Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2015) Volume 5, Issue 3
Background: Previous studies showed that the dilated main pancreatic duct (MPD) and pancreatic cysts were the important predictors of the subsequent development of pancreatic cancer. The purpose of this study was to reveal the utility of non-contrast reduced radiation dose CT with iterative reconstruction for screening in high risk pancreatic cancer individuals by assessing the dilated MPD and cysts by using abdominal phantoms.
Materials and methods: Two phantoms with normal and abnormal pancreas with dilated MPD (5 mm) and cysts (5 mm, 10 mm and 15 mm) were constructed. Each phantom was scanned by ten images using following three protocols: 120 kVp and 120mA with filtered back projection (FBP) algorithm (120 kVp-FBP), 80 kVp and 168mA with FBP algorithm (80 kVp-FBP), and 80 kVp and 168mA with sinogram affirmed iterative reconstruction (SAFIRE) (80 kVp-SAFIRE). The image noise and contrast-to-noise ratio (CNR) of the 15mm cyst were assessed. The radiation dose was assessed with the volume CT dose index (CTDIvol). Two radiologists scored the image quality and conspicuity of the dilated MPD and cysts.
Results: Mean image noise significantly decreased from 80 kVp-FBP images to 80 kVp-SAFIRE and 120 kVp-FBP images (p < 0.001). The CNR significantly increased from 80 kVp-FBP images to 120 kVp-FBP and 80 kVp-SAFIRE images (p < 0.05). Image quality was significantly lower in the 80 kVp-FBP images than in 120 kVp-FBP and 80 kVp- SAFIRE images in both readers (p < 0.05). The conspicuity point for the dilated MPD and three cysts was higher in 80 kVp-SAFIRE images than in 80 kVp-FBP and 120 kVp-FBP images. CTDIvol was reduced by 60 % at 80 kVp protocol.
Conclusion: Non-contrast 80 kVp-SAFIRE CT protocol allowed for higher conspicuity of dilated MPD and cysts at a reduced radiation dose compared with 120 kVp-FBP protocols.
<Keywords: High-risk individuals with pancreatic cancer; Screening; Reduced radiation dose CT with iterative reconstruction; Anthropomorphic abdominal phantom
The prognosis of all patients with pancreatic cancer remains quite poor, with a 5-year survival rate of only 5% [1]. According to the Japan Pancreatic Cancer Registry reported by Egawa et al. [2], the 5-year survival rate after surgery based on TNM classification is 85.8% in stage 0, 68.7% in stage IA and 59.7% in stage IB disease. Therefore, in improving the therapeutic outcomes for these patients it is vital that their cancer is detected at stage 0 or I.
There are two groups of hereditary [3,4] and non-hereditary conditions (e.g., diabetes mellitus, chronic pancreatitis, and certain abdominal surgeries) [5-7] that are known to be at elevated risk of pancreatic cancer; screening examinations of these groups have been proposed by several investigators [8-10]. Contrast-enhanced dynamic computed tomography (CT) is the most commonly used modality for clinical evaluation of pancreatic cancer. Yoon et al. [11] have reported that small pancreatic cancer (≤2 cm) could not be detected in 73% of patients on multiphasic multidetector CT images; however, most of these small pancreatic cancers exhibited secondary signs including main pancreatic duct (MPD) dilatation. In addition, previous studies using CT or ultrasonography have shown that MPD dilatation and the presence of pancreatic cysts were strong independent predictors of subsequent development of pancreatic cancer [12-14]. Contrastenhanced dynamic CT has a number of disadvantages such as patient exposure to ionizing radiation and the high cost of the enhanced images [15,16]. If these predictive signs could be detected using reduced radiation dose non-contrast-enhanced CT, these shortcomings could be addressed. Lowering tube voltage settings as a means of reducing radiation exposure typically results in increased image noise using the traditional filtered back projection (FBP) image reconstruction technique [17,18]. Iterative reconstruction (IR) is an alternative reconstruction technique that produces a reduced image noise at lower radiation doses relative to those of FBP. Sinogram-affirmed IR (SAFIRE) is one of the most recently developed raw data-based IR algorithms [19-21], and the benefits of SAFIRE for abdominal CT have been reported in previous studies [21-31]. Here, we constructed two anthropomorphic abdominal phantoms including a normal pancreas and an abnormal pancreas with a dilated MPD and cysts.
The objective was to elucidate the diagnostic utility of reduced radiation dose non-contrast-enhanced CT with SAFIRE for screening examination of high risk pancreatic cancer patients by assessing of the dilated MPD and cysts using abdominal phantoms.
This study is part of on-going research involving assessment of the radiation dose associated with abdominal imaging; it is financially supported by Siemens Japan (Tokyo, Japan). One author (“T.I.”) is an employee of Siemens Japan. None of the authors who are not employees of Siemens Japan have any financial interests with that company, and all authors maintained control over all of the data presented.
Mean CT values for the upper abdominal organs (pancreas, liver, gallbladder, kidneys, abdominal aorta, stomach, duodenum, intraabdominal fat, muscle, subcutaneous fat, diaphragmatic crus, vertebrae and ribs) were measured on non-contrast-enhanced CT images for the 60 subjects who met the following conditions: 20 subjects (10 males and 10 females) in three age groups, namely 50–59, 60–69 and 70–79 years; the subjects had not undergone surgery involving the thoracic, abdominal and pelvic organs, and did not exhibit abnormal findings regarding abdominopelvic CT images, or abnormal values in biochemical examination of the blood; and they had a normal body mass index (BMI; 18.5−25).
The scanning parameters for these subjects were: 120 kVp; 1.0- mm detector collimation; and 1.0-pitch at four discrete exposure settings (120 mAs [100% exposure level; volume CT dose index, 9.1 mGy]). Automated exposure control was turned off. Images were reconstructed at 1-mm section thickness using the standard FBP algorithm. An anthropomorphic normal pancreatic phantom (volume, 32 × 20 × 15 cm; mass, 10.5 kg) (Figure 1) was constructed by Kyoto Kagaku (Kyoto, Japan) based on a normal subject (62 year old male with a BMI of 22) and mean CT values were calculated for each organ (Table 1). Regarding the abnormal phantom with the dilated MPD and cysts, mean CT values for 20 dilated MPDs and 20 dilated branch ducts in 35 patients with surgically diagnosed intraductal papillary mucinous neoplasm of the pancreas were measured on non-contrast-enhanced CT images. The abnormal phantom with a dilated MPD of 5-mm in diameter and 5-mm cyst in the pancreatic tail, a 10-mm cyst in the body, and a 15-mm cyst in the head was constructed based on these mean CT values (Table 1; Figure 2).
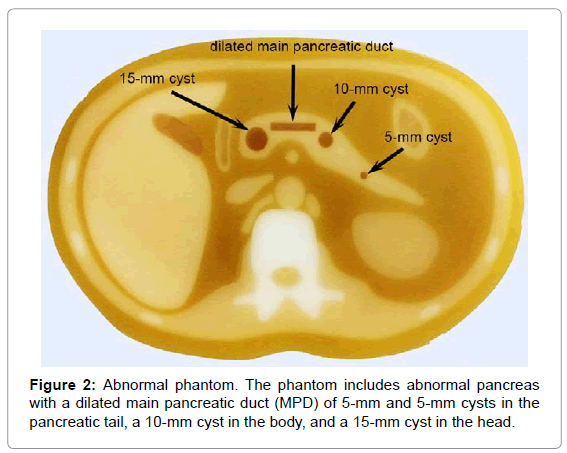
Figure 1: Normal abdominal phantom. Photographs show normal abdominal phantom in front view (a) and left oblique view (b).The phantom is composed of material that mimics the upper abdomen including the normal pancreas.
| Pancreas | Liver | Gallbladder | Kidney | Aorta | Gastric wall | Fluid in the stomach | Intraabdominal fat | ||
|---|---|---|---|---|---|---|---|---|---|
| Subjects(HU) | 45 | 60 | 12 | 31 | 46 | 40 | 15 | -70 | |
| Phantom(HU) | 47 | 63 | 29 | 39 | 50 | 39 | 24 | -56 | |
| Muscle | Subcutaneous fat | Diaphragmatic crus | Vertebra | Rib | Main pancreatic duct | cyst | |||
| Subjects(HU) | 45 | -70 | 45 | 378 | 318 | 5 | 5 | ||
| Phantom(HU) | 47 | -58 | 44 | 396 | 270 | 22 | 15 | ||
Table 1: Mean CT values of the upper abdominal organs.
Figure 2: Abnormal phantom. The phantom includes abnormal pancreas with a dilated main pancreatic duct (MPD) of 5-mm and 5-mm cysts in the pancreatic tail, a 10-mm cyst in the body, and a 15-mm cyst in the head.
The normal pancreatic phantom and abnormal phantom with the dilated MPD and cysts were scanned using the single-source acquisition mode of a dual-source 128-detector row CT scanner (Definition Flash: Siemens Healthcare, Forchheim, Germany). Image acquisition and reconstruction parameters were as follows: 120 kVp and 120 mA using the FBP algorithm (120 kVp-FBP), which is the tube voltage in clinical use for pancreatic multidetector CT(MDCT) in our department; 80 kVp and 168 mA using the FBP algorithm (80 kVp-FBP), and 80 kVp and 168 mA using SAFIRE (80 kVp-SAFIRE); 1.0-mm section thickness; 0.6-mm detector collimation; 0.9 pitch; 33-cm field of view; and 1.0-s gantry rotation time. Auto exposure control (CARE Dose4D: Siemens Healthcare) was turned off. The 120 kVp-FBP images and 80 kVp-FBP images were reconstructed at 1-mm section thickness using the standard B35f kernel with FBP. The 80 kVp-SAFIRE images were reconstructed at 1-mm section thickness using the matching I30f kernel of SAFIRE. In SAFIRE, two iteration loops are used to reconstruct the image. SAFIRE starts reconstruction using a weighted FBP image and introduces it into the first loop in the raw data domain to remove artifacts, resolve imperfections and improve spatial resolution by repeating re-projection and projection several times; then, the image is transferred to the second loop in the image domain to reduce noise until the desired noise level is achieved [19]. SAFIRE can yield lower image noise and a higher signal-to-noise ratio and contrast-to-noise ratio (CNR) than the FBP algorithm. In SAFIRE, noise reduction can be adjusted with five presets (strength 1–5); 1 being the weakest and 5 the strongest [19,21,22]. As recommended in previous studies [22,29], a medium strength of 3 was applied in this study. Ten scans were performed in each normal and abnormal pancreas using each protocol (120 kVp-FBP and 80 kVp-FBP).
For radiation dose assessment, the volume CT dose index (CTDIvol) was recorded for the scans at 120 kVp and 80 kVp protocols. The CTDIvol was obtained from the dose page provided by the CT scanner. Dose reduction in percentages was calculated relative to the radiation doses for the 120 kVp and 80 kVp protocols.
The obtained images were assessed using window level 40 and window width 350. Analysis was performed using a high-definition liquid crystal display monitor.
Image noise
For each of the three protocols image noise was measured by a radiologist with approximately 29 years’ experience in abdominal CT imaging, as the standard deviation (SD) of the pixel values from a circular or ovoid region of interest (ROI; mean pixel number, 486; range, 450–515 pixels) drawn on the liver of the normal phantom, and the mean SD obtained from the 10 slice images was analyzed.
CNR
For each of the three protocols, the CNRs relative to the pancreas for the 15-mm cyst were calculated by a radiologist with approximately 29 years’ experience in abdominal CT imaging using the following equation: CNR = (ROI p − ROI c)/SD n, where ROI p is the mean attenuation for the pancreas, ROI c is the mean attenuation obtained in the 10 slice images for the 15-mm cyst and SD n is the mean image noise.
Subjective image quality
Subjective image quality for the normal phantom was independently assessed on three protocol images from the normal phantom by two radiologists with approximately 38 and 14 years’ experience in abdominal CT imaging. They were blinded to the scanning protocols. The image quality was assessed based on the contour sharpness scores of the superior mesenteric artery (SMA) on three-point scales as follows: 1, poor (poorly defined SMA contour); 2, good (somewhat defined SMA contour); 3, excellent (very sharp SMA contour). The data set consisted of 30 images each containing 10 images obtained using each of the three protocols (120 kVp-FBP, 80 kVp-FBP and 80 kVp-SAFIRE) from a normal phantom. The data sets were presented in a different random order for each reader. The mean conspicuity point obtained in the 10 slice images scanned in each protocol was analyzed for each reader.
Conspicuity of the dilated MPD and cysts
The CT images from the two phantoms obtained using the three protocols were independently assessed by two radiologists with approximately 12 and 26 years’ experience in abdominal CT imaging. The readers were blinded to the number, location and size of the lesions, as well as to the scanning protocols. Before starting the assessment, each reader was given the criteria for image grading. The readers were asked to mark the location of the tumors on evaluation sheets, along with the grade of conspicuity of the dilated MPD and cysts on the following 5-point scale: 1, no demonstrable lesion; 2, questionable lesion; 3, subtle with poorly defined margins; 4, clearly seen with poorly visualized margins; and 5, clearly seen with sharp margins. A dataset consisted of 60 images each containing 20 images (10 images of the normal pancreas and 10 images of the abnormal pancreas) using each of the three protocols (120 kVp-FBP, 80 kVp-FBP and 80 kVp- SAFIRE). The datasets were presented in a random order that differed for each reader.
For evaluation of differences in image noise, mean CNR, image quality and lesion conspicuity among the three protocols, an exact Wilcoxon’s matched-pairs signed-rank test was performed. Interobserver agreement between the two readers regarding the evaluation of the image quality and the conspicuity of the dilated MPD and cysts was evaluated using weighted κ statistics. In accordance with the findings of Landis and Koch [32], k values of 0–0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80 and 0.81–1.00 were considered to represent slight, fair, moderate, substantial and almost perfect agreement, respectively. Statistical analyses were performed using SPSS software for Windows (Version 15.0: SPSS, Chicago, IL, USA). A p value of < 0.05 was considered as indicating a significant difference.
Radiation dose assessment
The CTDI vol was 60% lower using the 80 kVp protocol (3.7 mGy) compared with the 120 kVp protocol (9.2 mGy).
Image noise
The mean image noise was significantly higher in the 80 kVp- FBP images (mean SD, 31.8 HU) than in the 80 kVp-SAFIRE images (mean SD, 22.3 HU) and 120 kVp-FBP images (19.6 HU) (80 kVp-FBP images vs. 120 kVp-FBP images, p < 0.001; 80 kVp-FBP images vs. 80 kVp-SAFIRE images, p < 0.001; and 120 kVp-FBP images vs. 80 kVp- SAFIRE images, p = 0.0001).
CNR
The CNR was significantly higher in the 120 kVp-FBP images (1.91) and 80 kVp-SAFIRE images (2.21) relative to the 80 kVp-FBP images (1.52) (80 kVp-FBP images vs. 120 kVp-FBP images, p < 0,001; 80 kVp-FBP images vs. 80 kVp-SAFIRE images, p < 0,001; and 120 kVp-FBP images vs. 80 kVp-SAFIRE images, p = 0.01).
Subjective image quality
The mean score for subjective image quality in the 80 kVp-FBP images (1.6 for reader 1 and 1.7 for reader 2) was significantly lower than those for the 120 kVp-FBP images (2.9 for both readers) and 80 kVp-SAFIRE images (2.7 for reader 1 and 2.8 for reader 2) for both readers (p < 0.05; Figure 3). There was no significant difference between the mean scores for subjective image quality in the 120 kVp-FBP images and 80 kVp-SAFIRE images. The interobserver agreement between the two readers for the mean score for subjective image quality using the three protocols ranged from substantial to almost perfect agreement (120 kVp-FBP images, κ = 1.00; 80 kVp-FBP images, κ = 0.80; 80 kVp- FBP images, κ = 0.74).
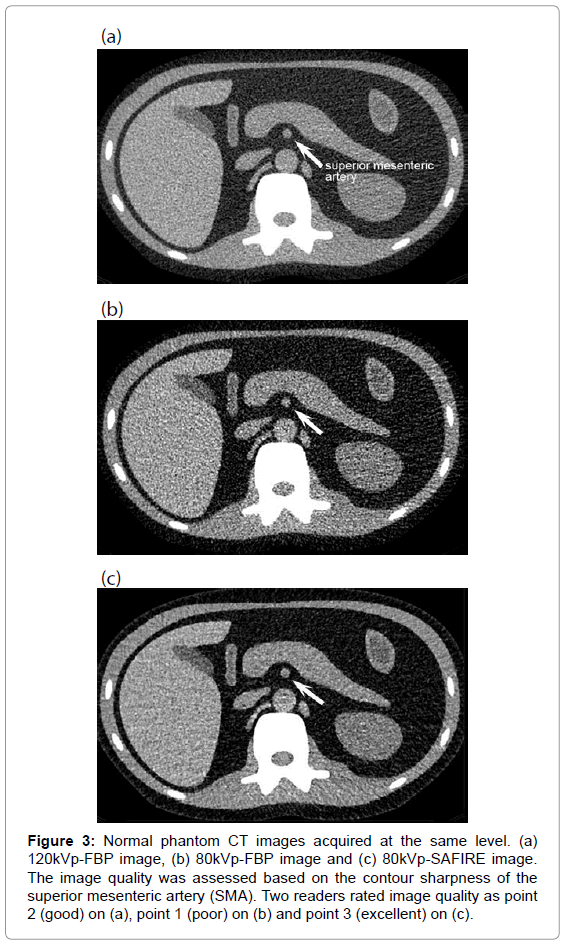
Figure 3: Normal phantom CT images acquired at the same level. (a) 120kVp-FBP image, (b) 80kVp-FBP image and (c) 80kVp-SAFIRE image. The image quality was assessed based on the contour sharpness of the superior mesenteric artery (SMA). Two readers rated image quality as point 2 (good) on (a), point 1 (poor) on (b) and point 3 (excellent) on (c).
Conspicuity of the dilated MPD and cysts
The conspicuity points assigned by the two readers are shown in Table 2.
| Reader 1 | Reader 2 | ||||||
|---|---|---|---|---|---|---|---|
| A.120kVp-FBP images |
B.80kVp-FBP images | C.80kVp-SAFIRE images | A.120kVp-FBP images |
B.80kVp-FBP images | C.80kVp-SAFIRE images | ||
| Dilated MPD | 5 mm | 4.2 | 4.3 | 4.8 | 4.4 | 4.3 | 4.8 |
| P value | 1.000(A vs. B) | 0.043(B vs. C) | 0.043(C vs. A) | 0.463(A vs. B) | 0.043(B vs. C) | 0.109(C vs. A) | |
| Cysts | 5 mm | 3.8 | 3.6 | 4.4 | 3.9 | 3.7 | 4.5 |
| P value | 0.423(A vs. B) | 0.018(B vs. C) | 0.091(C vs. A) | 1.000(A vs. B) | 0.018(B vs. C) | 0.043(C vs. A) | |
| 10 mm | 4.3 | 4.2 | 4.9 | 4.3 | 4.4 | 4.9 | |
| P value | 0.423(A vs. B) | 0.018(B vs. C) | 0.043(C vs. A) | 0.715(A vs. B) | 0.043(B vs. C) | 0.043(C vs. A) | |
| 15 mm | 4.4 | 4.4 | 5.0 | 4.5 | 4.7 | 5.0 | |
| P value | 1.000(A vs. B) | 0.043(B vs. C) | 0.028(C vs. A) | 0.500(A vs. B) | 0.110(B vs. C) | 0.068(C vs. A) | |
Table 2: Mean conspicuity points of the dilated mpd and cysts.
The mean conspicuity point for the dilated MPD and 5, 10 and 15- mm cysts in the normal phantom was consistently 1 (definitely absent) in both readers. With regard to the conspicuity of the dilated MPD and all cysts in the abnormal phantom, 80 kVp-SAFIRE images acquired higher point scores than 80 kVp-FBP and 120 kVp-FBP images for both readers (Figure 4); there were significant differences concerning the conspicuity points for all lesions for reader 1. In the case of reader 2, there were significant differences concerning the conspicuity points between 80 kVp-SAFIRE and 80 kVp-FBP images with regard to the dilated MPD, 5-mm and 10-mm cysts and concerning the conspicuity points between 80 kVp-SAFIRE and 120 kVp-FBP images with regard to all of the cysts. The interobserver agreement between the two readers for the mean conspicuity points of the dilated MPD and the 5, 10 and 15-mm cysts using all three protocol images had moderate to almost perfect agreement (120 kVp-FBP images, κ = 0.55, 0.57, 0.41 and 0.48, respectively; 80 kVp-FBP images, κ = 1.00, 0.84, 0.67 and 0.43, respectively; 80 kVp-FBP images, κ = 1.00, 0.81, 1.00 and 1.00, respectively).
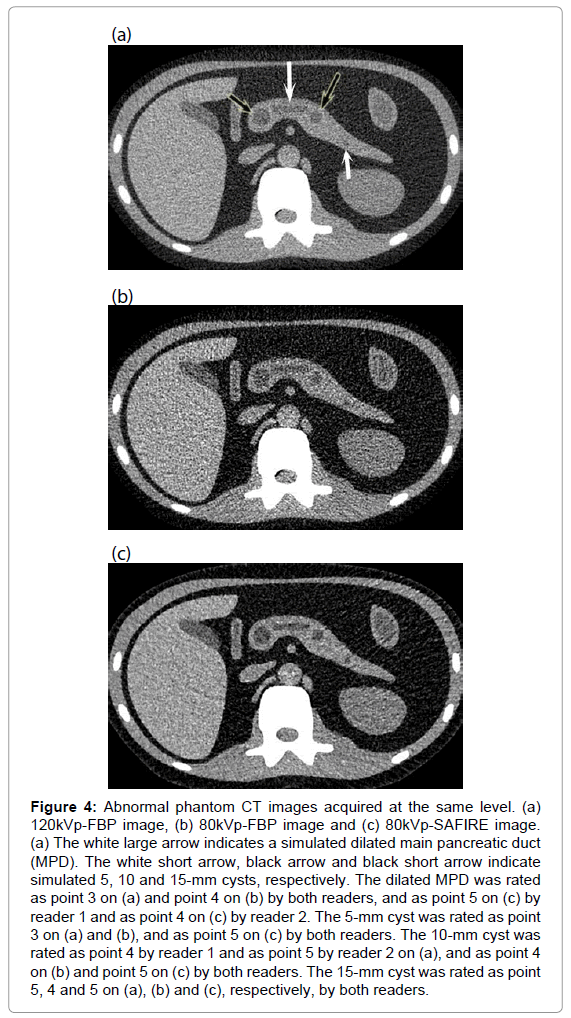
Figure 4: Abnormal phantom CT images acquired at the same level. (a) 120kVp-FBP image, (b) 80kVp-FBP image and (c) 80kVp-SAFIRE image. (a) The white large arrow indicates a simulated dilated main pancreatic duct (MPD). The white short arrow, black arrow and black short arrow indicate simulated 5, 10 and 15-mm cysts, respectively. The dilated MPD was rated as point 3 on (a) and point 4 on (b) by both readers, and as point 5 on (c) by reader 1 and as point 4 on (c) by reader 2. The 5-mm cyst was rated as point 3 on (a) and (b), and as point 5 on (c) by both readers. The 10-mm cyst was rated as point 4 by reader 1 and as point 5 by reader 2 on (a), and as point 4 on (b) and point 5 on (c) by both readers. The 15-mm cyst was rated as point 5, 4 and 5 on (a), (b) and (c), respectively, by both readers.
In the studies using a liver phantom including low attenuation lesions, the effect of SAFIRE has been evaluated regarding the optimization of CT imaging of the lesions. Lower image noise and higher conspicuity and CNR of the lesions was demonstrated; this eventually allowed for a reduction in the radiation dose ranging from 25% to 70 % relative to FBP algorithms [21-24]. Choi et al. reported that SAFIRE at strengths of S3 and S5 allowed the radiation dose to be reduced by 36% and 60%, respectively without image degradation, using a phantom designed to mimic the pancreas (including small pancreatic lesions) during the pancreatic parenchymal phase on contrast-enhanced CT. To our knowledge, there have been no previous studies concerning the diagnostic utility of reduced radiation dose non-contrast-enhanced CT with IR, for the assessment of the dilated main pancreatic duct and pancreatic cysts as predictive signs of the subsequent development of pancreatic cancer.
In our study, the mean image noise in the 80 kVp-FBP images was significantly higher than in the 120 kVp-FBP images and 80 kVp- SAFIRE images. This is due to the effect of lower tube voltage compared with 120kVp-FBP, and image noise reduction in the 80 kVp data through the use of SAFIRE. The CNRs of 120 kVp-FBP images and 80 kVp-SAFIRE images are significantly higher than that of 80 kVp- FBP images. This is because of the lower noise in the 120 kVp-FBP images than in the 80 kVp-FBP images. Furthermore, the CNR of the 80 kVp-SAFIRE images is higher than that of the 120 kVp-FBP images despite the higher image noise in the former, because of the increased contrast as a result of the lower tube voltage and the use of SAFIRE. The image quality was assessed based on the contour sharpness of the SMA. 80 kVp-FBP images had significantly lower image quality than 120 kVp-FBP and 80 kVp-SAFIRE images for both readers. This was thought to be because the 80 kVp-FBP images showed poorly defined SMA contours as a result of the high image noise and low CNR. Image quality in the 80 kVp-SAFIRE images was equivalent to that in the 120 kVp-FBP images for both readers. This is explained by the effect of SAFIRE, which reduces image noise and improves the sharpness of imaging [33]. The conspicuity points of the dilated MPD, and 5, 10 and 15-mm cysts for both readers were higher in the 80 kVp-SAFIRE images than in the 80 kVp-FBP and 120 kVp-FBP images; in addition, there were significant differences concerning the conspicuity points for all lesions for reader 1, and for reader 2 regarding the conspicuity points of the 5 and 10-mm cysts. This is explained by the effects of SAFIRE, which reduces image noise and increases the CNR. The 80 kVp-FBP images had an equivalent conspicuity point to the 120 kVp-FBP images regarding the dilated MPD and all cyst sizes. Although 80 kVp-FBP images had significantly higher image noise and lower CNR relative to 120 kVp-FBP images, these images had equivalent conspicuity points by being offset by increased contrast as a result of the effects of lower tube voltage. Regarding both the quantitative (image noise and CNR) and qualitative (image quality and lesion conspicuity) analyses, SAFIRE allowed the radiation dose to be reduced by 60% without degrading image quality compared with the FBP algorithm.
In the study by Canto et al. the detectability for the small, predominantly cystic, pancreatic lesions was lower on CT images (11%) compared with endoscopic ultrasonography (42.6%) and magnetic resonance imaging including cholangiopancreatography (33.3%) [34]. However, in our study, high conspicuity point (mean; 4.8; range, 4.4–5.0) could be obtained on 80 kVp-SAFIRE images. Detailed comparison of the results between two studies could not be conducted because their methods were different. Thus, further investigations are needed for the confirmation of our study.
Our study had several limitations. First, it entailed an ex vivo study design. However, using the phantom it was possible to obtain a similar effective radiation dose to those in human studies because the phantom included abdominal organs that more closely resembled those in the human abdomen than those in previously published phantoms. Second, a recognition bias concerning lesion conspicuity cannot be ruled out completely; however, we attempted to reduce bias by blinding the readers to the scanning protocol and by organizing the data in a random order that differed for each reader.
The non-contrast-enhanced 80 kVp-SAFIRE CT protocol allowed for higher objective and subjective image quality, higher conspicuity of the dilated MPD and cysts at a reduced radiation dose (60%) compared with a standard 120 kVp-FBP protocol; thus, it appears to be a promising method for screening examination of high risk pancreatic cancer patients.
Siemens Japan provided financial support for developing and purchasing an abdominal phantom. None of the authors has any financial interests with that company, and all authors maintained control of all data presented.