Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2016) Volume 5, Issue 3
Background: No previous study has investigated the computed tomography (CT) characteristics of follicular thyroid adenoma (FTA) and follicular thyroid carcinoma (FTC). This study aimed to compare the CT features of FTA and FTC. Methods: Eighty-seven consecutive patients with FTA or FTC that underwent preoperative neck CT from January 2006 to December 2013 were included. In each case, single radiologist retrospectively examined the corresponding neck CT under blinded conditions for the histopathological results. The CT features of FTA and FTC were evaluated, as well as the specific CT features for differentiating FTC from FTA. Results: After matching the CT and histopathological results, 55 FTAs and 25 FTCs in 80 patients were analyzed. No statistically significant differences were detected in patient age, gender, nodular size, or location between FTA and FTC patients. The most common CT features in both FTA and FTC included low attenuation, intraglandular configuration, smooth margin, round shape, absence of calcifications, and inhomogeneous enhancement. In particular, the prevalence of decreased, iso-, and increased enhancement was similar in both FTA and FTC. The prevalence of homogeneous attenuation in FTC was higher, whereas the prevalence of inhomogeneous attenuation in FTA was higher. The logistic regression analysis revealed no significant differences between FTA and FTC in any CT features, except for the pattern of attenuation (p = 0.002). Conclusion: No specific CT features of FTA and FTC were identified, and CT may be unhelpful for distinguishing FTC from FTA.
<Keywords: Thyroid nodule, Follicular neoplasm, Follicular adenoma, Follicular carcinoma, Computed tomography
Follicular neoplasm of the thyroid gland includes Follicular Thyroid Adenoma (FTA) and Follicular Thyroid Carcinoma (FTC). Further, reports have indicated that FTC is the second most common thyroid cancer after papillary thyroid carcinoma [1].
Thyroid follicular neoplasm can be suspected in 15–30% of fineneedle aspiration for thyroid nodules, whereas cytological diagnoses of suspicious thyroid follicular neoplasm represent a heterogeneous group of lesions including benign follicular hyperplasia, FTA, FTC, Hürthle cell neoplasm, and the follicular variant of papillary thyroid carcinoma [2-4].
However, core needle biopsy is not useful for the management of suspicious follicular neoplasm cytology because it does not provide specific information for FTA or FTC [3,5]. In practice, a surgical approach is used to treat most cases of suspicious follicular neoplasm cytology because a non-surgical biopsy does not aid in distinguishing FTA from FTC [5-7]. Despite the publication of several studies regarding the sonographic differentiation of FTA and FTC, no specific sonographic features of FTA or FTC have been reported [8,9]. Consequently, a diagnostic dilemma still exists for thyroid follicular neoplasm.
The numerous advantages of Computed Tomography (CT), including a wide field of view, objectivity, and detailed display of bone or air-containing organs, has led to the frequent use of CT for evaluating various neck lesions, despite its disadvantages including radiation hazard and the use of iodine-based contrast medium [10].
Although CT is not an established imaging modality for evaluating thyroid nodules, it has been used for tumor-node-metastasis staging in thyroid cancer patients [6,10]. In particular, several studies have attempted to identify characteristic CT features of malignant thyroid nodules [11-14].
However, to the best of our knowledge, no previous studies have investigated the specific CT features for differentiating FTC from FTA using detailed CT features and histopathological results. Therefore, the aim of this study was to assess CT features of FTA and FTC, and to determine specific CT features that would enable the differentiation of FTC from FTA.
Study population
The Institutional Review Board approved this retrospective study prior to patient selection, and informed consent was waived. From January 2006 to December 2013, 206 patients (176 women and 30 men; mean age, 49.7 ± 12.3 years; age range, 16–79 years) underwent surgical treatment of thyroid follicular neoplasm. Among them, 87 patients (70 women and 17 men; mean age, 49.9 ± 12.6 years; age range, 20–79 years) underwent preoperative neck CT in our hospital. The exclusion criteria included poor quality of CT images (n = 1), no CT delineation of FTC or FTA (n = 2), and unclear match between CT and histopathological findings (n = 4) due to the presence of one or more thyroid nodules which show similar size and location with the follicular neoplasm. Following application of the exclusion criteria, seven patients (six women and one man; mean age, 52.0 ± 10.0 years; age range, 37–69 years) were excluded from the study. Ultimately, 80 patients (64 women and 16 men; mean age, 49.7 ± 12.8 years; age range, 20–79 years) were included.
Neck CT
Neck CT scans were conducted using a 64-channel multi-detector CT scanner (Aquilion One; Toshiba Medical Systems, Otawara, Japan) with injection of contrast medium (iopamidol [Pamiray 370]; 2.5 mL/s, 40–60 seconds delay, and 2 mL/Kg [a total of 100–130 mL]; Dongkook Pharm., Seoul, South Korea) and with a scan range from the floor of the orbit to the sternum. Non-enhanced axial, contrast-enhanced axial, and contrast-enhanced coronal reformatted CT images were acquired in all cases (slice thickness, 3 mm; reconstruction increment, 3 mm; 250 mA, 120 KVp; 140-300 mA).
Image analysis
A single radiologist with 12 years of experience interpreting head and neck CT scans who was blinded to the histopathological results performed the image analysis in all cases using a picture archiving and communication system. Solid thyroid nodule CT features including the degree and pattern of attenuation, configuration, margin, shape, calcification pattern, and the degree and pattern of nodular enhancement were retrospectively evaluated. The adjacent thyroid parenchyma was used as reference to determine the degrees of attenuation and enhancement of thyroid nodules on non-enhanced and contrast enhanced CT images, respectively. The attenuation patterns of thyroid nodules on non-enhanced CT and enhancement patterns of thyroid nodules on contrast enhanced CT were classified as homogeneous or inhomogeneous. The configuration of the thyroid nodule was divided into intraglandular, which was defined as the presence of thyroid parenchyma between the nodule and adjacent thyroid capsule, expansile, which included a blunt angle between the lesion and adjacent thyroid capsule, or exophytic, which included an acute angle between the lesion and adjacent thyroid capsule. The margin of the thyroid nodules was classified as smooth, irregular (spiculated), lobulated, or poorly defined. The nodular shape was classified based on the ratio of anteroposterior to transverse diameters in axial images. First, the anteroposterior and transverse diameters of the nodule were evaluated for parallel orientation with the anteroposterior and transverse axes of the thyroid gland, respectively (Figure 1). Second, the shape of the thyroid nodules was divided into ovoid (anteroposterior diameter/transverse diameter ratio ≤ 0.8), round (0.8
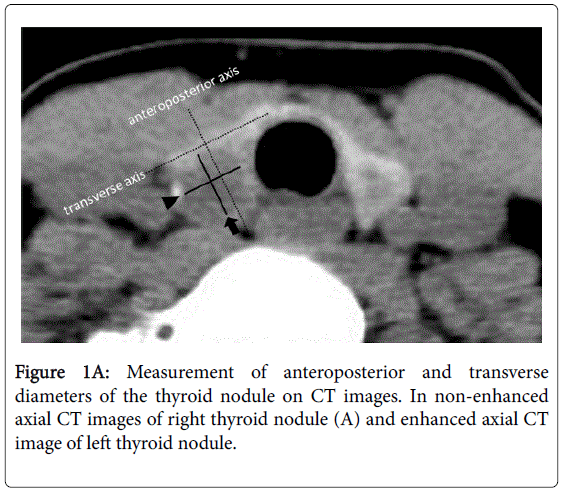
Figure 1A: Measurement of anteroposterior and transverse diameters of the thyroid nodule on CT images. In non-enhanced axial CT images of right thyroid nodule (A) and enhanced axial CT image of left thyroid nodule.
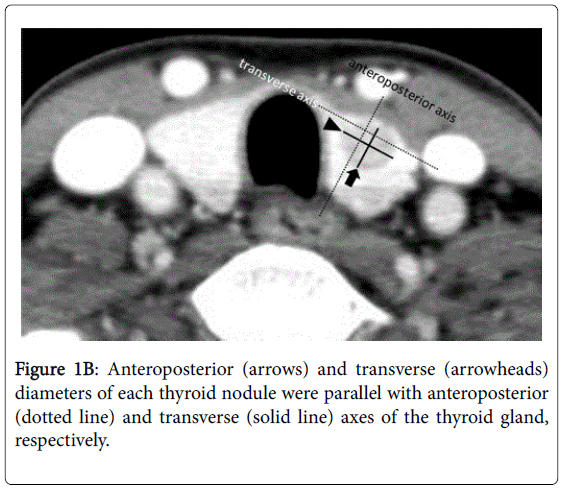
Figure 1B: Anteroposterior (arrows) and transverse (arrowheads) diameters of each thyroid nodule were parallel with anteroposterior (dotted line) and transverse (solid line) axes of the thyroid gland, respectively.
To avoid investigation bias, nodule selection and image analysis were independently performed in two stages:
• First, the selection, localization, and calibration of a thyroid nodule in all patients were performed based on the CT and histopathological findings of thyroid follicular neoplasm.
• After 2 weeks, image analyses of the target thyroid nodules were performed by a single radiologist blinded to the histopathological results. In the case of multiple FTAs or FTCs, the largest FTA or FTC was selected when two or more FTAs or FTCs were found in the same patient.
The data were tested for normal distribution using the Kolmogorov- Smirnov test. Age at the time of diagnosis and size of the nodule were expressed as the mean ± standard deviation (SD). Mean differences in age and size of the nodules between the two groups (FTA versus FTC) were compared using an independent t-test. Group comparisons of categorical variables were performed using the chi-squared (χ2) test. A univariate logistic regression analysis was used to evaluate the initial predictive power of each variable. The clinical and radiologic variables with a high predictive power (p<0.20, Wald test) were selected and incorporated into a multivariate logistic regression analysis to determine the optimal logistic regression model for differentiating FTC and FTA. A Receiver Operating Characteristic (ROC) curve was constructed to determine the diagnostic performance of each CT finding with the largest Az value used for the differentiation of FTC and FTA. All statistical analyses were performed using statistical analysis software (SPSS, version 17.0, SPSS, Chicago, IL, USA; MedCalc, version 9.0, MedCalc Software, Mariakierke, Belgium), and p values less than 0.05 were considered statistically significant.
Among the 80 patients, the reasons for thyroid surgery included suspicious follicular neoplasm cytology (n = 27), coexisting thyroid malignancy (n = 8), malignant cytology (n = 9), atypia of undetermined significance or follicular lesion of undetermined significance in cytology (n = 7), and patient request despite benign cytology (n = 29).
Based on the histopathological results following thyroid surgery, 55 patients (45 women and 10 men; mean age, 48.7 ± 12.2 years; age range, 20–79 years) had FTA (mean diameter, 28.3 ± 16.0 mm; range, 5.1–85.3 mm), and 25 patients (19 women and 6 men; mean age, 51.8 ± 14.0 years; age range, 22–78 years) had FTC (mean diameter, 34.9 ± 26.3 mm; range, 8.5–105.1 mm). Of the 29 patients with benign cytology, 6 had FTC.
Of the 80 patients, a limited number had multiple FTAs (n = 5) and FTCs (n = 1). The types of thyroid surgery in FTA and FTC patients included total thyroidectomy (n = 20 and 14, respectively), subtotal thyroidectomy (n = 5 and 1, respectively), and hemithyroidectomy (n = 30 and 10, respectively). The locations of FTA and FTC patients were right (n = 33 and 15, respectively), left (n = 22 and 9, respectively), and isthmus (n = 0 and 1, respectively).
There were no statistically significant differences in patient age (p = 0.317), gender (p = 0.546), size (p = 0.173), or location (p = 0.321) of follicular neoplasm between FTA and FTC patients. Of the 25 FTCs, a metastatic regional lymph node was confirmed in only one case.
The results of the analyses of FTA and FTC CT features are presented in Table 1. The most common CT features in both FTA and FTC included low attenuation, intraglandular configuration, smooth margin, round shape, absence of calcifications, and inhomogeneous enhancement (Figures 2 and 3). In particular, the prevalence of decreased, iso-, and increased enhancement was similar in both FTA and FTC. The prevalence of inhomogeneous attenuation was higher in FTA, whereas the prevalence of homogeneous attenuation was higher in FTC. However, no statistically significant differences in FTA and FTC CT features were detected, except for the pattern of attenuation (p = 0.019). Further, the logistic regression analysis revealed no significant differences between the FTA and FTC CT features, except for the pattern of attenuation (p = 0.002; Table 2).
| Follicular thyroid adenoma (n = 55) |
Follicular thyroid carcinoma (n = 25) |
P value | |
|---|---|---|---|
| Degree of attenuation | 0.497 | ||
| Low | 54(98.2) | 25(100) | |
| iso- | 0(0) | 0(0) | |
| High | 0(0) | 0(0) | |
| Cystic | 1(1.8) | 0(0) | |
| Pattern of attenuation | 0.019 | ||
| homogeneous | 24(43.6) | 18(72) | |
| inhomogeneous | 31(56.4) | 7(28) | |
| Configuration | 0.698 | ||
| intraglandular | 34(61.8) | 13(52) | |
| expansile | 18(32.7) | 10(40) | |
| exophytic | 3(5.5) | 2(8) | |
| Margin | 0.073 | ||
| Smooth | 49(89.1) | 19(76) | |
| irregular (spiculated) | 2(3.6) | 0(0) | |
| lobulated | 3(5.5) | 6(24) | |
| poorly defined | 1(1.8) | 0(0) | |
| Shape | 0.670 | ||
| Ovoid | 7(12.7) | 5(20) | |
| Round | 33(60) | 13(52) | |
| taller-than-wide | 15(27.3) | 7(28) | |
| Calcifications | 0.814 | ||
| None | 41(74.5) | 17(68) | |
| rim (eggshell) | 1(1.8) | 1(4) | |
| Nodular | 10(18.2) | 5(20) | |
| Punctate | 2(3.6) | 2(8) | |
| mixed* | 1(1.8) | 0(0) | |
| Degree of enhancement | 0.762 | ||
| no/scant | 2(3.6) | 0(0) | |
| decreased | 22(40) | 9(36) | |
| iso- | 15(27.3) | 8(32) | |
| increased | 16(29.1) | 8(32) | |
| Pattern of enhancement | 0.612 | ||
| homogeneous | 9(16.4) | 3(12) | |
| inhomogeneous | 46(83.6) | 22(88) |
Table 1: Analysis of computed tomography features of follicular neoplasm in 80 patients. Mixed means punctate plus nodular calcifications. Data are number of items, with percentage in parentheses.
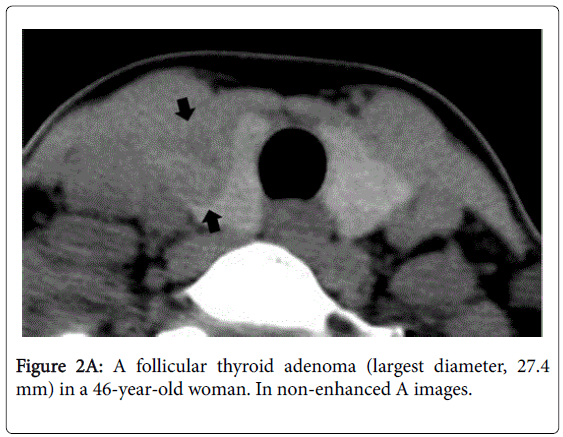
Figure 2A: A follicular thyroid adenoma (largest diameter, 27.4 mm) in a 46-year-old woman. In non-enhanced A images.
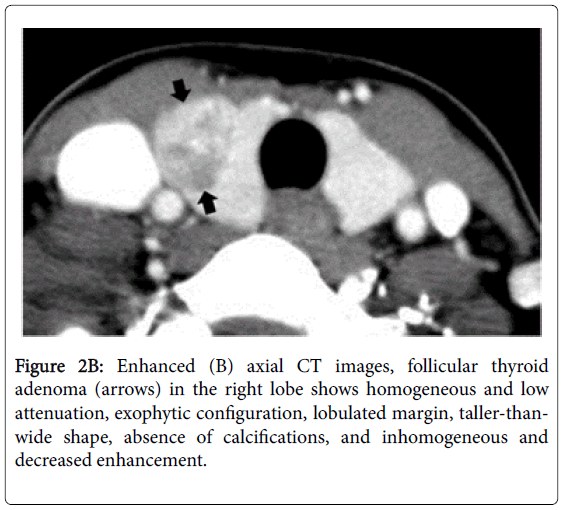
Figure 2B: Enhanced (B) axial CT images, follicular thyroid adenoma (arrows) in the right lobe shows homogeneous and low attenuation, exophytic configuration, lobulated margin, taller-thanwide shape, absence of calcifications, and inhomogeneous and decreased enhancement.
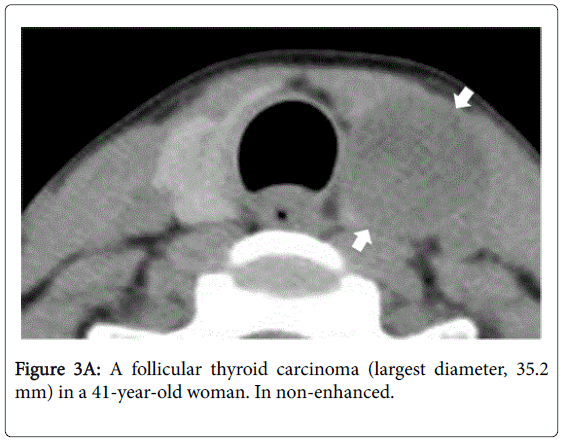
Figure 3A: A follicular thyroid carcinoma (largest diameter, 35.2 mm) in a 41-year-old woman. In non-enhanced.
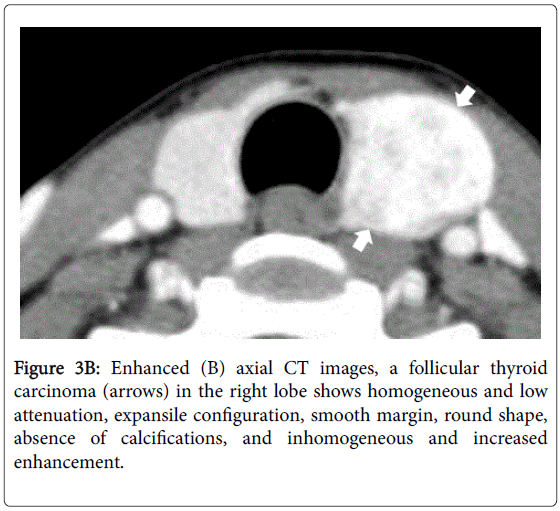
Figure 3B: Enhanced (B) axial CT images, a follicular thyroid carcinoma (arrows) in the right lobe shows homogeneous and low attenuation, expansile configuration, smooth margin, round shape, absence of calcifications, and inhomogeneous and increased enhancement.
| CT features | Odds Ratio* | P value |
|---|---|---|
| Degree of attenuation | NA | |
| Pattern of attenuation | 0.10 (0.02, 0.42) | 0.002 |
| Configuration | 1.85 (0.74, 4.64) | 0.190 |
| Margin | 2.10 (0.97, 4.56) | 0.061 |
| Shape | 0.72 (0.31, 4.67) | 0.448 |
| Calcifications | 1.49 (0.87, 2.53) | 0.146 |
| Degree of enhancement | 1.00 (0.52, 1.94) | 0.995 |
| Pattern of enhancement | 4.23 (0.75, 23.88) | 0.103 |
Table 2: Multivariate logistic regression analysis of CT features for differentiating follicular thyroid carcinoma from follicular thyroid adenoma: Numbers in parentheses are 95% confidence intervals. NA = not available (values are not presented for factors that were not included or found to be insignificant in multivariate analysis).
Significant differences in FTA and FTC CT features were further analyzed using a ROC curve analysis, and the sensitivity, specificity, positive predictive value, and negative predictive value of the individual CT features are presented in Table 3. However, no CT features exhibited both high sensitivity and specificity.
| CT features | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Azvalue* | P value |
|---|---|---|---|---|---|---|
| Degree of attenuation | 100 | 1.8 | 30.8 | 100 | 0.509 | 0.317 |
| Pattern of attenuation | 72 | 56.4 | 42.9 | 81.6 | 0.642 | 0.013 |
| Configuration | 48 | 61.8 | 36.4 | 72.3 | 0.551 | 0.409 |
| Margin | 24 | 92.7 | 60 | 72.9 | 0.568 | 0.167 |
| Shape | 20 | 87.3 | 4.7 | 70.6 | 0.523 | 0.721 |
| Calcifications | 32 | 74.5 | 36.4 | 70.7 | 0.532 | 0.577 |
| Degree of enhancement | 64 | 43.6 | 34 | 72.7 | 0.542 | 0.521 |
| Pattern of enhancement | 88 | 16.4 | 32.4 | 75.0 | 0.522 | 0.600 |
Table 3: Diagnostic performance of CT features for differentiating follicular thyroid carcinoma from follicular thyroid adenoma. Az means the largest area under the receiver operating characteristic (ROC) curve. PPV, positive predictive value; NPV, negative predictive value.
Thyroid nodules are often detected incidentally following neck CT. Based on previous studies, the malignancy rate of such incidentaloma ranges from 3.9% to 13.3% [11-14]. However, no specific CT features that can reliably distinguish malignant from benign thyroid lesions have been identified [11]. Consequently, it is still unclear whether CT aids the diagnosis of thyroid incidentaloma. Recently, one study demonstrated that the most common CT features for papillary thyroid carcinoma included homogeneous low attenuation, a taller-than-wide shape, absence of calcifications, and homogeneous decreased enhancement [15]. In the present study, the most common CT features of both FTA and FTC included low attenuation, intraglandular configuration, smooth margin, round shape, and absence of calcifications. In particular, the prevalence in the nodular shape and enhancement degree and pattern were different from the previous study for papillary thyroid carcinoma (Figure 2).
To date, no useful imaging or biopsy method for differentiating FTA from FTC has been established [5-7,16]. Thus, many cases of suspicious follicular neoplasm cytology are treated surgically. Although several studies have investigated CT features of malignant thyroid nodules [11-14], no previous studies have attempted to differentiate FTA from FTC (Figure 3).
In the present study, attempts were made to investigate the specific CT features of FTA and FTC in patients who underwent preoperative neck CT and thyroid surgery for FTA or FTC. The prevalence of decreased, iso-, and increased enhancement was similar in both FTA and FTC. In particular, the prevalence of homogeneous attenuation was higher in FTC, whereas inhomogeneous attenuation was higher in FTA. However, no specific CT features reliably distinguished FTA from FTC.
In the present study, a specific CT evaluation of nodular shape was conducted. The basic concept in nodular shape analysis is that the measurement condition on CT should be the same as ultrasonography conditions. On thyroid ultrasonography, anteroposterior and transverse diameters of the nodule are parallel with anteroposterior and transverse axes of the thyroid gland, respectively [17]. In a recent CT study of papillary thyroid carcinoma [15], the assessment of nodular shape revealed a significant difference between ultrasound and CT, but the nodular shape evaluation method in CT was different from the present study. In addition, the present study did not involve the measurement of longitudinal diameter of thyroid nodules.
Our study had several limitations. First, a single radiologist performed the analysis of the CT images and subjectively determined the nodular attenuation and degree of nodular enhancement. Second, there were varying degrees of CT attenuation artifacts from the clavicle, which were not considered. Third, in cases that involved multiple FTAs or FTCs, only one dominant follicular neoplasm for each lobe was selected. Fourth, the possibility of underlying diffuse thyroid disease that, if present, might have affected the analysis of CT features was not considered. Finally, a combination analysis of individual CT features for differentiating FTA from FTC was not performed.
In conclusion, the study results demonstrated that the most common CT features in both FTA and FTC included low attenuation, intraglandular configuration, smooth margin, round shape, absence of calcifications, and inhomogeneous enhancement, and that the prevalence of homogeneous attenuation was higher in FTC, whereas the prevalence of inhomogeneous attenuation was higher in FTA. However, no specific CT features of FTA and FTC were identified. Therefore, CT may be unhelpful for distinguishing FTC from FTA.