Journal of Molecular Imaging & Dynamics
Open Access
ISSN: 2155-9937
ISSN: 2155-9937
Case Report - (2018) Volume 8, Issue 2
Introduction: This case report illustrates complex sigmoid diverticulitis presenting as tubo-ovarian abscess and developed iliopsoas abscess as complications.
Case description: A 37-year-old female presented with lower abdominal pain, fever and diarrhoea. Initial clinical assessment and CT imaging diagnosed tubo-ovarian abscess. She underwent laparoscopic drainage. Patient represented with similar complaints. Further imaging visualised persistent tubo-ovarian abscess with a new iliopsoasabscess. Her disease progression and initial treatment failure led to clinical diagnosis of sigmoid diverticulitis. The patient underwent Hartmann’s procedure and radiological drainage and has been asymptomatic since then. A Hartmann reversal is planned.
Discussion and Conclusion: First, it demonstrates the potential for sigmoid diverticulitis to present as tuboovarian abscess and develop iliopsoas-abscess complications. Second, it signifies prudence of high degree suspicion when evaluating female patients with pelvic abscesses and gastrointestinal symptoms. Finally, it shows the value of the MDT-approach in providing optimal care.
Keywords: Sigmoid diverticulitis; Tuboovarian abscess; Iliopsoas abscess; Radiology
A 37-year-old multiparous woman presented with lower abdominal pain, a high-grade fever and diarrhoea, with no significant past medical/surgical history. Initially, patient was diagnosed of left Tubo- Ovarian abscess based on clinical assessment and CT Imaging suggestive of left tubo-ovarian abscess. Patient underwent laparoscopic drainage of abscess but showed poor treatment response and further developed left iliopsoas abscess which was later diagnosed as complication that developed due to Sever sigmoid diverticulitis. Both Hartmann’s procedure for sigmoid diverticulitis and radiological drainage of iliopsoas were performed. Since then, the patient has been asymptomatic and clinically well and planned for Hartmann’s reversal. This case report summaries an unusual presentation of sigmoid Diverticulitis as tubo-ovarian abscess and developed an iliopsoas abscess as complications.
Colonic diverticula are due to outpouching of colonic mucosa and overlying connective tissue through the colonic wall [1]. According to Wong [2], 55‒66% of cases of diverticular disease occurs in patients who are older than age 80, and only 10% in patients who are younger than age 40. However, in recent years, the frequency of cases of diverticular disease in patients younger than age 50 has increased. Diverticula are usually asymptomatic, but when they are inflamed, they can lead to a condition called diverticulitis. If this condition is undiagnosed or untreated, it can proceed to various complications, including pelvic abscesses, peritonitis, diverticular fistula, and stricture [3-5].
Tubo-ovarian abscess is a severe presentation of pelvic inflammatory disease, and it can be caused by multiple factors, including poor hygiene, contraceptive devices, irritable bowel syndrome, diverticulitis and even cancer. The key factors for effective treatment and management are antibiotics with or without surgical intervention and identifying the root cause. This case report illustrates an atypical presentation of sigmoid diverticulitis and its management.
A 37-year-old multiparous woman with no significant past medical/ surgical history presented to the emergency department with lower abdominal pain of 3 weeks durations worse since past 2 days, associated with fever and diarrhoea. The patient was sexually active and had used intrauterine contraceptive device. On examination, the patient was pyrexial and had left iliac fossa tenderness with raised inflammatory markers (WCC 18.8, NEU 14.3 CRP 144). So, the patient was started on broad spectrum intravenous antibiotics. Two days post treatment, patient clinically deteriorated with further worsening of inflammatory markers (WCC 15, NEU 13.5, CRP 394) and so CT imaging was performed which showed a complex left adnexal mass 10.2 × 8.5 × 5.8 cm with fluid filled components and sigmoid colon draped over the superior-medial margins of this mass. Following the CT finding, the patient’s care was taken over by the gynaecology team.
On bimanual examination, the patient’s cervix was found to be displaced to the right, with tenderness and fullness in the left adnexa. Based on the patient’s age, history, findings of abdominal and bimanual examination and CT, a diagnosis of left tubo-ovarian abscess was established, and treatment was begun with antibiotics, followed by laparoscopic drainage of abscess.
A full immuno-suppression and tumour was conducted and came back negative. A pus culture grew an extended spectrum Beta lactamases E. coli and so patient was started in intravenous meropenem, as advised by microbiologist. In addition, patient exhibited raised HBA1c and therefore was newly diagnosed with Type 2 Diabetes and started in metformin. On Post-operatively Day 7, patient had a transvaginal ultrasound scan, which showed a complex left adnexal mass 6.6 × 5.6 × 5.2 cm. However, the patient was clinically improving and showed improved inflammatory markers, so she was discharged with outpatient Transvaginal Ultrasound scan in 6 weeks.
However, 20 days post discharge, the patient was readmitted with identical complaints of lower abdominal pain, fever, tenderness in the left iliac fossa and mildly raised inflammatory markers (WCC 8.5 NEU 6.1 CRP 68), Subsequently patient was started on IV Meropenem.
Further CT Imaging was performed and showed persistent left tubo-ovarian abscess (Figure 1). Further there was a separate focus of circumferential thickening in the midsigmoid colon, with soft tissue stranding in the adjacent fat (Inflammatory changes). In addition, a new Iliopsoas abscess of 15.7 × 5.3 × 9.3 cm (Figure 2) was noted which was in proximity with the left femoral vessel and had suspicion of possible extension of infective process into the hip.
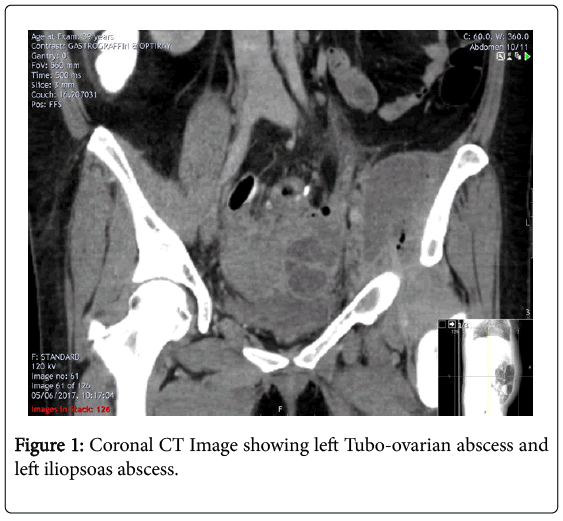
Figure 1: Coronal CT Image showing left Tubo-ovarian abscess and left iliopsoas abscess.
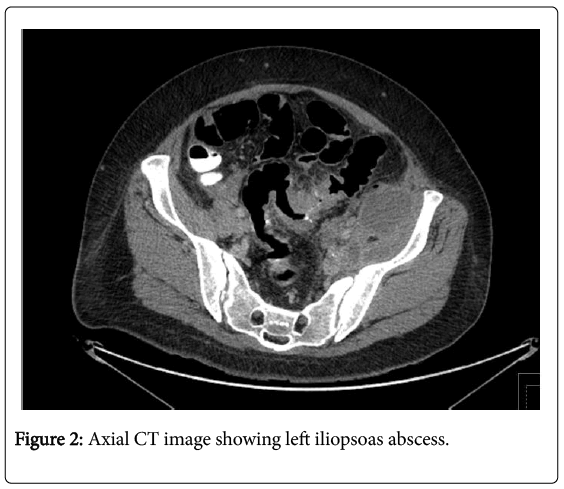
Figure 2: Axial CT image showing left iliopsoas abscess.
Due to the disease progression, failure of treatment, recent CT findings of mid sigmoid thickening and fat stranding and discussion with colorectal surgeon a clinical diagnosis of sigmoid diverticulitis was made, and patient was brought under joint care of colorectal surgery and gynaecology team.
Orthopaedic team was consulted regarding the suspicion of hip involvement due to iliopsoas abscess and because patient had full range of movements in all the joints, was advised to treat the primary source of infection (Sigmoid Diverticulitis). Since the iliopsoas abscess was inoperable surgically, radiological approach for the drainage of iliopsoas abscess was attempted using a 8 -- French Drain under ultrasound guidance, it was successfully inserted into the left psoas collections and the correct position of the drain was double checked with the CT, but there was no output from the drain and was concluded the collection to be thick and loculated and so was planned to treat by removing the primary source of infection and continue with antibiotics. Then, the patient underwent an emergency laparotomy for Hartmann’s procedure to treat sigmoid diverticulitis.
Histology confirmed the diagnosis and reported colonic diverticulitis with associated muscular hypertrophy and extensive organising peritonitis. A Pus culture grew E. coli and enterococcus faecium, which were then treated with intravenous Meropenem.
The patient clinically improved post operatively and so was planned to treat the complications conservatively with antibiotics and review her in clinic in 6 weeks to decide if any further imaging or interventions were required. Patient was discharged with red flags advice. Unfortunately, one month later, the patient was again readmitted with left loin pain and a spiking fever and on examination showed tenderness and markedly raised inflammatory markers (WCC 10.8 NEU 8.2 CRP 234). Further CT imaging showed an increase in size of iliopsoas abscess from 15 cm craniocaudally to 18 cm. With further MDT discussion, patient underwent repeat radiological drainage using 10 –French locking pigtail catheter and successfully drained 200 ml of bloodstained pus. Subsequently, MRI left hip and pelvis was performed and showed significant reduction in the size of left iliopsoas collection, with unchanged Tubo-ovarian abscess and no discrete/established features of septic arthritis or osteomyelitis in the left hip or pelvis. Patient clinically improved post operatively and was discharged with a follow-up transvaginal ultrasound imaging for TOA and clinic review in 6 weeks.
Since the time of last discharge, the patient has recovered well and has been asymptomatic for past one year.
Six weeks after last discharge, the patient attended a follow-up review appointment and underwent a transvaginal scan, which showed the known left tubo-ovarian abscess of size 7 × 5 cm. Because patient was clinically well and asymptomatic and patient’s interest to avoid surgery, a conservative plan was adopted to wait and watch while safety-netting the patient to return if any red flags symptoms arose.
At her One-year Review, she has been clinically very well leading her routine lifestyle and has been asymptomatic. Her TV US report showed no signs of any infection/abscess in the left fallopian tube and ovary and thus TOA was managed successfully.
Diverticulitis is a very common condition that usually presents with left iliac fossa pain, fever, and diarrhoea, classic symptoms that facilitate early diagnosis and effective management. On the other side, the same condition can present with atypical symptoms that are usually misdiagnosed and can result in intense complications, including iliopsoas abscess, as seen in the study case and in [6], or fistula, stricture and perforations [5], which have been life threatening.
First, this study case clearly indicates the potential that sigmoid diverticulitis can present as a tubo-ovarian abscess with both DVT and an iliopsoas abscess as complications. Second, it indicates the prudence of having a high degree of suspicion when evaluating patients with pelvic abscesses and gastrointestinal symptoms, particularly female patients. The close proximity of the left fallopian tube and ovary to the sigmoid colon means that there is always a chance of diverticulitis infiltrating the left ovary/fallopian tube and causing a tubo-ovarian abscess. Such an infiltration is indistinguishable from other common causes [6].
Finally, this study case indicates the value of a multidisciplinary team approach to providing optimal care. Overall, early recognition of diverticulitis as a root cause of tubo-ovarian abscess and prompt surgical treatment with radiological drainage will prevent complications, thereby helping patients experience early, uncomplicated recovery.