palpation can be useful in some cases to located the nerve which can be felt with the nail of the index finger as a bowstring-like structure in the tracheoesophageal groove. Once the identification of the nerve is visually confirmed it can be followed up into the region of the thyroid and dissected free of the scar while the thyroid resection is performed. Most of the surgeons are familiar with this approach which is an advantage, but the dissection usually proceeds through the scarified tissues and exposure of parathyroid glands and the recurrent laryngeal nerve can be disturbed by undue bleeding which adds difficulty to the operation.
Medial approach to superior thyroid pole
For this approach, the avascular plane between the superior thyroid plane and the cricothyroid muscle is developed. The superior pole is retracted laterally, and the dissection is carried inferiorly along the larynx to the laryngotracheal groove. The recurrent laryngeal nerve can be usually encountered in this area as it enters the larynx within the inferior constrictor muscle. Retrograde dissection of the recurrent laryngeal nerve should be done with this approach to allow for safe removal of the thyroid lobe. The disadvantage of this approach lies in its unfamiliarity to most less experienced surgeons. This technique should be reserved for previously not resected thyroid lobe and for experienced surgeons.
Rodio-guided completion thyroidectomy
Radio-guided surgery has been recently performed in thyroid operations to facilitate dissection of metastatic lymph nodes and removal of recurrent tissues in patients with well-differentiated thyroid carcinoma, and in parathyroid operations to perform minimally invasive parathyroidectomy. The use of radio-guided surgery also has been recommended in completion thyroidectomy to detect the residual thyroid tissue and to achieve a complete resection [15]. Using this technique a completion thyroidectomy is performed with aid of an intraoperative hand-held gamma probe. Usually 5 mCi of 99mTc is applied by an intravenous route 20 minutes prior to the skin incision. After the dissection of the sternocleidomastoid muscle from the strap muscles, the background activities are counted from the left and the right shoulders with an intraoperative hand-held gamma probe. The probe is then placed in each thyroid gland site and count rates are recorded for 10 seconds. The sites with high count rates in comparison to the background activity are explored, and any residual thyroid tissue is removed. The background activity should be compared with the thyroidectomy bed to confirm the completeness of the procedure after the removal of the residual tissue. Although the intraoperative use of a handheld scintillation gamma probe may provide easy access to the residual thyroid tissue during completion thyroidectomy, it offers no benefit over conventional surgical exploration in the aspects of operation time, complication rates, and completeness of thyroidectomy in a center experienced in endocrine surgery. However, the assistance of a gamma probe for general surgeons, who are less familiar with reoperative thyroid surgery, might be very helpful in performing a more complete and safe completion thyroidectomy [16].
Revision neck operations for recurrence in the thyroid bed or cervical lymph nodes
Surgical re-exploration is the preferred method of management for locoregional recurrences (i. e. cervical lymph nodes and/or soft tissue tumor in the neck), when distant metastases are not present, and is usually followed by 131-I therapy. It is not clear that treatment of locoregional disease is beneficial in the setting of untreatable distant metastases, except for possible palliation of symptoms or prevention of airway or aerodigestive obstruction [12]. Impalpable metastatic lymph nodes, visualized on ultrasound or other anatomic imaging modality, that have survived initial 131-I therapy should be considered for resection. Conversely, the benefit to removing asymptomatic small (< 8mm) metastatic lymph nodes towards improving gross clinical disease recurrences or disease-specific survival is unproven. When surgery is elected, most surgeons endorse comprehensive or selective ipsilateral compartmental dissection of previously unexplored compartments with clinically significant persistent or recurrent disease (i.e. , lymph nodes > 8 mm in diameter,) while sparing vital structures (e. g. , ipsilateral central neck dissection [level VI], selective neck dissection levels II–IV, or modified neck dissection [levels II–V sparing the spinal accessory nerve, the internal jugular vein, and sternocleidomastoid muscle] as opposed to ‘‘berry picking,’’ limited lymph node resection procedures, or ethanol ablation, because microscopic lymph node metastases are commonly more extensive than would appear from imaging studies alone. Conversely, compartmental surgical dissections may not be feasible in the setting of compartments that have been previously explored due to extensive scarring, and only a more limited or targeted lymph node resection may be possible [1].
Recurrent neck disease uncontrolled by surgery and 131-I therapy is best treated by high-dose palliative external beam radiotherapy. As patients are likely to survive for a significant period, radical external beam radiotherapy (doses 50–66 Gy) is often necessary with a daily fractionation and meticulous radiotherapy planning techniques.
While the strategy outlined above is applicable in high-risk cases, the efficacy of an aggressive approach in low-risk cases where sensitive diagnostic techniques (high-definition ultrasonography, stimulated serum Tg measurements) indicate very low volume disease in the neck is less well established [12].
Methods of laryngeal nerves’ preservations during revision thyroidectomy
Routine identification of the recurrent laryngeal nerve now is part of treatment recommendations [1,12] and is regarded as the gold standard of care in either initial or revision thyroid surgery [13,17,18,20].
The recurrent laryngeal nerve crosses the inferior thyroid artery or its terminal branches at the level of the junction of the lower and the middle thirds of the thyroid lobe. The left recurrent laryngeal nerve ascends at the depth of the tracheoosophageal groove or just lateral to it at the lower pole of the thyroid. Usually it crosses deep to the inferior thyroid artery, sometimes between the terminal branches of the inferior thyroid artery, seldom superficially. The right recurrent laryngeal nerve courses more obliquely, being somewhat more lateral in position caudally. It rarely crosses deep to the artery, usually between its terminal branches. In fact, the nerve is particularly prone to injury at the level of inferior thyroid artery and in due course at the level of Berry’s ligament. Peripheral ligation of the branches of the inferior thyroid artery close to the thyroid capsule is the best way to preserve the nerve and the parathyroid glands, as well. The recurrent laryngeal nerve may be mistaken for a branch of the artery, particularly for the inferior laryngeal artery. The nerve is less regular, rounded, and elastic than artery. A small, red, sinous vessel, a vasa nervorum, can be noticed on it. However, during traction when the nerve is under tension, this small vessel can be hardly visible. The nerve rarely bifids below the inferior thyroid artery, but the closer the entry into the larynx the higher chance for encountering a ramified nerve, the value of which is approaching to 30% at the level of the Berry’s ligament. Thus, the safest way to visualize the recurrent laryngeal nerve is to search for it below the artery and when identified to follow its course upward. Each extralaryngeal branch of the recurrent laryngeal nerve should be preserved. At the two upper tracheal rings the nerve is embedded in the posterior portion of Berry’s ligament. This ligament extends posteriorly behind the recurrent nerve and loosely attaches the thyroid to the oesophagus. At the level of Berry’s ligament the inferior laryngeal artery is localized just posterior to the recurrent nerve and often gives off a small branch that crosses the nerve to enter the thyroid gland. Therefore, any bleeding in this area needs nerve identification before clamping this vessel to avoid injury to the nerve. Moreover, medial traction of the thyroid lobe should be as gentle as possible in this area to avoid nerve paresis due to pressure of posterior fibres of Berry’s ligament on the nerve against the lateral aspect of the trachea. Instead, it is preferable to retract the lobe upward after complete dissection of its lower pole, which facilitates to follow the nerve until its entry into the larynx.
Non-recurrent inferior laryngeal nerve is a rear anatomical variant and can be encountered in approximately 0.5% of patients, almost always on the right side. Presence of non-recurrent nerve is a result of vascular anomaly during embryonic development of the aortic arches and is associated with lacking innominate artery and presence of an aberrant subclavian artery (arteria lusoria), the condition which can be recognised preoperatively during Doppler ultrasound of the neck.
The following methods of recurrent laryngeal nerve preservation can be considered:
(1) visual nerve identification,
(2) use of magnifying glasses to facilitate nerve visualization,
(3) nerve palpation (against the trachea wall)
(4) visual nerve identification with aid of intraoperative electrophysiological nerve integrity monitoring system (IONM).
Thus, recent advances in thyroid surgery include IONM which significantly aids visual identification of recurrent laryngeal nerve, allowing even for nerve mapping before its visualization, and provides the surgeon with a functional dimension previously not available with visual identification alone. Recently, it has been documented in a randomized controlled trial that IONM decreased the incidence of transient but not permanent recurrent laryngeal nerve paresis following thyroidectomy compared with visualization alone [17]. The prevalence of transient recurrent laryngeal nerve paresis was lower in patients who had recurrent laryngeal nerve monitoring by 2.9% in high-risk patients (p=0.01) and 0.9% in low-risk patients (p=0.25). Despite these promising observations IONM technique is currently used mostly in high-volume thyroid surgery centres and is still under clinical assessment [18]. It is up to each surgeon to decide whether to use nerve monitoring as a routine adjunct to each thyroid operation or to reserve it for challenging operations. A recently published questionnaire study aiming to estimate the patterns of use of IONM devices during thyroid surgery by otolaryngologists in the United States documented that the majority them did not report regular usage of recurrent laryngeal nerve monitoring in their practices (only 28.6% of responders admitted to use this device regularly) [19]. Surgeon background and training, more so than surgical volume, significantly influenced the use of IONM. However, it is also important to stress that recurrent laryngeal nerve monitoring allows for nerve function documentation before and after thyroid resection (by printing the electromyographic signal of evoked potentials), which is of great importance in an increasing number of litigations.
One may consider IONM in three discrete modes of application [20]:
Identification (“neural mapping”) of the recurrent laryngeal nerve: The nerve is mapped out in the paratracheal region through stimulation and then visually identified through directed dissection provided by the neural mapping. Multiple studies suggest IONM is associated with a rates of nerve identification of between 98-100%. This is of great importance in revision thyroid surgery as identification of the recurrent laryngeal nerve in scarified tissues is more difficult than in initial surgery.
Aid in dissection: Once the nerve is identified, additional intermittent stimulation of adjacent non- neural tissue vs. nerve can help in tracing the nerve and all its branches though the dissected field.
Prognostication of postoperative neural function and lesion site identification: This has great significance in prevention of bilateral vocal cord paralysis given the frequent bilateral nature of the typical thyroid procedure. Prognostic statistics vary due to a number of factors but electric testing of the nerve represents a significant improvement in accuracy in prognostic neural function when compared to the currently available test of visual inspection of the nerve.
During revision thyroidectomy attempts should be also made to preserve the external branch of the superior laryngeal nerves (EBSLN) by ligation of the superior thyroid vessels at the capsule of the gland. It is also reasonable to dissect first the superior thyroid vessels away from the nerve by opening up a space between the cricothyroid muscle and the upper pole of the thyroid, and then ligate the vessels as low as possible on the surface of the thyroid gland.
External laryngeal nerve injury has an associated morbidity, particularly in voice-quality changes (loss of vocal cords’ tension makes it impossible to phonate with high-pitched voice sounds). Injury rates may be higher than for recurrent laryngeal nerve damage as it is usually overlooked at postoperative laryngoscopy. Barczyński et al. reported recently results of randomized controlled trial of visualization versus neuromonitoring of the EBSLN during thyroidectomy. It is worthy to note that use of IONM in this study significantly improved the identification rate of the EBSLN during thyroidectomy, as well as reduced the risk of early phonation changes after thyroidectomy [21].
Techniques of parathyroid glands’ preservation during revision thyroidectomy
Parathyroid glands should whenever possible be identified and preserved. Meticulous dissection and preservation in situ of all parathyroid glands encountered during thyroidectomy has been accepted as routine clinical practice for many years. However, attempts at preserving a functioning parathyroid gland with a long pedicle are destined to fail in many cases, as it infarcts later on as a result of thrombosis of the tenuous vascular supply, or as a result of edema and swelling of the gland within its dissected capsule. If vascular supply of preserved parathyroid gland/s is compromised, the gland/s should be excised and reimplanted into muscle. In such situations, as well as in cases of inadvertent removal of parathyroid gland found on inspection on the thyroid capsule after resection, parathyroid autotransplantation is the only valid alternative reported to reduce the incidence of permanent hypoparathyroidism.
Prior to any autotransplantation of the parathyroid gland, it is vitally important to send a small piece for frozen section to confirm that the autotransplanted tissue is truly a parathyroid gland, and not a lymph node or metastatic thyroid cancer. Most thyroid surgeons employ the standard technique of parathyroid autotransplantation described by Wells et al. In this technique the parathyroid tissue is placed in saline at 4ºC soon after excision. After cooling for 30 minutes, the gland is sliced into 1-mm slices (generally 10-20 pieces) and inserted into individual muscle pockets of the ipsilateral sternocleidomastoid muscle. The incisions are closed with nonabsorbable sutures. Use of many individual muscle pockets for parathyroid slices instead of one or two pockets only reduces the risk of graft insufficiency in case of hematoma formation around the transplanted tissue and resultant avascular necrosis. Alternatively to Wells technique parathyroid autotransplantation can be done using parathyroid tissue injection technique, which is preferred by some surgeons. To minimize the risk of permanent hypoparathyroidism to almost zero, it has been also suggested to perform routinely elective parathyroid autotransplantation of at least one gland in all patients undergoing thyroid surgery. In spite of the fact that such a strategy effectively prevents persistent hypoparathyroidism, it significantly increases the incidence of transient hypoparathyroidism requiring calcium medication prolonged for 12-18 weeks. To avoid this drawback of elective parathyroid autotransplantation, a tailored approach to parathyroid reimplantation based on the result of intraoperative parathyroid hormone assay might be beneficial for patients, meaning a zero risk of permanent hypoparathyroidism and a markedly reduced incidence of transient hypocalcemia. Intraoperative iPTH level within the reference range soon after total thyroidectomy indicates that at least two parathyroid glands function well and the risk of permanent hypoparathyroidism may be considered low. On the other hand, a drop in the iPTH plasma level below the lower limit of the reference range (<10ng/L) should be regarded as a permanent deficiency of at least three parathyroid glands, until proven otherwise, meaning a high risk of permanent hypoparathyroidism [22]. It is important to remember that lymph node dissection in the central compartment (level VI) is associated with an increased risk of postoperative hypoparathyroidism. Thus, all these high risk patients should benefit most from parathyroid reimplantation, while in low risk patients, parathyroid autotransplantation could be abandoned in order not to increase the incidence of transient hypoparathyroidism. Regardless of what approach to parathyroid autotransplantation is used, either liberal routine reimplantation or more conservative selective and based on clinical judgment supported by the result of intraoperative iPTH assay, a combination of both preservation of parathyroid glands in situ and by autotransplantation is essential in modern thyroid surgery, reducing the risk of permanent hypoparathyroidism following either total or completion thyroidectomy to almost zero.