Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2014) Volume 2, Issue 6
Introduction: Myelofibrosis is characterized by bone marrow fibrosis, cytopenias and extramedullary hematopoiesis. Ruxolitinib is a Janus Kinase-2 inhibitor recently approved for myelofibrosis. In the Philippines, it was made available through the compassionate use program.
Methods: This is a multicentre, retrospective case series of eleven patients in the compassionate use program and eleven age-matched historical controls on best available therapy.
Results: The median age was 54.5+7.33, 82% females. Using the International Working Group on Myelofibrosis Research and Treatment (IWG-MRT) consensus criteria of 2013, 1 out of the 11 patients had both spleen response and anemia response, achieving transfusion independence for > 12 weeks. Nine patients experienced clinical improvement specifically spleen response. Decrease in spleen size was seen in the first 3 months of ruxolitinib use with a mean of 53.5% from baseline. Hematologic toxicities were anemia and thrombocytopenia while nonhematologic were gastrointestinal disorders 5(45%) and hepatic dysfunction 4(36%). These patients were matched by age with historical controls on best available therapy. There was a remarkable decrease in spleen size with ruxolitinib (53.5%) compared to BAT group (18% from baseline). Thrombocytopenia and anemia occurred more frequently in the ruxolitinib group.
Conclusion: Ruxolitinib is a viable treatment option for Intermediate-2 to high risk myelofibrosis with massive splenomegaly. Anemia and thrombocytopenia were common hematologic toxicities during therapy.
Keywords: Myelofibrosis; Compassionate use; Ruxolitinib; Myeloproliferative neoplasm
The term myelofibrosis (MF) refers to primary MF and the phenotypically overlapping conditions that develop as usually in the late evolution of either polycythemia vera (post-polycythemic myelofibrosis) or essential thrombocytosis (post-thrombocythemic myelofibrosis). It is more than a century old disease that was first described by Hueck in 1879, and was included in the group of myeloproliferative disorders in 1951. Primary myelofibrosis is diagnosed using the 2008 World Health Organization criteria. Diagnosis requires meeting all three major criteria and 2 minor criteria. The major criteria are as follows: 1) megakaryocyte proliferation and atypia accompanied by either reticulin and/or collagen fibrosis, or in the absence of reticulin fibrosis, the megakaryocyte changes must be accompanied by increased marrow cellularity, granulocytic proliferation and often decreased erythropoeisis; 2) not meeting WHO criteria for CML, PV, MDS or other myeloid neoplasm; 3) demonstration of JAK2V617F or other clonal marker or no evidence of reactive marrow fibrosis. The minor criteria include leukoerythroblastosis, increased serum lactate dehydrogenase (LDH), anemia and palpable splenomegaly. It is the most heterogeneous disease in the group when it comes to patient characteristics and natural history of the illness [1-3].
The only therapeutic option with curative intent is allogeneic stem cell transplant while all other options are mostly symptomatic. Stem cell transplantation is beyond the reach of most of our patients and because of this, there is a constant search for medical therapeutic options that would improve patients’ symptoms. The association of this disease to a specific mutation known as JAK-2 (V617F) has been the target of scientific research in the early 21st century, hence the discovery of JAK-2 inhibitor. Ruxolitinib, a non-selective Jak-2 inhibitor is not yet available in the Philippines but through the Compassionate-Use-Program, eleven (11) Filipino patients with myelofibrosis were able to use it. It is the aim of this study to describe the demographic profile, clinical profile, treatment response and adverse effects experienced by Filipino patients with myelofibrosis on ruxolitinib under the compassionate use program and compare them with age-matched controls on best available therapy.
This is a multicentre, retrospective cohort study of patients with myelofibrosis given ruxolitinib under the compassionate use program. The compassionate use program opened in June 2011. The aim was to make ruxolitinib available to myelofibrosis patients here in the Philippines and gain preliminary clinical experience on its use. Hematologists from different institutions endorsed their patients with myelofibrosis for approval to the said program. Inclusion criteria were the following 1) male or female patients aged ≥18 years of age, 2) diagnosed with PMF, PPV-MF or PET-MF, according to the 2008 World Health Organization criteria, irrespective of JAK2 mutation status, 3) IPSS classification-high risk (≥3 prognostic factors) ; or intermediate risk level 2 (≥2 prognostic factors) ; or, intermediate risk level 1 (1 prognostic factor) with an enlarged spleen, 4) patients should have adequate liver and renal function, 5) ECOG score of 0, 1, 2 and 6) patients must have recovered or stabilized sufficiently from adverse drug reactions associated with prior treatments before beginning treatment with ruxolitinib. Exclusion criteria to the program were as follows; 1) those who have inadequate bone marrow reserve (ANC<1000, platelet count <100,000), 2) pregnant and lactating women, 3) Patients who have gastrointestinal diseases (IBD, crohn’s disease), cardiac diseases (heart failure/angina), or any coagulopathy, active bacterial, fungal or viral infection, 4) patients who received investigational drug within 30 days and those who have hypersensitivity to JAK inhibitors or any of its excipients. Once approved, they were given protocol guidelines for the use of ruxolitinib. Sample size for this study was not computed, it was limited by the total number of patients included in the compassionate use program. All eleven (11) patients who received ruxolitinib were included and were monitored with weekly to monthly complete blood count and spleen size. Attending hematologists were asked to provide information on disease characteristics, treatment history, spleen size, complete blood count, as well as the ruxolitinib dose adjustments and adverse events (AE). These data were collated using the standardized case report form.
The patients given ruxolitinib were matched by age with historical controls given best available therapy. Criteria for historical controls were as follows: 1) 18 years old and above, male or female, 2) diagnosed MF, post-PV MF, or post-ET MF, 3) patients on best available therapy which includes treatment with any commercially available medications for myelofibrosis (as monotherapy or in combination), 4) a palpable spleen 5 cm or more below the costal margin, 4) no signs of transformation to acute leukemia, 5) and at least a monthly follow-up visit for at least one year. There were a total of 22 patients from ruxolitinib group and best available therapy group. All patients gave informed consent for the review and analysis of medical data. The study was initiated after evaluation and approval of the protocol by the institutional review board of the primary site.
Data collection form or case report form (CRF) was designed to standardize the data gathered from the different centers. It consisted of general data, clinical and laboratory data 3 months prior and 3, 6, 9 and 12 months after the initiation of ruxolitinib. Data monitored and recorded include spleen size, hemoglobin level, platelet count, leukocytes count and differential count. Frequency of blood transfusion and the concomitant use of other medications for myelofibrosis were also noted. Outcome measures were based on the International Working Group for Myelofibrosis Research and Treatment (IWG-MRT)-Response Criteria of 2013 [4]. We evaluated the safety issues by recording adverse events during the treatment using the National Cancer Institute Common Toxicity Criteria for Adverse Events (NCI-CTCAE), Version 3 [5].
Patients’ profile A total of 11 patients under the compassionate use program of ruxolitinib received the drug with a total of 125 person-months treatment and observation period. The demographic and clinical characteristics of these patients are presented in Table 1. The median age of the patients in the ruxolitinib group was 54.5+7.33(range, 49-64), 2 (18%) were males, 9 (82%) were females. Eight (73%) have primary myelofibrosis (PMF) while 3 (27%) had developed MF from essential thrombocythemia or polycythemia vera. Majority, 9(82%) had intermediate-2 risk using Dynamic international prognostic scoring system. The presence of mutation in JAK2 gene were seen in 7 (64%) of the patients. Patients had received a median of 2 prior therapies (range 2-4). Most common previous therapies were hydroxyurea 11 (100%), red blood cell transfusions (7, 64%), erythropoietin (2, 18%), androgens (5, 45%) and corticosteroids (6, 55%), and/or interferon-alpha. Regarding the pre-treatment laboratory data, 7 (64%) patients had anemia (Hb<10 g/dl), 2 (18%) leukopenia (<5 × 109/L) and 4 (36%) leukocytosis (>15 × 109/L). Five (45%) patients had thrombocytopenia (platelet count<150 × 109/L) and 11 (100%) patients had palpable splenomegaly, mean 14 cm (range=10-26 cm).
| RUXO (n=11) | BAT(n=11) | |
| Gender (M:F) | 1:4 | 1:1 |
| Median Age | 54.5+/-7.33 | 58+/-8.6 |
| Median disease duration | 3+/-4.56 | 4+/-4.15 |
| Type of MF | ||
| Primary MF | 8 (73%) | 7(64%) |
| Secondary MF (Post-PV and Post-ET) | 3 (27%) | 4(36%) |
| Dynamic Intl prognostic scoring system | ||
| Low | 0 | 0 |
| Int-1 | 0 | 0 |
| Int-2 | 9 (82%) | 8(73%) |
| High | 2 (18%) | 3(27%) |
| JAK 2 status | ||
| Positive | 7 (64%) | 0 |
| Negative | 1 (9%) | 0 |
| Unknown | 3 (27%) | 11(100%) |
| Prior treatments received: (given in combination or alone) | ||
| Transfusion red cells | 8 | 3 |
| EPO | 2 | 0 |
| Androgens | 5 | 7 |
| Steroids | 6 | 6 |
| Hydroxyurea | 11 | 11 |
| IFN-alpha | 1 | 0 |
| Others | ||
| Median Hb | 90 g/L | 100g/L |
| % patients with anemia (<100g/dl) | 7 (64%) | 4 (36%) |
| Median WBC | 9.1 × 109/L | 10×10 9/L |
| % patients with leucocytosis(>15×109) | 4 (36%) | 4(36%) |
| % patients with leucopenia (<5×109) | 2 (18%) | 2(18%) |
| Median plt count | 189×109/L | 206×109/L |
| % patients with thrombocytosis (plt≥450) | 1 (9%) | 1(9%) |
| % patients with thrombocytopenia (plt ≤150) | 5 (45%) | 2(18%) |
| Median spleen size | 14 cm | 15 cm |
| % patients with splenomegaly | 11(100%) | 11(100%) |
Table 1: General Characteristics of the Population, *CI-SR-clinical Improvement-spleen response;** AR-anemia response, ***SD-Stable disease; CAD-coronary artery disease.
Ruxolitinib Dosing
Of the 11 patients, 4 (36%) started with 20 mg BID, while 7 (64%) patients started with 15 mg BID based on their baseline platelet count. From the protocol guideline, dose adjustments should be done for thrombocytopenia and neutropenia. Majority of the patients continued a lower dose (5 mg BID-15 mg BID) from the original or starting ruxolitinib dose due to hematologic toxicity. All eleven patients on ruxolitinib had at least one dose reduction due to anemia and thrombocytopenia (Figure 1).
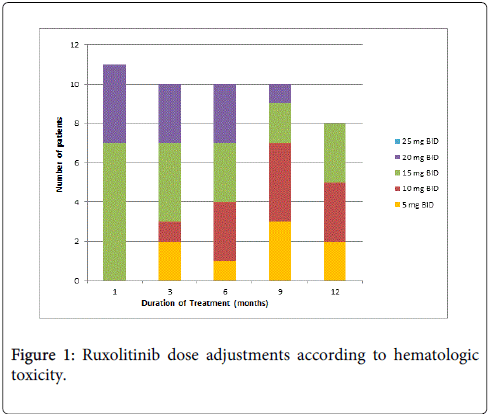
Figure 1: Ruxolitinib dose adjustments according to hematologic toxicity.
Treatment response
According to the International Working Group-Myelofibrosis Research and Treatment 2013 (IWG-MRT) consensus criteria for treatment response in myelofibrosis, 1 out of the 11 patients experienced clinical improvement termed as spleen response and anemia response, wherein there was achievement of transfusion independence of > 12 weeks. After 6 months this patient had leukemic transformation to AML as evidenced by bone marrow myeloblasts of > 20% and is currently back to transfusion requiring state with red cells and platelets. None achieved complete response (CR). Nine patients experienced clinical improvement specifically a spleen response. The remarkable decrease in spleen size was seen in the 1st 3 months of ruxolitinib use with a mean of 53.5% decrease from baseline size. There were some patients who experienced plateau phase but with continued use there was further decrease in spleen size (Table 2 and Figure 2).
| Case | Age/ Sex | MF type | Disease duration (yrs) | DIPSS | JAK2 status | CV risk | Complete Blood count (baseline) | Spleen Baseline(cm) | Ruxolitinib starting dose | Other meds combined with ruxo | Outcome | Patient status | ||
| Hb | WBC | Platelet | ||||||||||||
| 1 | 63/M | 10 | 12 | Int-2 | + | CAD at risk; HPN | 99 | 2.50 | 133 | 12 | 15 mg BID | Androgens+pred | CI-SR* | Drop-out /Expired |
| 2 | 67/F | 10 | 3 | High-risk | + | No CAD risk factor | 68 | 2.70 | 102 | 10 | 15 mg BID | EPO+pred+androgen | CI-SR&AR** | Alive |
| 3 | 51/F | 10 | 2 | Int-2 | + | No CAD risk factor | 97 | 5.40 | 275 | 14 | 20 mg BID | Androgen | CI-SR | Alive |
| 4 | 49/M | 10 | 2 | Int-2 | - | No CAD risk factor | 74 | 9.10 | 189 | 22 | 15 mg BID | Pred | CI-SR | Alive |
| 5 | 64/F | 10 | 15 | Int-2 | n/a | No CAD risk factor | 77 | 6.87 | 101 | 16 | 15 mg BID | none | CI-SR | Alive |
| 6 | 56/F | 20 | 2 | Int-2 | + | No CAD risk factor | 100 | 25.5 | 867 | 14 | 20 mg BID | Androgen | CI-SR | Alive |
| 7 | 58/F | 20 | 5 | Int-2 | + | No CAD risk factor | 107 | 15.10 | 367 | 26 | 20 mg BID | Androgen | CI-SR | Drop-out/ Expired |
| 8 | 42/F | 10 | 3 | Int-2 | n/a | No CAD risk factor | 64 | 5.2 | 110 | 12 | 15 mg BID | EPO | CI-SR | Alive |
| 9 | 53/F | 20 | 1 | Int-2 | + | No CAD risk factor | 103 | 26.5 | 124 | 10 | 15 mg BID | none | CI-SR | Alive |
| 10 | 51/F | 10 | 8 | Int-2 | + | No CAD risk factor | 89 | 14.69 | 129 | 29 | 15 mg BID | none | SD*** | Alive |
| 11 | 59/F | 10 | 7 | High-risk | n/a | No CAD risk factor | 101 | 20.6 | 278 | 18 | 20 mg BID | none | CI -SR | Alive |
Table 2: Individual characteristics of myelofibrosis patients under ruxolitinib treatment.
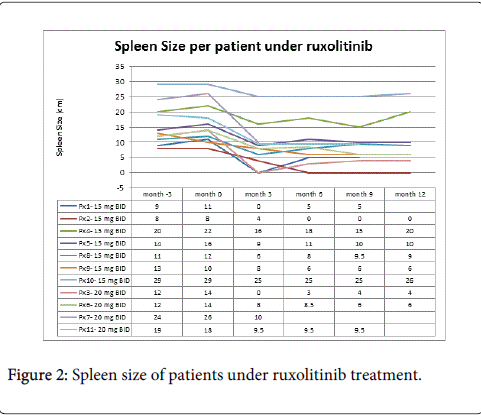
Figure 2: Spleen size of patients under ruxolitinib treatment.
Adverse events
The most common adverse events were hematologic toxicity which included grade 3 anemia in 10 out of 11 patients and grade 1-4 thrombocytopenia in 8 out of 11 patients especially during the 1st three months of therapy (Figures 3 and 4). There were no signs of overt bleeding from thrombocytopenia. None had neutropenia nor febrile neutropenia. Non-hematologic adverse events were gastrointestinal disorders seen in 5(45%), hepatobiliary disorders 4(36%) and cardiac dysfuction 1 (9%) (Table 3). Eight out of 11 patients had to hold ruxolitinib therapy temporarily due to cytopenia/s which recovered spontaneously and/or with transfusion of blood products, after which ruxolitinib was restarted with a lower dose. Ruxolitinib was combined with other adjunct medications for myelofibrosis like androgens, corticosteroids and erythropoiesis stimulating agents (ESA) to decrease the severity of anemia/thrombocytopenia and avert need for blood transfusion. Currently, there are nine (9) patients still receiving ruxolitinib, while there were 2 drop-outs due to death from causes unrelated to myelofibrosis or the current treatment as assessed by their attending physician. The two cases who died were due to 1) fatal arrhythmia, and 2) ruptured duodenal artery aneurysm.
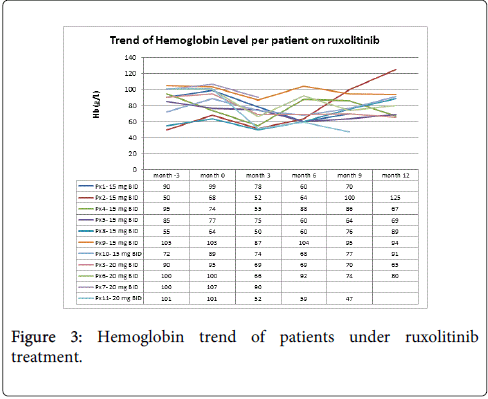
Figure 3: Hemoglobin trend of patients under ruxolitinib treatment.
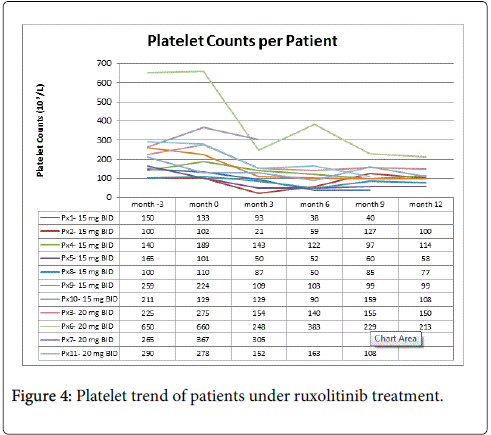
Figure 4: Platelet trend of patients under ruxolitinib treatment.
| No of Patients (%) | |||||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 | |
| Anemia | 0 | 1 (9%) | 10(91%) | 0 | 0 |
| Thrombocytopenia | 1 (9%) | 2(18%) | 4(36%) | 1(9%) | 0 |
| Neutropenia | 0 | 0 | 0 | 0 | 0 |
| Febrile Neutropenia | 0 | 0 | 0 | 0 | 0 |
| Gastrointestinal Nausea &vomiting Diarrhea Ruptured duodenal artery aneurysm Diverticulitis |
1(9%) 2(18%) 0 0 |
0 0 0 0 |
0 0 0 1(9%) |
0 0 0 0 |
0 0 1(9%) 0 |
| Muskuloskeletal | 0 | 0 | 0 | 0 | 0 |
| Pulmonary disorders Pneumonia |
0 | 1(9%) | 3(27%) | 0 | 0 |
| Cardiac disorders Conduction abnormalities |
0 | 0 | 0 | 0 | 1(9%) |
| Hepatobiliary disorders/elevated liver enzymes | 4(36%) | 0 | 0 | 0 | 0 |
| Others | |||||
Table 3: Adverse events during treatment with ruxolitinib.
Ruxolitinib VS BAT
The patients given ruxolitinib were matched by age with historical controls given best available therapy. All of the patients under best available therapy (BAT) were taking hydroxyurea for splenomegaly, which was combined with either steroids and/or androgen for anemia. There was a remarkable decrease in spleen size in ruxolitinib group compared to BAT group. The diminution in spleen size was evident within the first 3 months of treatment with ruxolitinib at a mean of 53.5% from baseline size compared to a mean of 18% decrease in the BAT group (Figure 5). A statistical significance cannot be computed because of the small sample size and the descriptive, retrospective nature of the study. Thrombocytopenia and anemia occurred more frequently in the patients receiving ruxolitinib than in those receiving the best available therapy. Majority of the patients who were given ruxolitinib required transfusion with packed red cells and/or platelet concentrate during the 1st three months of therapy with decreasing need after long term use but only 1 achieved transfusion independence (Figures 6 and 7).
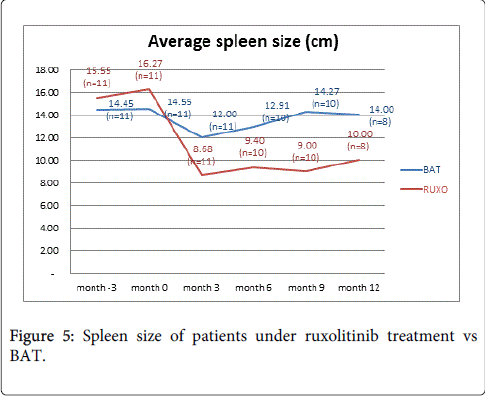
Figure 5: Spleen size of patients under ruxolitinib treatment vs BAT.
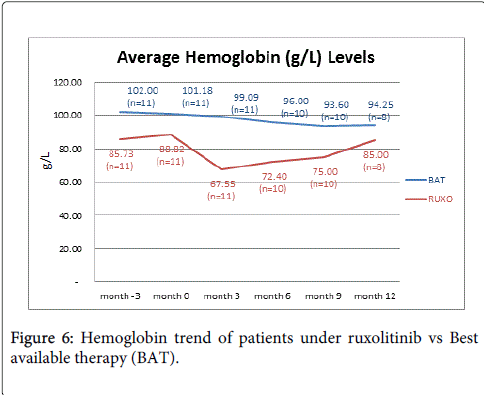
Figure 6: Hemoglobin trend of patients under ruxolitinib vs Best available therapy (BAT).
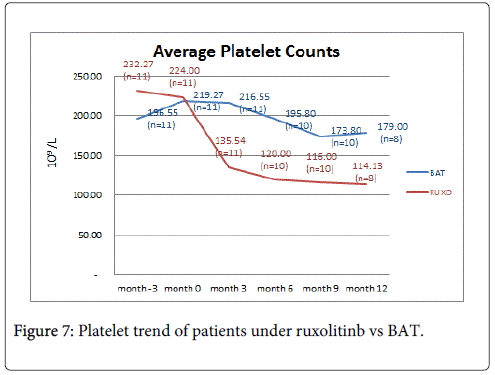
Figure 7: Platelet trend of patients under ruxolitinb vs BAT.
Myelofibrosis is one of several diseases in the spectrum of myeloproliferative neoplasms (MPN). Approximately 50 percent of cases have a mutation in the Janus kinase 2 (JAK 2) gene. The Janus kinase family of protein tyrosine kinases (JAKs) plays an important role in the signalling of a number of cytokines and hematopoietic growth factors, hence its mutation results in the pathogenesis of the different MPNs. Ruxolitinib (3-(4-(7HPyrrolo[2,3-d]pyrimidin-4-yl)-1H-pyrazol-1-yl)-3-cyclopentylpropanenitrile)) is an orally active and potent inhibitor of Janus kinases [6]. The local experience with ruxolitinib is consistent with the previous studies on its efficacy to reduce the spleen size remarkably. The best response during treatment was clinical improvement in both spleen and anemia in 1 out of 11 patients, wherein there was disappearance of splenomegaly and improvement of peripheral blood counts hence achieving transfusion independence. Nine out of 11 patients had clinical improvement specifically decrease in spleen size with a mean of 53.5% from baseline size. One had stable disease. As with the COMFORT-I trial by Verstovsek S. et al, ruxolitinib was compared with placebo in patients with myelofibrosis, the results showed a reduction in spleen size which was reached in 41.9% on the ruxolitinib group compared to 0.7% in the placebo group(p<0.001) [7,8]. The COMFORT-II trial by Harrison et al compared ruxolitinib with Best available therapy (BAT), the results showed that 28% of patients in the ruxolitinib group had at least 35% reduction in spleen volume at week 48 compared with 0% in the group receiving best available therapy (p<0.001) [9]. When we compared our patients on ruxolitinib compassionate use program vs historical controls on BAT, it also showed a better spleen size reduction from baseline at 53.5% vs 18% respectively.
Both COMFORT I and II trials showed anemia and thrombocytopenia as the most common adverse event. In COMFORT-I, 60% and 38% of ruxolitinib- and placebo-treated patients, respectively, received red blood cell transfusions during the treatment phase. In COMFORT-II, treatment-emergent anemia was 2-3-fold higher in the ruxolitinib arm relative to the best available therapy arm. This is consistent with the reported adverse events among our Filipino patients who received ruxolitinib. Grade 2-3 anemia was seen in all of our patients. There was also an increase in requirement for blood transfusion in 5 out of 11 patients especially during the 1st three month of treatment. These hematologic toxicities may be explained by the mechanism of action of the drug, since JAK-STAT pathway plays a central role in the signal transduction of erythropoietin and thrombopoietin, hence its inhibition may result to anemia and thrombocytopenia [10,11]. In COMFORT-I and COMFORT-II, the median time to onset of grade 3/4 thrombocytopenia was 8 weeks. The median time to platelet recovery >50 × 109/L after dose interruption was 14 days. Similarly, the median time to onset of grade 2 or higher anemia was 6 weeks. From our experience, hematologic toxicities were generally manageable, and were usually addressed by blood transfusion, dose reductions or temporary discontinuation and/or use of ESA’s and bone marrow stimulants. One common observation is that anemia and thrombocytopenia were more frequent and severe in Filipino patients given ruxolitinib using the standard dose of 20 mg BID based on clinical trials with Caucasian patients. Hematologic toxicities were noted to be reversible and dose dependent and so majority of our Filipino patients continued with a lower dose of ruxolitinib between 5 mg BID to 15 mg BID. Recognizing that there may be biologic variability in Asians then determination of optimal dose in this population merits investigation in future clinical trials. A limitation of the current study is the small sample size and non-probability sampling used; because of this it was difficult to find a statistically significant relationship from the data.
In both COMFORT I and COMFORT II trials, quality of life (QOL) were measured and included as endpoint using a QOL questionnaire (EORTC-Q30).This is another limitation of our study, since there was no single objective scale for symptom assessment that was used by the treating physicians, thus quality of life was not included in our analysis.
In summary compared to best available therapy, patients who received ruxolitinib had a remarkably reduction in splenic size particularly evident within the 1st three months of therapy. Thus, ruxolitinib is a viable treatment option for Intermediate-2 to high risk myelofibrosis patients with massive splenomegaly. However, anemia and thrombocytopenia were common adverse events during the treatment and may be managed with blood transfusion, dose reductions or temporary discontinuation and/or use of erythropoiesis stimulating agents (ESA) and/or androgens.
We would like to thank Dr Lhoree Gie Antonio-Dela Cruz, Dr Teresita Dumagay and Dr Rosalyn Valerie Cortes for their assistance in data collection. Research grant: Novartis Healthcare Philippines
The authors declare no conflict of interests.