Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2013) Volume 2, Issue 2
clinical outcome in patients with rapidly growing thyroid. Design: Case series, three patients presenting with a growing enlarged thyroid at a secondary practice for endocrinology. Methods / Outcome measures: Diagnostic findings, clinical course and comparison to the literature. Results: All patients were postmenopausal women (age: 58-74 years). The leading symptom was goiter with growing volume or mass in the neck region. Upon ultrasound, all patients demonstrated hypoechoic irregular areas suggesting autoimmune thyroiditis. In one patient, the thyroid capsule could not be distinguished suggesting infiltrative disease, while another patient had markedly enlarged cervical lymph nodules. Thyroid function was hypothyroid in two patients and euthyroid in one. The latter patient had elevated anti-thyroid antibody titres, fine needle aspiration cytology indicated lymphoma and diagnosis was confirmed by excisional biopsy. This patient was successfully treated with chemotherapy remaining disease free four years later. In the two other patients, repeated cytology and lymph nodule resection could not provide definite diagnosis and both underwent thyroidectomy. Final histology revealed large B-cell lymphoma localized within the thyroid in one patient, who is disease free two years after surgery and diagnosis of chronic autoimmune thyroiditis with severe lymphadenitis in the other. Conclusions: Thyroid lymphoma should be considered in patients with increasing thyroid volume and signs of autoimmune thyroiditis. Finite differential diagnosis between autoimmune thyroiditis and lymphoma cannot always be achieved cytologically. Sufficient material is necessary and some patients may need thyroidectomy to classify disease definitively.
<Keywords: Autoimmune thyroiditis; Fine needle aspiration Cytology; Goiter; Lymphoma; Thyroid cancer; Thyroid nodule
Patients presenting with whole thyroid enlargement or growing nodules require a differential diagnosis between malignant thyroid disease, autoimmune thyroiditis and thyroid lymphoma. This is essential as the therapeutic consequences are quite different for each condition [1]. Standard procedures for diagnosing increasing thyroid volume or growing nodules include sonography, scintigraphy to differentiate between functioning and nonfunctioning tissue, laboratory tests (thyroid function, autoantibodies, thyroglobulin, calcitonin) and Fine Needle Aspiration Cytology (FNAC) [2-4]. Differentiation between autoimmune thyroiditis and thyroid lymphoma can be especially challenging due to variable overlap of both conditions [5-7]. We report the clinical course and diagnostic findings of three patients presenting with a rapidly growing and enlarged thyroid suspicious for lymphoma or malignant thyroid disease and compare the findings with the literature.
Patients were admitted because of increasing thyroid volume. Diagnostic procedures compromised ultrasonography of the thyroid gland and neck region using a ultrasound scanner with a wide band linear probe (5 - 10 MHz) documenting total thyroid volume, thyroid tissue echogenicity, nodules and lymphadenopathy. Thyroid scintigraphies and FNAC were obtained according to standardized conditions. Laboratory tests on thyroid function or thyroid disease classification (FT3, FT4, TSH, calcitonin, thyroglobulin, antithyroid antibodies (antithyroperoxidase, anti-Tg) were performed during routine conditions using commercial standard tests.
All diagnostic procedures were part of the patients evaluation performed during clinical practice conditions; all patients gave their consent to the respective investigations.
Patient 1
A 63 year old woman was admitted due to increasing goiter predominantly of the left side first observed three months prior. At the initial admission (10/2008) she had no local problems and no signs of general sickness. The thyroid volume was 30 ml (11 ml right, 19 ml left side) determined sonographically, with a hypoechoic irregular structure, and a nodule on the left side (10 ml volume) shown to be cold following scintigraphy. There were no enlarged cervical lymph nodules. FNAC of the left nodule showed plenty of lymphocytes, few regressive thyreocytes and no signs of malignancy. The findings suggested autoimmune thyroiditis, however TPO antibodies were not or only marginally increased (43 kU/ml; normal value <34 kU/ ml). Thyroid function was latently hypothyroid (TSH 12.0 U/l). Levothyroxine therapy was initiated and, eight months later, although the patient was euthyroid (TSH 0.9), the left thyroid lobe increased and nearly doubled in size (left side 38 ml). A second left side FNAC yielded a finding similar to the first suggesting autoimmune thyroiditis. The patient was symptom free and elected for conservative management with continued levothyroxine therapy. During follow up (3/2010), the right thyroid side had enlarged (16 ml right side, 30 ml left side) and appeared sonographically hypoechoic and in homogenous. The patient was still free of symptoms and declined surgical therapy. FNAC of the right side revealed some oxyphilic cells and was classified most likely to be autoimmune thyroiditis - laboratory tests for autoantibodies remained negative; thyroglobulin was not or only marginally increased. Five months later (8/2010), a further increase was observed with a doubling of the right thyroid (38 ml) and a slight decrease of the left side (25 ml). Repeated FNAC was rich in cells with some signs of proliferative activity, indifferent thyroiditis but no malignancy. Within a F-18-FDG-PET/CT, performed for staging of rectal carcinoma for which the patient was operated in 4/2010, the right thyroid showed an increased uptake of F-18-FDG. The patient finally agreed to surgical therapy to clarify the thyroid enlargement.
Total thyroidectomy was performed (10/2010) and histology revealed a magnocellular B-cell lymphoma of the right and chronic lymphocytic thyroiditis of the left thyroid (Figure 1). Staging showed no signs of lymphoma outside the thyroid. Chemotherapy and therapy with rituximab was recommended, but refused by the patient. During follow up nine months later, the patient observed a palpable mass within the left supraclavicular fossa. No further lymph nodules were found by staging with computer tomography of thorax and abdomen. The mass was removed for definitive histology that only showed sclerotic tissue but no vital tumor. As such, the patient did not receive chemotherapy but was monitored. She is in good health two years (10/2012) after thyroidectomy without signs of recurrent B-cell lymphoma.
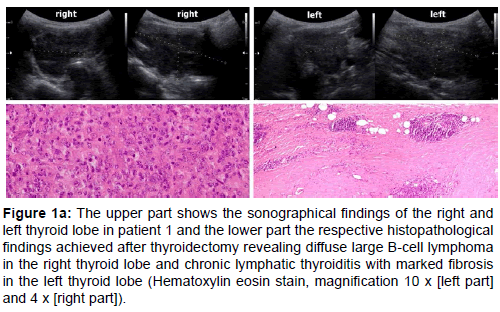
Figure 1a: The upper part shows the sonographical findings of the right and left thyroid lobe in patient 1 and the lower part the respective histopathological findings achieved after thyroidectomy revealing diffuse large B-cell lymphoma in the right thyroid lobe and chronic lymphatic thyroiditis with marked fibrosis in the left thyroid lobe (Hematoxylin eosin stain, magnification 10 x [left part] and 4 x [right part]).
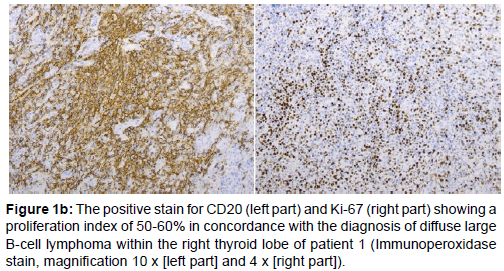
Figure 1b: The positive stain for CD20 (left part) and Ki-67 (right part) showing a proliferation index of 50-60% in concordance with the diagnosis of diffuse large B-cell lymphoma within the right thyroid lobe of patient 1 (Immunoperoxidase stain, magnification 10 x [left part] and 4 x [right part]).
Patient 2
A 74-year-old woman was admitted in 7/2007 because of a markedly increased left thyroid over the four weeks prior. She complained about hoarseness and pain within the neck. There was no previous thyroid disease. The patient history revealed treatment of colon carcinoma twenty years ago, of breast cancer three years ago, and monoclonal gammopathy of unknown significance diagnosed eight years before. Furthermore, she suffered from hypertension, coronary heart disease and arrhythmia absoluta for several years.
Upon admission, the left thyroid was palpably enlarged with increased consistency and fixed tissue during swallowing. Thyroid volume was determined sonographically (right thyroid: 13 ml, left thyroid: 45 ml) with inhomogeneous echonormal or hypoechoic structure. There was one hypoechoic nodule in the left thyroid 29 ml in volume. The patient was euthyroid (TSH 3.2) and had markedly increased anti-TPO antibodies (>1300 U/l). During the following four weeks, the left thyroid doubled in size to 90 ml and the thyroid border was not clearly distinguishable from the surrounding soft tissue. Computer tomography showed the enlarged thyroid, but no enlarged lymph nodules. FNAC of the left thyroid showed no signs for anaplastic thyroid carcinoma but was suggestive of lymphoma; however immunocytological examination with a CD20 antibody showed only a few positive cells. An excisional biopsy of the left thyroid revealed a diffuse infiltration of muscle and soft tissue with a pleomorphic, partly necrotic, malignant tumor. Immunohistology was positive for CD20, proliferation activity was >50%, confirming the diagnosis of a magnocellular, diffuse B-Cell lymphoma. Further staging showed only few mediastinal lymph nodules up to 15 mm. LDH was slightly elevated (269 U/l, normal value <248 U/l) and sCD25 was increased (1611 U/ ml, normal value <900 U/ml). The patient received three chemotherapy cycles with COP (cyclophosphamid / vincristine, prednisolon) and rituximab from 10/2007 to 12/2007. Therapy response was positive and restaging showed no enlarged lymph nodules. During follow up in 12/2010, thyroid size was normal (5 ml right side, 3 ml left side) with a small nodule in the left side (0.9 ml). The patient was complaint free, however became hypothyroid after chemotherapy, requiring levothyroxine substitution. Follow up in 11/2011 showed no evidence of recurrent lymphoma.
Patient 3
A 58-year-old woman was admitted in 6/2011 because of an increased thyroid volume three months prior and pressure within the neck region. She had received levothyroxine 75 μγ for the last six years due to hypothyroidism. Laboratory tests showed euthyroid function under levothyroxine substitution (TSH 3.9 IU/l), negative anti-TPO (<5 kU/l), increased Tg-antibodies (529 kU/l), normal Tg 6.1 (recovery 85%) and normal CRP (<1.0 mg/l). Sonographically, the thyroid was enlarged, especially the left side, (11 ml right, 28 ml left side) and tissue appeared hypoechoic, inhomogenous without distinct nodules. There were multiple markedly enlarged lymph nodules within the left neck compartment, > 20 mm in size (Figure 2). Following discontinuation of levothyroxine substitution, the entire thyroid showed nearly no uptake during thyroid scintigraphy. FNAC demonstrated enriched lymphoid-like cells suggestive of a Non Hodgkin lymphoma. In 7/2011, one cervical lymph nodule was removed and histology was negative for lymphoma. Staging by computer tomography of the thorax and abdomen and a bone marrow biopsy also showed no evidence for malignant lymphoma. Therefore conservative management and follow up under continuing levothyroxine substitution was recommended.

Figure 2: The sonographical appearance of the left thyroid lobe (left part) and the cervical lymphadenopathy (right part) found in patient 3, which was diagnosed after surgical therapy and histopathological studies as chronic lymphocytic thyroiditis and severe nonspecific hyperplastic lymphadenitis.
Two months later (8/2011), the patient had increasing symptoms of pain and pressure in the neck, dyspnoea, and difficulty in swallowing. CRP was not increased. The sonographical findings were unchanged. A repeated FNAC of the thyroid and of a lymph nodule suggested thyroiditis. Analysis of the FNAC for mutations within BRAF V600 E, K601E, NRAS 61, HRAS 61, KRAS 12 and 13 did not reveal any abnormalities. The patient still suffered from cervical pressure and decided against careful monitoring in favor of surgery therapy to obtain a finite histology. In 10/2011, she underwent thyroidectomy and lymphadenectomy of the central and left lateral compartment. Histologically, the thyroid showed typical changes associated with lymphocytic thyroiditis, but no signs of malignancy or lymphoma and the enlarged lymph nodules showed an excessive lymphatic hyperplasia but also no lymphoma. The patient was substituted with levothyroxine and is symptom free one year after surgery.
(Table 1) summarizes the diagnostic findings and clinical outcome of the three patients.
| Patient Sex / age | Clinical symptoms | Thyroid volume ( ml) diagnosis / follow up | Thyroid function at diagnosis | Thyroid antiboidy antiTPO / TAK | Enlarged cervical lymph nodules | FNAC / histology* | Therapy | Final histology / diagnosis | Disease free follow up after therapy |
| F / 63 | no | 30 / 63 (after 2 years) | hypothyroid | negative / negative | no | autoimmune thyroiditis -no malignancy (performed four times during follow up) | 1) clinical follow up, thyroxine - for 2 years 2) thyroidectomy (increasing right thyroid) | - B-cell lymphoma (right side); - chronic lymphatic thyroiditis (left side) | 2 years |
| F / 74 | local | 58 / 113 (after 4 weeks) | euthyroid | positive / not done | no | lymphoma / lymphoma | chemotherapy | B-cell lymphoma | 4.3 years |
| F / 58 | local | 39 / 44 (after 3 months) | hypothyroid | negative / positive | yes - left side | lymphoma / no malignancy, no lymphoma, thyroiditis | thyroidectomy + lymphadenectomy | autoimmune thyroiditis + lymphadenitis | 1 year |
FNAC: Fine Needle Aspiration Cytology
*Lymphadenectomy or Excisional biopsy from the thyroid
Table 1: Diagnostic findings, diagnosis and outcome in three patients with a growing enlarged thyroid.
Despite the same leading symptom of increasing thyroid volume in three patients, the final diagnoses confirmed by histology were thyroid lymphoma in two patients and autoimmune thyroiditis accompanied by lymphadenopathy in the third.
Although both characterized with lymphoma, the two patients demonstrated a distinct clinical course. The differential diagnosis for patient 2 was anaplastic thyroid carcinoma with a very rapid enlargement of the left thyroid causing local symptoms of hoarseness, tenderness and dyspnoea within few weeks. In contrast, patient 1 exhibited a more slowly but continuously increasing thyroid volume without clinical symptoms. In both patients, development of thyroid lymphoma was associated with autoimmune thyroiditis; however clinical presentation was also quite different. Autoimmune thyroiditis was diagnosed in patient 1 based on sonographical findings and repeated FNAC, while autoantibodies were negative or only marginally elevated and thyroid function was latently hypothyroidic at first admission. During follow up, the increasing thyroid volume despite sufficient levothyroxine substitution was suggestive of malignant disease. Repeated FNAC was insufficient to clarify the diagnosis and thyroidecotmy was ultimately required, which revealed the thyroid lymphoma. The diagnosis of autoimmune thyroiditis in patient 2 was guided by markedly elevated autoantibodies, euthyroid function at first admission, and clinically, the rapidly growing left thyroid mass with local symptoms was the leading symptom suggestive for malignant disease. Neither patient with thyroid lymphoma had enlarged lymph nodules within the neck region, no systemic involvement and disease was limited to the thyroid in patient 1 but showed extracapsular spread within the neck region in patient 2.
Both patients with lymphoma had signs of autoimmune thyroiditis, confirming the known increased risk for primary thyroid lymphoma in patients with chronic autoimmune thyroiditis [8-12]. There is an overlap between both conditions, clearly demonstrated in patient 1 where a histopathological diagnosis of autoimmune thyroiditis within the left thyroid lobe was concomitant with a B-cell lymphoma within the right lobe that developed during the two year observation time. Furthermore, the histological differentiation between diffuse lymphocytic infiltration associated with Hashimoto thyroiditis and lymphoma can be very difficult and may require additional techniques like immunohistochemical examination and molecular analysis [13]. Positive uptake during an F-18-FDG-PET-CT was found in one of our patients with lymphoma even though this is not a diagnostic criterion to differentiate between autoimmune thyroiditis and lymphoma as both conditions demonstrate an increased F-18-FDG-uptake [14]. This finding, however, was the key to convincing patient 1 to undergo surgical therapy, which revealed the magnocellular B-cell lymphoma.
The diagnostic dilemma between autoimmune thyroiditis and lymphoma is also demonstrated in patient 3 who showed clinical signs of pain, pressure within the neck, and marked cervical lymphadenopathy close to the enlarged left thyroid lobe. Although highly suggestive of malignant disease, none was found even by careful staging including lymphadenectomy. A thyroidectomy and lymphadenectomy was performed in response to persisting clinical symptoms and wish of the patient, which led to the finite diagnosis of autoimmune thyroiditis accompanied by lymphadenitis but no malignancy. Differential diagnosis of painful autoimmune thyroiditis, other forms of thyroiditis and lymphoma is a challenge and may require surgical therapy. Kon et al., describe the outcome of seven patients with painful Hashimoto thyroiditis who finally underwent surgical therapy: four patients had permanent and total relief, one patient had partial relief and two patients had transient relief but relapsed symptoms after variable time [6].
Among thyroid diseases, lymphoma is a rare condition representing about 2% of all malignant thyroid diseases [8,15]. The incidence is described to be 2.1 / million persons, predominantly postmenopausal women [10]. Histopathological studies revealed signs of autoimmune disease in about 50% of patients. As lymphoid tissue is normally absent in the thyroid, the acquired lymphoid tissue in connection with autoimmune thyroiditis is probably one step within the pathogenesis of thyroid lymphoma. The differentiation between autoimmune disease and extranodal marginal zone B-cell lymphoma (MALT) is a challenge and there is speculation that MALT can transform into aggressive lymphoma [16,17], which might have occurred in one of our patients (patient 1).
Diffuse large B-cell lymphoma is most common (60-80%), and the form found in our two lymphoma patients, while MALT is found in about 30%, and other subtypes like Hodgkin lymphoma or T-cell lymphoma are extremely rare findings [8,10,13,17,18].
Clinical signs of thyroid lymphoma are a rapidly enlarging goiter often accompanied by hypothyroidism, local symptoms like hoarseness and vocal cord paresis, and enlarged cervical lymph nodules in about 50% of patients. Only about 10% of patients present with B-symptoms, which were not seen in our patients [19].
The outcome of patients with thyroid lymphoma has been described in cytopathological studies ranging over a long period of observation (1960-1998) [20]. In a 27 patient cohort, DiBiase et al. found that combined modality therapy (n=8) is superior to radiotherapy alone (n=19) [20]. The overall survival rate of 5 years was 56% within this patient group. Within a retrospective study of 26 patients with thyroid lymphoma the 5 year (10 year) overall survival was 77% (54%) depending from the subtype and stage of disease [17]. Thieblemont et al. could not identify any clinical parameters to aid the prediction of lymphoma development from autoimmune thyroiditis.
In two more recent studies on the outcome of patients with thyroid lymphoma, including 171 patients observed between 1990 and 2004 and 87 patients observed between 1986 and 2006 it was shown that combined modality therapy is superior to single modality therapy in respect to overall survival ranging between 74 and 85% for 5 year survival rate [12,21]. In summary, these recent studies [12,21] underline the increased risk of thyroid lymphoma in postmenopausal women with autoimmune disease who present with a rapidly growing thyroid volume. Both of our patients with lymphoma had respective findings. Patients with thyroid lymphoma have a good prognosis if treated with combined modality therapy including radiotherapy, chemotherapy and rituximab. Surgical therapy is mostly unnecessary and can be limited to patients with unclear diagnosis in whom thyroidectomy or biopsy is essential for final disease classification. In patients with thyroidlimited lymphoma, surgical therapy alone may suffice but careful follow up is essential with respect to lymphoma recurrence (patient 1). Surgical therapy should not be the first choice for patients with diffuse large B-cell lymphoma, who often present with disseminated disease, as these patients generally respond quickly to chemotherapy and immunotherapy (as shown in our patient 2).
Patients with a history of hypothyroidism and markedly increase of thyroid volume, despite sufficient substitution therapy and typical findings of autoimmune thyroiditis, are at increased risk of developing thyroid lymphoma. FNAC often seems insufficient and excisional biopsy is required to obtain sufficient material for histology, whereby some patients may even need surgical therapy with thyroidectomy for final disease diagnosis.
All authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.