Journal of Molecular Imaging & Dynamics
Open Access
ISSN: 2155-9937
ISSN: 2155-9937
Research Article - (2018) Volume 8, Issue 2
Presently, CT is considered a first-line modality for evaluation of a variety of small and large bowel diseases. A wide spectrum of intestinal wall morphologic and enhancement abnormalities can be seen with bowel disorders. Once an abnormality is detected, the radiologist needs a systematic approach for determining the specific cause of the intestinal abnormality. Bowel wall thickening may be related to several entities, including normal variants, inflammatory conditions, and neoplastic disease.
Keywords: Inflammatory; Neoplastic; Bowel wall; Lesions
The CT findings that needs to be analyzed when assessing thickened bowel to differentiate benign and malignant lesions of bowel wall we consider, pattern of attenuation; bowel wall thickness; extent of lesion; degree of thickening symmetric, asymmetric with associated peri enteric abnormalities.
The normal small-bowel wall is thin, measuring between 1 and 2 mm when the lumen is well distended. However, the thickness of the normal small-bowel wall varies slightly depending on the degree of luminal distention. As a result, different criteria have been used to diagnose small-bowel wall thickening When the lumen of the small bowel is distended, the wall is often not seen [1].
If the bowel is partially collapsed, the wall measures between 2 mm and 3 mm with symmetric thickness. In these cases, we compare the degree of thickness of other similar distended segments to exclude disorders.
Although subjective assessment and assignment of a bowel wall attenuation abnormality to a category may prove challenging, this approach will narrow the diagnostic possibilities. Supplemental morphologic mural and regional factors provide specific diagnosis.
The retrospective study was carried out on patients during 2011- 2018 who underwent CT evaluation of abdomen for suspicion of bowel pathology based on clinical grounds.
The examinations were performed using 64 slice CT system. Somatom CT, Siemens Somatom Definitions, Germany. SIEMENS 16 slice spiral CT scanner. Scanning parameters: Voltage 120 kv, current 210 mA thickness 2 mm used. GE light speed 64 CT scanner. we review the images at an initial window width of 250 HU and window level of 45 HU. CT scans are obtained from the dome of the liver to the level of the perineum to cover the entire course of the intestine. Imaging with the patient in the prone position is recommended to disperse the small bowel loops.
The IV–contrast Ultravist 300 mg I/ml was used. Dose 2-2.5 ml/kg at a rate of 2 mL/sec through a 20-gauge intravenous catheter.
Enhanced contrast scan was performed, in two or three phases, with nonionic contrast agent and intravenous contrast, after injection of contrast arterial phase was scanned after 25-30 secs. Venous phase was scanned after 60-70 secs. Here many bowel wall observations may be very subtle, scanning technique with CT technology is important in differentiating intestinal abnormalities.
Study contents
Degree of bowel wall thickening: The small bowel wall should not exceed 3 mm despite luminal distention.
• Mild 3-4 mm
• Moderate 5-9 mm
• Marked-more than or equal to 10 mm
Density of involvement: To identify the general density of the thickening bowel wall lesions. The critical diagnostic observation when the general pattern of thickening of small bowel folds, appears perpendicular to the bowel lumen, parallel to neighboring fold, distorted, not perpendicular to the lumen, show angle with respect to neighboring folds:
• Symmetric
• Asymmetric
Length of involvement: The extent and location of bowel wall involvement should be evaluated.
a. Focal: Less than 5 cm
b. Segment: 6-40 cm
c. Diffuse: >40 cm
Enhancement pattern: We review the use of intravenously administered contrast material to assess the pattern accurately describe the five categories of attenuation patterns.
• Grey attenuation.
• White attenuation.
• Black enhanced.
• Water halo.
• Fat halo.
In this study, 122 cases of benign and malignant lesions were differentiated
In which 62 cases were male and 60 cases female, with age group between the age 20 to 80-years-old, with mean age 52.7. The main clinical symptoms were malaise, pain in abdomen, anorexia, loss in weight.
In total 122 cases, there were total of 46 cases of malignant bowel wall lesions and 76 benign cases
Of the total 122 cases, in 50 cases there was involvement of small bowel while in 72 cases were involved in large intestine. Certain lesions which extended towards the adjacent segment of bowel were classified into the category where the major length of abnormal involvement was seen.
In benign lesions, cases seen in small intestine, lesions seen in duodenum-(22 cases, 18.03%), lesions seen in jejunum-(30 cases, 24.5%), lesions seen in Ileum-(10 cases, 8.1%)
Cases of lesions which are involved in large intestine, lesions seen in ascending colon-(6 cases, 4.91%), lesions seen in Transverse colon-(2 cases, 1.6%), lesions seen in descending colon-(4 cases, 3.2%), lesions seen in sigmoid colon-(2 cases, 1.6%), rectum-(2 cases, 1.6%).
Malignant lesions, cases seen as adeno carcinoma-(24 cases, 20.5%), lymphoma-(10 cases, 9.8%), carcinoids-(9 cases, 7.37%), malignant GIST-(3 cases, 2.4%)
Among malignant lesions which are seen in Involvement of small intestine-(34 cases, 27.8%), large intestine (12 cases, 9.8%). lesions which involved both small intestine and large intestine were 3 cases.
Mild bowel wall thickening was seen in total 37 cases, 37 cases were benign, which was not specific for malignant cases
Moderate bowel wall thickening between (5-9 mm) in total 47 cases, 27 cases were Benign, 20 cases were malignant. Marked bowel wall thickening in 38 cases, of size between (10 mm-20 mm) 12 cases were benign, 26 cases were malignant.
Here, degree of thickening of lesions, mild, moderate, marked criteria for all lesions were considered separately for all 122 individual cases.
Asymmetrical bowel wall thickening seen in total 43 cases: Out of which in 43 cases, were malignant, 1 case was seen in benign cases
Here malignant lesions show 93% sensitivity, 51% specificity. Symmetrical bowel thickening was seen in total 79 cases. Out of which 75 were benign and 2 cases were malignant. Here benign lesions show 98% sensitivity, 53% specificity.
Here symmetry, asymmetry of lesions was considered for all 122 cases separately.
In total 52 cases showing focal involvement of bowel, 37 cases were in malignant group, 15 cases were benign
Here, malignant lesion cases show 80.4% sensitivity which is sensitive to predict the lesion, lesions show 65% specificity. In total 34 cases showing segmental involvement of bowel, 24 were in malignant group, 10 cases were benign. Here, malignant lesions show 52% sensitivity, while the lesions show 95% specificity, which is highly specific to show the malignancy of lesion. In total, 36 cases for Diffuse, 1 case was malignant and, 35 cases were benign. Here benign cases show 48% sensitivity, 86% specificity which is highly specific to show benignity of the lesions.
Here, focal involvement of lesion, show good sensitivity of 80.4% to evaluate the malignant lesions. Segmental involvement of lesions shows high specificity 95%, to evaluate the malignant lesions. Diffuse involvement of lesions shows, 86% good specificity to evaluate the benign lesions. Here, length of involvement, focal, segmental, diffuse were also considered separately for all 122 individual cases.
Density of lesions with heterogenous enhancement seen in total 53 cases, out of which 25 cases were malignant cause of bowel wall thickening: 28 cases were benign lesions
Malignant lesions show 54.3% sensitivity, 93% good specificity. Heterogenous enhancement shows highly specific for malignant lesions Table 1. Homogenous enhancement was seen in 69 cases, 48 cases were benign, 23 cases were malignant. Benign lesions show 63.3% sensitivity, 88% good specificity. Homogenous enhancement of lesion shows highly specific for benign lesions. Homogenous, heterogenous enhancement is also considered separately for all 122 cases.
| S.no | CT characteristics feature | Sensitivity | Specificity | |
|---|---|---|---|---|
| 1 | Heterogenous enhancement | 54.3% | 93% | |
| 2 | Moderate bowel wall thickening | 42% | 86% | |
| 3 | Marked bowel wall thickening | 55% | 92% | |
| 4 | Asymmetrical involvement | 86% | 54% | |
| 5 | Grey pattern of attenuation | 98% | 97% | |
| 6 | Focal involvement of lesion | 80.4% | 65% | |
| 7 | Segmental involvement | 52% | 95% | |
| 8 | Fat stranding | 65% | 92% | |
Table 1: Sensitivity and specificity of various CT characteristic features for labelling malignant lesions.
Color patterns of enhancement
In grey pattern, total 55 cases, 47 cases were malignant, 8 cases were benign, here malignant lesions show 97% specificity, 98% sensitivity. Grey pattern of enhancement was highly sensitive and specific marker to predict the malignant lesions. In white pattern, total 39 cases, 39 cases were benign, there was no malignant case. Here Benign lesions show 51.3% sensitivity, 95.1% specificity. White pattern of enhancement shows good 95.1% specificity for benign lesions. In black pattern, total 28 cases, 27 cases were benign, 1 case was malignant. Here benign lesions show 36% sensitivity, 57% specificity. Black pattern of enhancement shows 57% specificity for benign lesions. Here color pattern of enhancement was also considered separately for all 122 cases.
In benign group, fat halo pattern was seen in 1 case, it was not seen in malignant group
Fat halo pattern is not sensitive enough for benign lesions. Fat halo pattern is considered additional for 1 case in benign group.
Water halo pattern was noticed in 2 cases
In benign group 1 case of water halo pattern were seen. In malignant group, water halo pattern was seen in 1 case. Water halo pattern is considered additional for 1 case in benign group, 1 case in malignant group. Water halo pattern in Malignant lesions shows 50% specificity water halo pattern doesn’t show good sensitivity.
Associated CT findings like ulceration, necrosis, surrounding fat stranding were also monitored
Out of 24 cases showing necrosis, all cases were considered in malignant group.
Necrosis shows 50% sensitive for malignant lesions, 89% specificity for malignant lesion
Ulceration was seen in 36 cases, belonged to the malignant group: Ulceration shows 75% sensitivity, 95.6% specific for malignant lesions. Ulceration shows good specificity for malignant lesions.
Fat stranding was seen in 36 cases, fat stranding was seen in 6 cases of benign group, 30 cases were seen in malignant group
Fat stranding shows 65% sensitivity, 92% specificity. Here fat stranding was more specific for malignant lesions. Other additional features like ulceration, necrosis, fat stranding these features were considered additional on top of benign and malignant cases as mentioned above.
Perforation seen as local complication in (48 cases, 39.3%) out of which (44 cases, 36.06%) were in malignant group and obstruction is seen as major complication in total (57 cases, 46.7%) out of which (42 cases, 34.4%) were malignant
Bowel obstruction was seen in adenocarcinoma-(24 cases, 19.6%), lymphoma-(9 cases, 7.3%), carcinoids-(9 cases, 7.3%).
In total 122 cases, 10 cases were having ascitis, free fluid in abdomen, 2 cases were in Benign category, 8 cases in malignant group
Ascites shows 81% sensitivity, 62.5% specificity for malignant lesions.
Mesenteric involvement was seen in malignant group, which was not seen in benign cases. Mesenteric vessel involvement was seen in 9 cases of malignant group
Mesenteric involvement shows 75% sensitivity, 67% specificity for malignant group. Out of 122 cases, 80 cases showed lymph node positive status. 4 cases were seen in benign group. Among malignant group, 64 cases showed lymph node <1 cm diameter, while 12 cases showed >1 cm diameter. Lymph node positive status shows 95% sensitivity, 55% specificity for malignant lesions. Color patterns of attenuation, grey, white, black is taken for each individual 122 cases, Symmetry, asymmetry of lesion was also taken for each 122 cases, SPSS 23.0 medical statistics software was used for statistical analysis. Measured data were expressed as mean. The t-test was used for the comparison between the two groups. The data were expressed as frequency and percentage. We use SPSS Chi-square method, ANOVA method. The Chi-square test was used for the difference test between the groups where p<0.05 was statistically significant.
Relationship of degree of thickening in both benign and malignant types of lesion was further studied. In Mild thickening (up to 3 mm)-15 cases of benign lesions were seen, 4 malignant cases. In mild thickening from (3 mm-4 mm)-14 cases of benign lesions, 7 cases of malignant lesion were seen Figure 1.
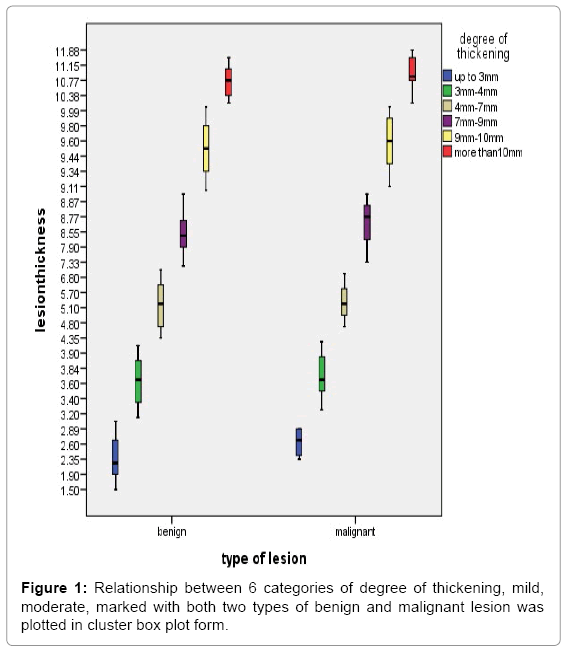
Figure 1: Relationship between 6 categories of degree of thickening, mild, moderate, marked with both two types of benign and malignant lesion was plotted in cluster box plot form.
X2=0.7, p=0.3, Here p>0.05.
In moderate thickening from (4 mm-7 mm)-12 cases of benign lesion, 7 cases of malignant lesions were seen. Moderate thickening from (7 mm-9 mm)–10 cases of benign lesion, 11 cases of malignant lesions were seen.
X2=0.9, p=0.3, here p>0.05.
In marked thickening from (up to 10 mm)-14 cases of benign lesion, 10 cases of malignant lesions were seen. In marked thickening from (more than 10 mm)-11 cases of benign lesion, 7 cases of malignant lesions were seen.
X2=0.03, p=0.8, here p>0.05.
We box plot the above cases: Here, 6 categories of degree of thickening in two types of both benign and malignant lesion was plotted in cluster box plot form Figure 2. Median value of both benign and malignant lesion is seen in interquartile range, in benign lesions, 6 different categories of mild, moderate, marked with two different sub categories was studied as mentioned above. In benign lesion median range of degree of thickness in interquartile range in each category is 2 mm, 3.6 mm, 5.1 mm, 8 mm, 9.5 mm, 10.7 mm respectively. Minimum thickness whisker value in interquartile range is, 1.5 mm and maximum are 11.1 mm. In malignant lesion, median range of degree of thickness in interquartile range is 2.7 mm, 3.7 mm, 5.6 mm, 8.8 mm, 9.7 mm, 11.2 mm. Here maximum value is 11.88 mm, minimum value is 2.3 mm.
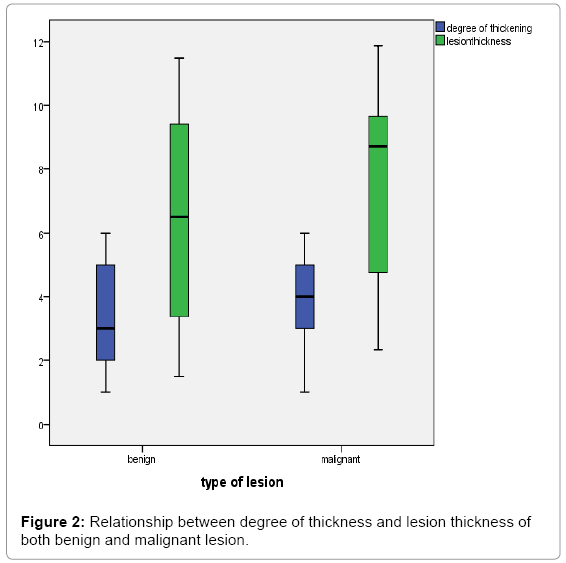
Figure 2: Relationship between degree of thickness and lesion thickness of both benign and malignant lesion.
We use, spss software via ANOVA method to calculate the value, f=780.3, p=0.0, which is less than p value, p<0.05, which shows statistically significant. so, we can say, median degree of thickness is different in different categories rejecting the null hypothesis Figures 3-13.
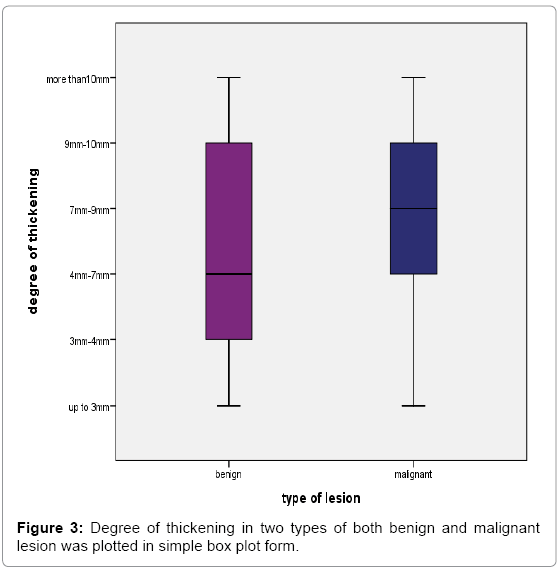
Figure 3: Degree of thickening in two types of both benign and malignant lesion was plotted in simple box plot form.
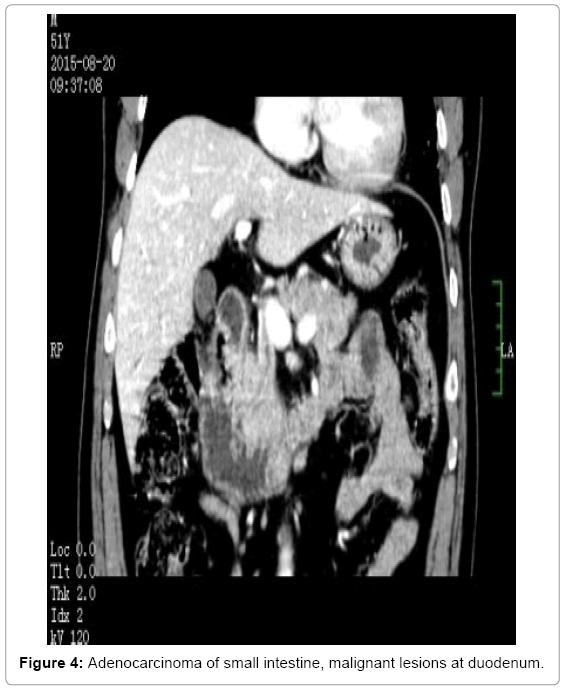
Figure 4: Adenocarcinoma of small intestine, malignant lesions at duodenum.
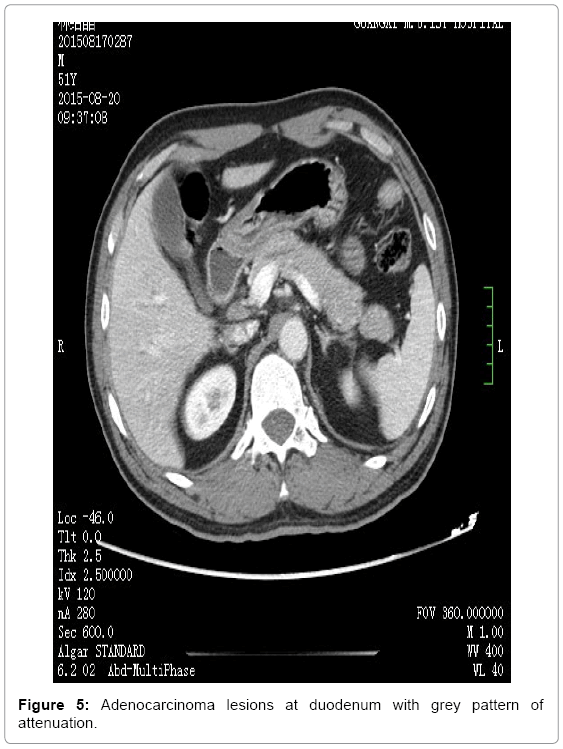
Figure 5: Adenocarcinoma lesions at duodenum with grey pattern of attenuation.
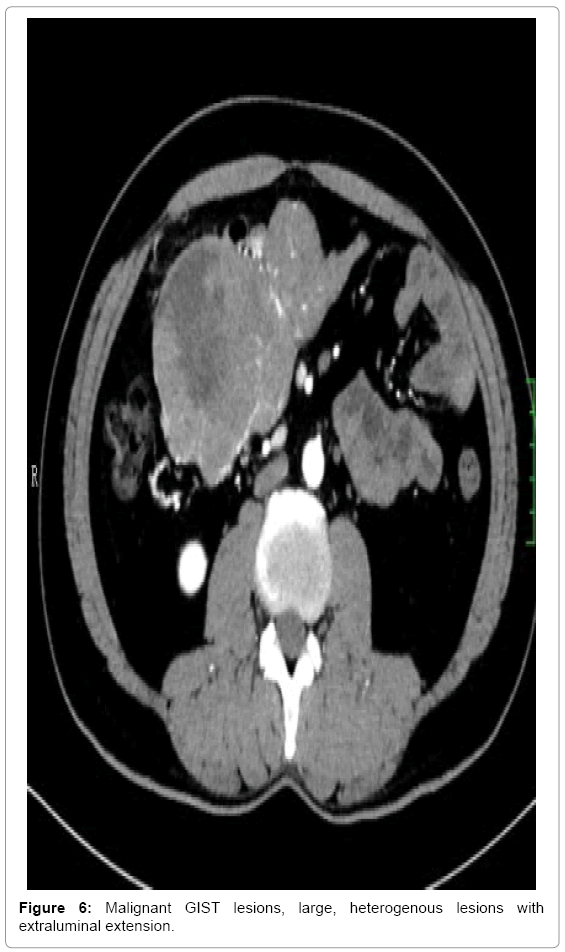
Figure 6: Malignant GIST lesions, large, heterogenous lesions with extraluminal extension.

Figure 7: Malignant GIST lesion, in small intestine, heterogenous enhancement.
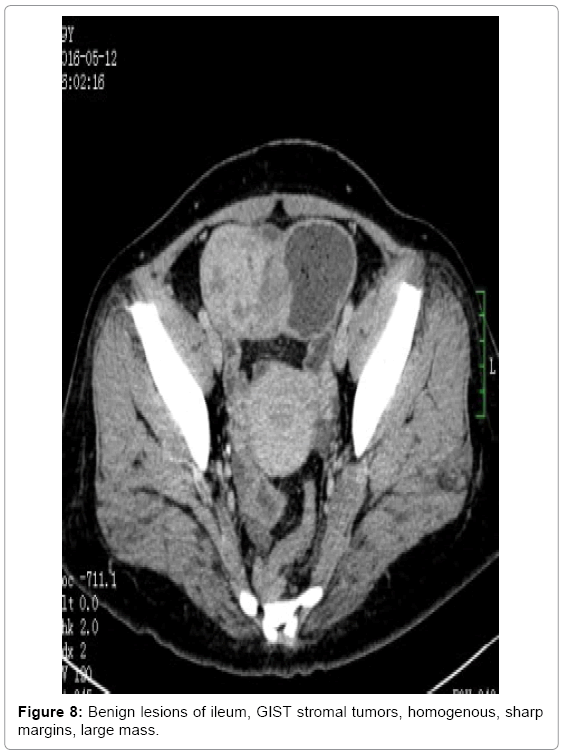
Figure 8: Benign lesions of ileum, GIST stromal tumors, homogenous, sharp margins, large mass.
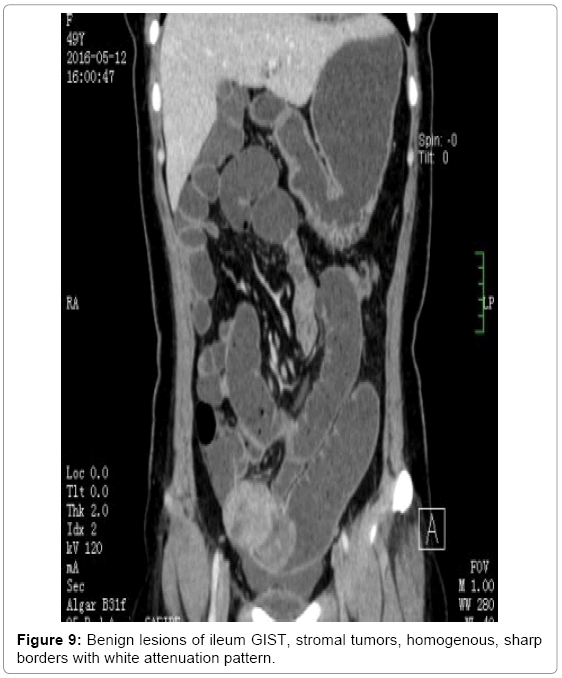
Figure 9: Benign lesions of ileum GIST, stromal tumors, homogenous, sharp borders with white attenuation pattern.
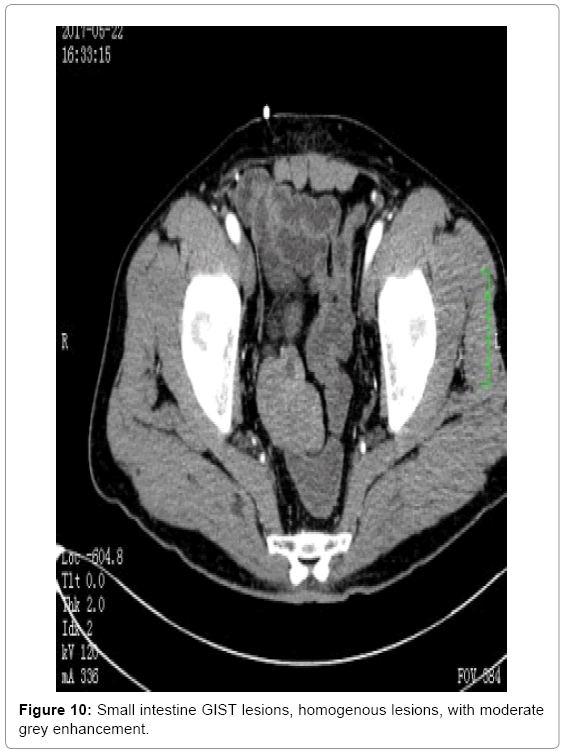
Figure 10: Small intestine GIST lesions, homogenous lesions, with moderate grey enhancement.
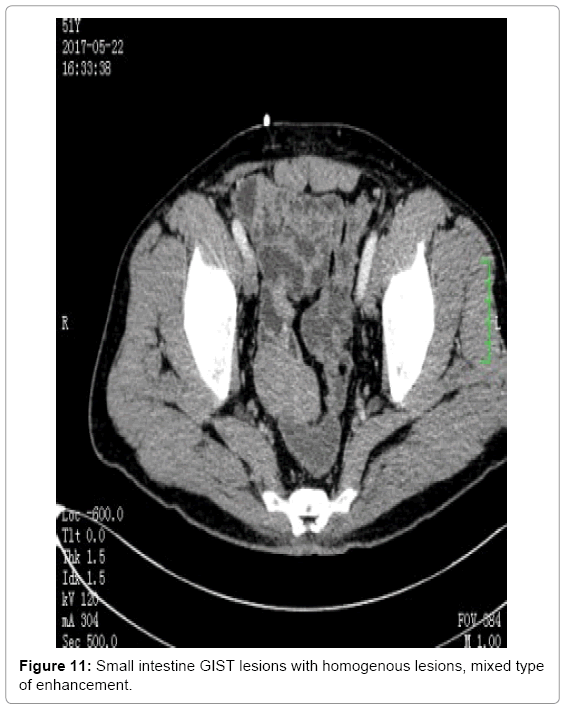
Figure 11: Small intestine GIST lesions with homogenous lesions, mixed type of enhancement.
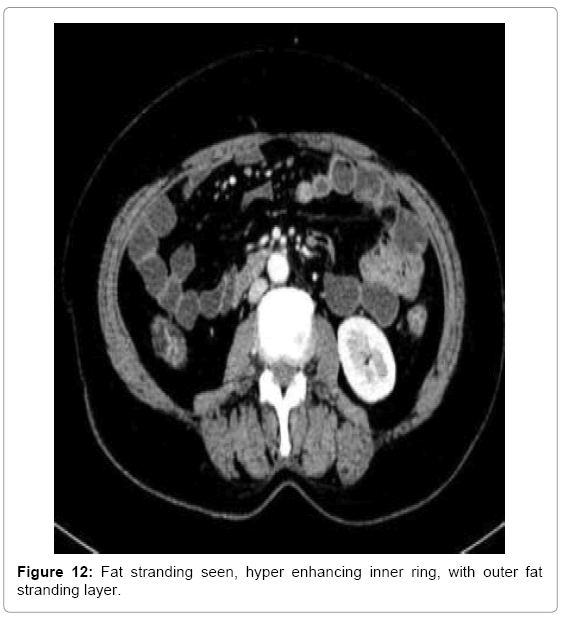
Figure 12: Fat stranding seen, hyper enhancing inner ring, with outer fat stranding layer.
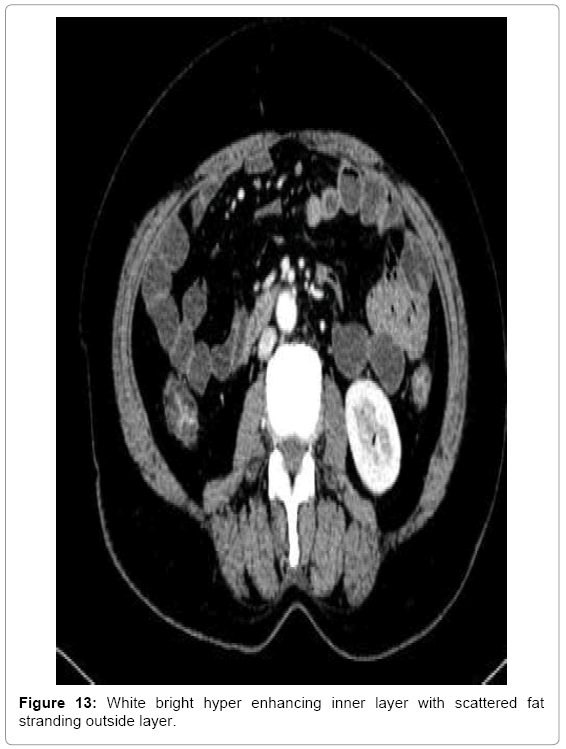
Figure 13: White bright hyper enhancing inner layer with scattered fat stranding outside layer.
From inter quartile range median value of degree of thickness is in between 4 mm-7 mm in benign type of lesion. Here it shows degree of thickness involved is more moderate type in benign lesion (Figures 4-13). While in malignant lesion, median value of degree of thickness is in between 7 mm to 9 mm. Here it shows degree of thickness involved is marked type in malignant lesion.
Thickening of small bowel folds more than 3 mm can be caused by any process that increases the volume of fluid or cells in the submucosal or mucosal region. The critical diagnostic observation is whether the general pattern of the thickening is symmetric or asymmetric. Thickening of small bowel folds, which are perpendicular to the bowel lumen and parallel to neighboring folds, is usually caused by fluid, generally hemorrhage or edema. Irregular thickening of small bowel folds is produced by diseases that infiltrate the bowel wall [1,2].
Symmetric thickening
Any cause of bleeding into the bowel wall can lead to uniform, regular thickening of small bowel folds. The parallel arrangement produces a symmetric, spike like configuration. There usually is segmental involvement, especially of the jejunum. Concomitant bleeding into the mesentery often results in separation of bowel loops and even an eccentric mass simulating malignancy [1,3,4].
Asymmetric thickening
Infiltrative processes causing irregular thickening of small bowel folds may be due to an infection, nonspecific inflammation, or malignancy. Distinguishing among the many diseases that cause this pattern requires an analysis of the site of the lesion, associated radiographic findings, and clinical history [5,6].
Lymphoma shows small bowel involvement together with other small bowel findings it includes isolated or multifocal polypoid masses, circumferential infiltration of bowel wall, and neoplastic involvement of adjacent mesentery and lymph nodes.
Attenuation of the thickened bowel wall
The attenuation pattern of a thickened segment of bowel wall is an important criterion for establishing a differential diagnosis.
Homogeneous attenuation
The diagnosis of a thickened bowel wall that shows homogenous attenuation on CT includes submucosal hemorrhage, infarcted bowel lesions, neoplasm. Submucosal hemorrhage-The diagnosis of submucosal intestinal hemorrhage is evaluated when CT shows circumferential and symmetric bowel wall thickening [7,8]. On CT, most cases of submucosal hemorrhage show homogeneous high attenuation of the thickened segment. In most cases, the small bowel is affected in a segmental distribution [9].
Infarction and ischemia
When the wall is ischemic, it is often circumferentially thickened and may contain a target or halo configuration of attenuation. Chronic Crohn’s disease and chronic radiation enteritis may show homogenous attenuation on contrast-enhanced CT.
Neoplasm
Gastrointestinal neoplasms can present with homogeneous attenuation of the thickened segment on contrast-enhanced CT. In these instances, other criteria (degree; density of lesions; length of involved segment; and associated peri enteric abnormal conditions) are important in establishing the right diagnosis. In cases of neoplasm. Smaller tumors present either as circumferential areas of bowel wall thickening or as asymmetric areas of bowel wall thickening with homogeneous enhancement [10,11].
Important
Malignant lesions can present with homogeneous attenuation of the thickened segment on contrast-enhanced CT. In cases of malignant lesions, homogeneous attenuation correlates with size of the tumor. Thickening of the small bowel wall may be a neoplastic or nonneoplastic condition. Neoplasms are usually short, asymmetric, and they tend to have a chronic onset. In contrast, nonneoplastic small-bowel wall thickening is usually long, uniform, and circumferential, with either an acute onset or a chronic onset. On contrast-enhanced CT scans, the chronic onset diseases, those lesions may have any of three appearances: homogeneous soft-tissue attenuation and enhancing white attenuation pattern or poorly enhancing gray attenuation pattern. Two concentric rings of inner low attenuation and outer high attenuation double halo sign and three concentric rings of high–low–high attenuation the target or “water-halo” sign [12,13]. Double halo is composed of either a higher-attenuation outer annular ring surrounding, other annular ring of gray attenuation. The lower- gray attenuation layer of the water halo sign represent, the edematous or hemorrhagic changes of the submucosa, the amount of fat deposition [14].
Heterogenous
When the attenuation of a thickened bowel wall is heterogeneous, the wall may display a stratified pattern or a mixed pattern of attenuation [15]. The double halo and target signs usually indicate an acute inflammatory or ischemic condition. The finding of stratified attenuation in a thickened segment, is used mainly to exclude malignant conditions.
The water halo sign indicates stratification within a thickened bowel wall that consists of either two or three continuous, symmetrically thickened layers. The water halo sign is most valuable observation of acute bowel wall injury, malignancy rarely manifests water halo sign [12,13].
Differential diagnosis
Common diagnoses with water halo sign include idiopathic inflammatory bowel diseases, vascular disorders, infectious diseases, and radiation damage. This pattern is uncommon in malignancy. The fat halo sign refers to a three-layered target sign of thickened bowel in which the middle or submucosal layer has a fatty attenuation. Common diagnoses with this sign include Crohn disease in the small intestine and idiopathic inflammatory bowel diseases in the colon [16,17]. The deposition of submucosal fat in the large and small bowels has been documented in patients with both acute and chronic inflammatory disorders of the bowel [17]. Although a stratified pattern of attenuation is present with submucosal fat deposition, recognizing the very low attenuation of the submucosa will allow an accurate diagnosis to be established [18,19]. The darker attenuation of intramural fat can usually be visually distinguished from the grayer tone of the water halo sign [7,20,21]. The common diagnoses in which the fat halo sign is seen in Benign lesions which include Crohn disease in the small intestine and ulcerative colitis.
Heterogenous mixed attenuation
In these cases, the grossly thickened bowel wall shows several irregular zones of lower attenuation randomly located adjacent to areas of higher attenuation. The findings are related to ischemia and necrosis and are seen in high grade, poorly differentiated gastrointestinal neoplasms such as adenocarcinoma and stromal cell tumors. Larger tumors frequently undergo central necrosis and will show heterogeneous enhancement on contrast-enhanced scans. The white pattern represents contrast material enhancement that uniformly affects most of the thickened bowel wall. Common diagnoses with this pattern include idiopathic inflammatory bowel diseases and vascular disorders [11,13,22,23]. Absence or decreased enhancement of the bowel wall is the specific finding for bowel ischemia, ischemic segment may also appear with increased enhancement which is caused by altered vascular permeability [13,24]. The increased wall enhancement associated with inflammatory bowel disease reflects the hyperemic and hyper vascular state in acute inflammation. This hypervascularity is reflected in mesenteric changes of vascular dilation and tortuosity [8]. The common diagnoses in which the white attenuation pattern is seen include idiopathic inflammatory bowel diseases and vascular disorders. This pattern is uncommon in malignancy. The gray pattern is defined as a thickened bowel wall with limited enhancement whose homogeneous attenuation is comparable with that of enhanced muscle [25,26]. This pattern is used to differentiate between benign and malignant disease. It is common in both benign and malignant diseases noted that bowel wall thickening of less than 2 cm was more characteristic of benign conditions, whereas thickening greater than 3 cm was usually present in malignant cases. Differential Diagnosis: The gray attenuation pattern and accompanying morphologic characteristics are used in differentiating between benign and malignant disease. Black attenuation is the equivalent of pneumatosis, and this pattern is commonly seen in ischemia, infection, and trauma [27]. It is hard to detect small collections of intramural gas but to avoid confusing them with intraluminal gas collections that attach to the mucosa. In the cases where the gas bubbles are noticed in the cecum and ascending colonic wall, which results due to gas trapped between fecal debris and mucosa [13,26]. Repositioning and rescanning the patient in a decubitus position clears confusion. In each of the five categories of attenuation patterns-white, gray, black, water halo sign, fat halo attenuation patterns are described. Mesenteric calcifications are seen in benign and malignant conditions. Benign mesenteric calcifications may be present in granulomatous lesions such as tuberculosis, sarcoidosis [28,29]. Malignant neoplasms may present on CT with calcifications in the mesentery, which is occasionally seen in patients with treated lymphoma [11,30,31]. Malignant lymphoma of the small bowel tends to be more homogenous and show less contrast enhancement [32,33].
Carcinoid tumor appears as an intramural mass demonstrating increased enhancement due to hyperemia [33-35]. Calcified foci in the mesentery can also be seen in mucinous metastases from ovarian or gastrointestinal neoplasms. Another neoplastic process that can present with a calcified soft-tissue mass in the mesentery is carcinoid tumor [1,36]. Small bowel is often thickened with tethering adjacent loops of bowel toward the calcified central mass.
In bowel lesions, CT with the perspective of morphology, bowel wall thickening, attenuation values, with contrast resolution, enhancement pattern, intensity values HU. CT has surveillance overall bowel lesions can be analyzed with good efficacy. The appearance, degree, and consistency of bowel wall enhancement have been well described. An approach for classifying bowel wall abnormality was presented based on different variations. The classification is most useful in distinguishing benign lesions from malignant lesions. The approach can serve as good stimulus for radiologists to attain positive goal.