Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Case Report - (2018) Volume 6, Issue 3
Aim: Epinephrine infusions are often used in intensive care and cardiac surgical applications. Major hemodynamic responses to epinephrine have been described and include changes in vascular tone, heart rate and myocardial contractility. Arrhythmias seen in acute coronary syndromes and myocardial infarction cases are bradyarrhythmias and tachyarrhythmias. Case: A 78-year-old woman was admitted to our hospital due to emergency chest pain. The patient was hospitalized with coronary intensive care with myocardial infarction without ST elevation. The patient developed ventricular fibrillation (VF) in coronary intensive care unit and underwent coronary angiography in emergency conditions. The patient who entered VF three times during the procedure was defibrillated. In coronary intensive unite lots of VF occurred. Arrhythmia could not be controlled with routine medical treatment. It was seen that the patient's VF initiation was after ventricular extra systole (VES). RonT was evaluated as a phenomenon. Epinephrine 5mg was administered intravenously to the patient who had undergone uncontrolled arrhythmia. VF was controlled then. Discussion: Beta blockers, amiodarone, and nifekalant (a pure Ikr blocker) have been shown to be effective in suppressing ESs during an acute MI. There have been several reports in which a stellate ganglion block and renal sympathetic nerve ablation may have been effective in suppressing the ES. When an ES could not be suppressed by drug therapy and cardiac support devices, catheter ablation procedures have occasionally been applied to rescue patients. A ventricular premature complex (VPC) triggering polymorphic VT or VF is one of the targets of the ablation. We have not received any response to routine medical treatment in our own case. The adrenalin infusion has depressed ES by suppressing VES with tachycardia.
Keywords: Myocardial infarction; Atherosclerosis; Arrhythmias; Electrical storm; Epinephrine
Aim
Atherosclerotic heart disease is the most common cause of mortality and morbidity in all populations [1]. The overall mortality rate in acute MI (myocardial infarction), including deaths in the hospital, is over 30%. In-hospital mortality in acute MI patients is primarily due to either circulatory failure due to severe left ventricular failure or one of the MI complications. These complications are classified as mechanical, electrical or arrhythmic, ischemic, embolic or inflammatory (such as pericarditis). Arrhythmias seen in acute coronary syndromes and myocardial infarction cases are Bradyarrhythmias and Tachyarrhythmias. The incidence of Bradyarrhythmias such as sinus node dysfunction, Sino-atrial transmission anomalies, high-grade AV block and/or branch block is between 0.3% and 18% [2]. Sudden cardiac death in 50% of acute MIs can be seen as the onset symptom of coronary artery disease, due to ventricular tachycardia (VT), ventricular fibrillation (VF), and ventricular flutter [3,4]. Electrical storm (ES) is defined as three or more episodes of ventricular fibrillation (VF) or ventricular tachycardia (VT) within 24 hours and is associated with an increased cardiac and all-cause mortality. One of the major causes of mortality in acute coronary syndrome is fatal arrhythmias.
Case
A 78-year-old woman was admitted to our hospital due to emergency chest pain on 10th of December 2017. Nonspecific changes were detected in the ECG of the hospital emergency department. Troponin I 1.9% (0.00-0.04) and CKMB 6.9% (0.6-6.3) were measured in the laboratory tests performed on the patient. The patient was hospitalized with coronary intensive care with myocardial infarction without ST elevation (Figure 1). Antiaggregant therapy was initiated and intravenous hydration was initiated in patients with high levels of creatinine. Patient creatine level was 1.8 mg/dl (0.6 mg/dl -1.3 mg/dl) and urea level was 110 mg/dl (10 mg/dl-50 mg/dl). Patient without chest pain was decided to treat with medical therapy not invasive therapy. The patient developed ventricular fibrillation (VF) in coronary intensive care unit and underwent coronary angiography in emergency conditions. Left main coronary artery and left anterior descending artery stent implantation was performed and full openness was achieved in the patient (Figures 2 and 3). The patient who entered VF three times during the procedure was defibrillated. In coronary intensive unit lots of VF occurred. It is defined as electrical storm. The patient with respiratory arrest was entrained. Amiodarone infusion was opened to the patient frequently entering VF. In those patients whose arrhythmia could not be controlled, infusion of Magnesium sulfate, Metoprolol and potassium was given. Her potassium level was 3.5 mmol/l (3.5 mmol/l-5.5 mmol/l). It was seen that the patient's VF initiation was after ventricular extra systole (VES). RonT was evaluated as a phenomenon. Epinephrine 5 mg was administered intravenously to the patient who had undergone uncontrolled arrhythmia. VF was controlled then. Approximately 5 minutes to 10 minutes after ES started again, epinephrine infusion started (0.5 mcg.kg-1.min-1). After the infusion was switched on, the arrhythmia was under control. Two days later our patient developed acute renal failure. Our patient who had hypotensive status had exitus.
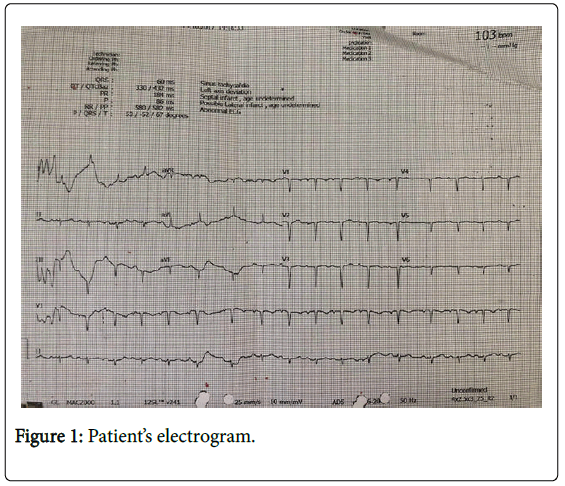
Figure 1: Patient’s electrogram.
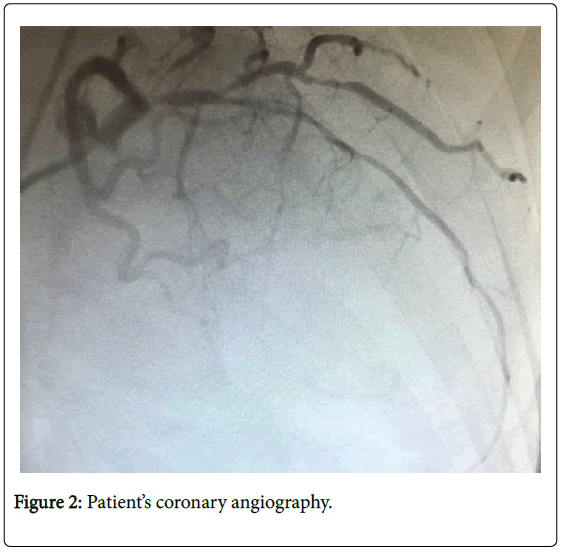
Figure 2: Patient’s coronary angiography.
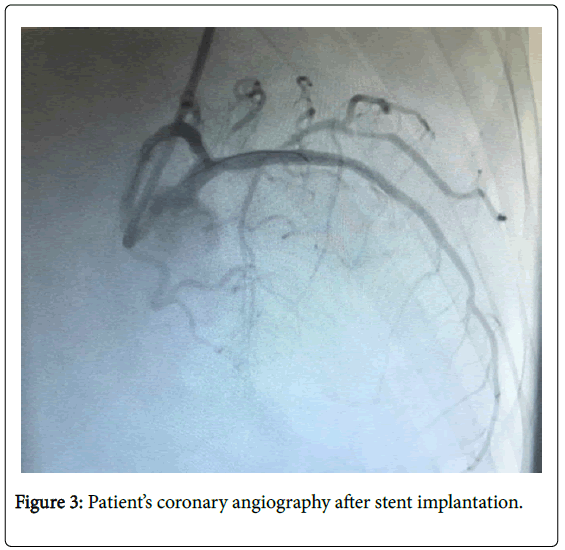
Figure 3: Patient’s coronary angiography after stent implantation.
Acute Coronary Syndrome (ACS) could lead to transient myocardial ischemia and infarction and result in lethal ventricular arrhythmias [5,6]. Patients with ACS are re-vascularized to cure ES [7]. Lethal ventricular arrhythmias could be decreased by coronary vasodilators based on pathogenetic mechanisms of ACS [5]. Both calcium channel blockers and nitrates are the guideline medicine for relaxing vascular smooth muscle and preventing ACS [8]. However, ACS in some patients showed less response to these drugs so that lethal ventricular arrhythmias cannot be suppressed. Beta blockers [8], amiodarone [9] and nifekalant (a pure Ikr blocker) [10] have been shown to be effective in suppressing ESs during an acute MI. There have been several reports in which a satellite ganglion block and renal sympathetic nerve ablation may have been effective in suppressing the ES [9-13]. When an ES could not be suppressed by drug therapy and cardiac support devices, catheter ablation procedures have occasionally been applied to rescue patients [14,15]. In that case, a ventricular premature complex (VPC) triggering polymorphic VT or VF is one of the targets of the ablation. We have not received any response to routine medical treatment in our own case. The adrenalin infusion was depressed electrical storm by suppressing VES with tachycardia.
The rate of mortality in patients with electrical storms is very high and cannot be suppressed by routine treatment.