Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2012) Volume 1, Issue 2
Branchial cysts are the most frequent both congenital abnormalities and cysts in the neck. We present the case of an adult man who come to the clinical observation after the sudden onset of swelling of 14 cm at the II LEVEL A, without general symptoms. Clinically, the lesion presented with smooth margins, well-defined limits, tense-elastic, non-tender upon palpation nor spontaneously, moving on planes both above and below. The U. S. CT and MR study confirmed the cystic nature of the lesion (may be a lymphangioma). After its removal histological examination diagnosed an infection of the branchialarch cysts
<Keywords: Second branchial cleft cyst; Diagnosis; Treatment; Surgical notes
A 35 year old man presented to clinical observation after onset of a sudden swelling of left second lateral cervical level. Shortly, this lesion reached a size of 14 x 7 cm (Figure 1). The volume increase was accompanied by an inflammatory reaction that at the time of clinical observation was not present. The patient never presented any general symptoms. Clinically, the lesion presented with smooth margins, well-defined limits, tense-elastic, non-tender upon palpation nor spontaneously, moving on planes both above and below. The ultrasound diagnosed a cystic lesion with peripheral vascularity with some intracystic septums at the inferior pole, as well as intimate relationship with the carotid, The MRI and CT scan show a novel morphology expansive lesion of 48 x 38 x 54 (Figure 2, Figure 3), situated along the anterior margin of the sternocleidomastoid muscle, which is marked, the upper pole joins with the horizontal ramus of the mandibular angle which also comes in contact with the lower pole of the parotid gland, the subman dibular glandis anterior-medially displaced. Its till has a thin fat plane of cleavage that displaces the carotidspa cemedially, the tumor appears with polycyclicmargins, multi-lobulated for the presence of multiple cystic which are marked lyhyper intense on T2contents as fluid, with thin walls, with thin septa and context mild impregnation in the contrast phase. There is also a solid nodule about 2 cm in the lower third which in stead presents significant enhancement post-contrast that is likely attribute a bletoa vascular component. About the nature of the lesion it's compatible with lymphangio main the first case, but it's in the differential diagnosis with branchial cleft cysts. After what was found from the imaging studies, a surgical removal of the lesion was suggested. During surgery (Figure 4) the mass appeared to be composed of a thick wall, multi-lobulated, and filled with purulent liquid (Figure 5). Treatment of branchial cysts is surgical removal. The incision is slightly concave, or horizontal for aesthetic reasons. When we prepare the top flap, the incision of the superficial fascia and platysma muscle is necessary in order to carefully protect the man dibular branch of the facial nerve. The separation of cysts from the front edge of the sternocleidomastoid muscle should be done carefully because it is possible to meet the accessory spinal nerve or its branches. The external and the anterior jugular vein can be tied and cut if necessary, as well as the sensitive nerve endings that cross the incision line. The facial vein can be cut or preserved. When dissecting the posterior and deep wall of the cyst from the front surface of the carotid sheath we can see crosses the hypoglossal loop, this nerve should not be isolated but only recognized and preserved. When dissecting the top of the cyst it is possible to cross the hypoglossal nerve in contact with the belly of the digastric muscle, the vein or veins of the tongue, and it is also possible to cross the inferior glossopharyngeal nerve that at this level can give branches to the pharynx (Figure 6). In the third type of lesion the "tail" of the cyst must be followed between the external and internal carotid artery (paying attention to the superior laryngeal nerve that passes through them), deep to the posterior belly of digastric and stylus hyoid. Ligature and division cysts and after a careful hemostasis, placement of a suction drain. Suture of platysma and the skin on separate planes. Histological examination diagnosed an infection of the branchial arch cysts. The culture of the pus isolated Streptococcus Pneumoniae.
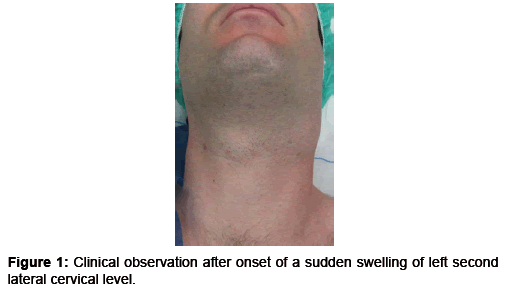
Figure 1: Clinical observation after onset of a sudden swelling of left second lateral cervical level.
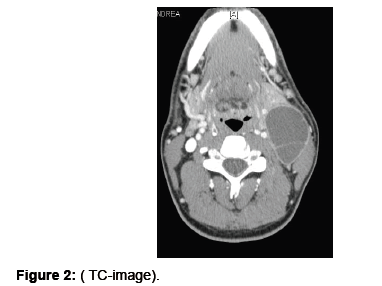
Figure 2: ( TC-image).
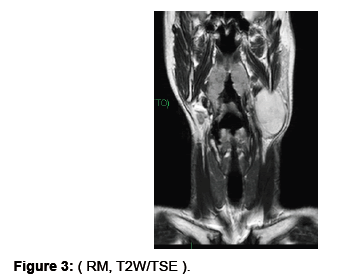
Figure 3: ( RM, T2W/TSE ).

Figure 4: Lesion with thick wall, multi-lobulated, and filled with purulent liquid.
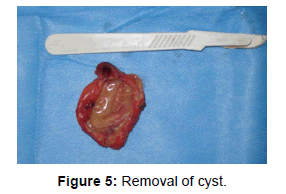
Figure 5: Removal of cyst.
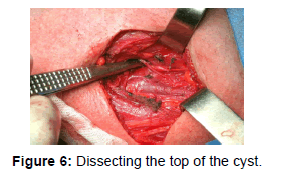
Figure 6: Dissecting the top of the cyst.
Branchial cysts are the most frequent both congenital abnormalities and cysts in the neck. The anomalies of the second branchial cleft are the most common apparatus branchial anomalies, representing approximately 95% of cases [1,2]. The branchial apparatus begins to develop during the second week of gestation and the formation is completed between the sixth and seventh week of fetal life, and probably in this period may be some alterations in the maturation process that lead to the abnormalities of the branchial apparatus [3]. Several theories on the formation of branchial apparatus abnormalities (cervical thymus-pharyngeal theory, the included theory [4]) have been developed, but the most accepted theory is the evolution of the incomplete branchial apparatus [5]. Branchial cysts have equal prevalence in both sexes, and the average age at diagnosis is between the second and fourth decade [6-8] and only 2-3% of cases are bilateral and rare lymultiple [9]. Branchial apparatus anomalies are distinguished according to the classification of Bailey / Proctor anomalies in the first branchial cleft, the second branchial cleft, and the third cleft and fourth branchial cleft. The first branchial cleft anomalies are divided into type I cyst within the parotid with a presentation at a young age, type II are present in the front triangle of the neck communicating with the external auditory canal and development in childhood. The second branchial cleft anomalies are divided into: Type I: localized between the platysma and anterolateral surface of the sternocleid omastoid; type II along the anterior surface of the sternocleidomastoid muscle lateral to the carotid space and posterior to the submandibular glands, originating from the space including between the skin and the ipsilateral tonsil; type III are between the internal carotid and the external carotid artery, the presence of a "tail" of the cyst between these two vessels is pathognomonic of type III cysts [10-12]. Type IV: originate from the pharyngeal mucosa, deeply compared to the palatine tonsils and often can reach the base of the skull [12]. The anomalies of the third and fourth branchial cleft are rare and they are localized at the lower third of the neck [13]. The second branchial cleft cysts are often located between the first and second third of the front surface of the sternocleidomastoid muscle.
Branchial cysts can have two types of clinical presentations: a lump with well-defined margins and limits, mobile on the plans above and below, with a slow-growing volume, asymptomatic, which leads to late diagnosis, or a sudden growth of a lesion unrecognized due to infection of the cyst, with all the signs of local inflammation, that may form a empyema with fistula that can create fistulas in contiguous structures.
Ultrasound examination is helpful in diagnosis because it is cheap, easily repeatable, non-invasive, even if it doesn't allow differential diagnosis with other cystic lesions of the neck (primary or secondary lymph node malignant disease subject to central necrosis, lipoma, teratoma, parotid cancer, lymphangioma, hemangioma, jugular glomus tumors, paragangliomas, thyroglossal duct cyst, tuberculous lymphadenitis, dermoid cysts, glomus tumors, carotid neurofibromas [14-16]. Undoubtedly, CT scan contrast and MRI with contrast add basic information about the volume, relations with neighboring structures and the nature of the lesion, allowing to formulate the most appropriate surgical strategy to minimize complications [17,18]. The FNAC of cystic lesions may be diagnostic but can't define the nature of the lesion, even though they often are not able to make a specific diagnosis of the inflamed cystic lesion [19].
A good preoperative study using imaging allows the preparation of an operative strategy aimed at the complete removal of the lesion and to reduce surgical complications. In the case of infected cysts it is necessary to subject the patient to anti-inflammatory and antibiotic therapy, and after four weeks it is possible to perform the surgery, burdened by the formation of post-inflammatory fibrotic tissue [5].
Over time, other surgical treatments have been proposed as an intraoral resection [20] or endoscopic [21], without any success.
Before suggesting surgery, the second branchial cleft cysts in adults must be well studied. The pre-operatory plan consists of clinical evaluation, US, CT, MRI and FNAC that allows to program a correct preoperative strategy and surgical tactics, in order to completely eradicate the lesion and prevent injury to neighboring nerve and vascular structures.