Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2015) Volume 4, Issue 1
Background: On 31st August, 2014, eighty cases of the gastroenteritis were reported in Ghallour sub-centre area. We investigated the outbreak to identify the source, propose control and preventive measures.
Materials and methods: We defined a case as occurrence of three or more watery stools with or without vomiting, w.e.f 27 January, till 2nd Feb2014 in residents of Ghallour sub-centre area of Jawalamukhi Block. We hypothesized it as a water borne outbreak. We determined age and sex specific attack rate. We collected information about personal history on age, sex, residence, and date of onset of symptom from case patient and established line list. We collected 9 stool samples/rectal swabs from the cases; 3 pre and 4 post chlorination water samples and sent them for microbiological testing. We mapped water supply pipelines of the area and reviewed water chlorination record.
Results: We identified 390 cases. The overall attack rate was 8% with range of 1.3% to 36%. The cases patients were reported from all age groups and both the genders with the youngest student; 1 year old to the oldest one as 88 years. Two thirds of the cases reported vomiting with some complaining of pain abdomen. Villages like Jathman, Khattni, Rajol Patta, Kohara has 100% case patients of loose motions while villages like Dhroli, (100%), Sasan (63%) and Ghallour (50%) etc have combined symptoms of loose motions and vomiting. No fatality was reported. Escherichia coli was detected in the samples from water samples. Records of chlorination were not properly maintained.
Conclusion/recommendation: The outbreak was caused due to contamination of water at the source in Jolly Khad. Regular treatment of the water needs to be done right at the source before being lifted.
<Keywords: Epidemic; Watery diarrhea; Coliform bacteria; Public health issue; Kangra
In India, diarrheal diseases are not only a major public health problem not only among children under the age of five but also in adults in the lower belt of Himachal Pradesh, including, Hamirpur, Una, and especially Kangra where heavy rain falls are seen every year. Since diarrheal diseases are caused by 20 to 25 pathogens, vaccination, though an attractive disease prevention strategy, is not feasible. However, as the majority of diarrheas are caused by V. cholerae, Shigellae dysenteriae Type 1 and Enterotoxigenic Escherichia coli which have high morbidity and mortality [1]. In Himachal Pradesh, the burden of infectious diseases continues to be high (respiratory diseases-23.5%; diarrhoeal diseases-14.5% and road traffic accidents at curves-10.5%). In Kangra, the frequent uninvestigated outbreaks of gastroenteritis in summer were 11 in number in 2007 [2]. The watery diarrhoeal outbreak investigation of gastroenteritis in Ghallour subcentre provided us with an excellent opportunity to investigate the case patients with the youngest student is 1 year old to the oldest one as 88 years; with the total of 390 cases.
We investigated the outbreak with the following objectives: (1) confirming the existence of the outbreak, (2) identifying the source and mode of transmission, and (3) initiating control and preventive measures.
On 31st Jan 2014, a news article reported an outbreak of gastroenteritis in Ghallour sub-Centre area, Jawalamukhi block, district Kangra followed by a female health worker, in-charge health center Ghallour under Jawalamukhi block of district Kangra-Himachal Pradesh informed telephonically to health supervisor on dated 30/01/2014 at 9:45 am about 100-125 case patients of loose motions and vomiting. First and information report (FIR) was lodged to block health authorities and investigation was initiated in 1st February, 2014. This epidemic covered the sixteen villages within a radius of 10 kms from block headquarter-Jawalamukhi. Affected villages and distance from block head quarter have been labeled as follows:
Jawalamukhi to village Sasan: 9 km; village Sasan to village Banna; 1 km; village Banna to village Bharoli Ghallour: 1 km; village Bharoli (Ghallour) to village Bhagour; 1.5 km; village Bhagour to village Ghallian Bala; 1 km; vill Ghallian to vill Rukwal Lahar and Bhagera;1.5 km; vill Rukwal Lahar to vill Daryala; 1.5 km and village Daryala to village Daroli, Nand; 1.5 km.
Descriptive epidemiology
We defined a case as occurrence of three or more watery stools with or without vomiting, w.e.f 27 January, till 2nd Feb 2014 in residents of Ghallour sub-centre area of Jawalamukhi Block, Kangra. We defined the probable case patients as the case patients reporting with watery diarrhea and the confirmed case patient as the suspected case patient in whom laboratory investigation confirms the presence of one or more water borne pathogens in a clinical specimen Case search was made by door to door search having obtained informed consent from the case patients for this study. We collected information about personal history on age, sex, residence, and date of onset of symptom from case patient and established line list.
Laboratory investigations: We collected 9 stool samples/rectal swabs from the cases; 3 pre and 4 post chlorination water samples and sent them for microbiological testing to Doctor Rajinder Prasad government medical college, Kangra at Tanda under cold chain.
Environmental Survey: We mapped water supply pipelines of the area and reviewed water chlorination record. Epidemic curve was constituted so as to chart out the development of the outbreak over time. Spot map and area map were charted out. We conducted an unmatched case control study to test the hypothesis that the outbreak occurred due to contamination in the public distribution system (irrigation and public health department water). Data analysis was done by calculating attack rates by age and sex using population of subcentre area. We entered and analyzed the data using a microsoft excel spreadsheet and epics info, version 3.3.2. However, this investigation was conducted in the context of a public health response to an outbreak and therefore an ethical committee review was not indicated.
From our study, we identified 390 cases from the area of sub-centre Ghallour of Jawalamukhi block. The overall attack rate was 8% with range of 1.3% to 36% (Tables 1 and 2). Cases were reported from all age groups and both genders with the youngest student; 1 year old to the oldest one as 88 years. Sasan was first village to be afflicted with outbreak and index male case ageing 47 years became down with an attack of loose motions and painful abdomen and thereafter spread to the neighbouring villages like Bhana, Dhroli, Dodan, Gahllian, Ghallour, Jathman and so on. (Spot maps (i, ii and iii)) Two thirds of the cases reported vomiting with some complaining of pain abdomen. Villages like Jathman, Khattni, Rajol Patta, Kohara has 100% case patients of loose motions while villages like Dhroli, (100%), Sasan (63%) and Ghallour (50%) etc have more of the case patients suffering from combined symptoms of loose motions and 10% of the cases with bloody motions and vomiting (Figure 1). The health teams from district and block level hospitals provided treatment and health education in all the areas. Four cases were admitted in health institutions. There were no deaths. 57 cases reported symptoms on 29th of January which peaked with 311 cases on 30th January and thereafter the number cases came down rapidly. There was generation of single peak which indicated a point source epidemic. The peak tapered off suddenly as the 31st Jan 2014 till 2nd Feb14 and there was no case reported thereafter after free two incubation period (Figure 2-epi curve).
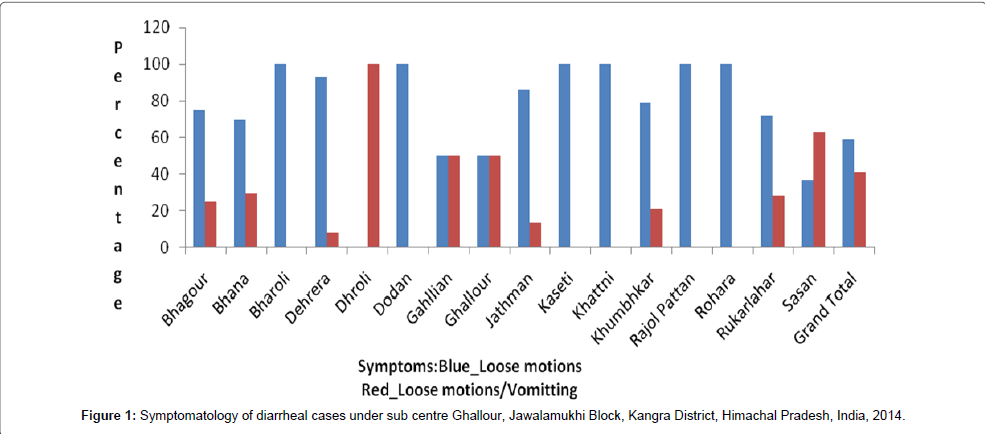
Figure 1: Symptomatology of diarrheal cases under sub centre Ghallour, Jawalamukhi Block, Kangra District, Himachal Pradesh, India, 2014.
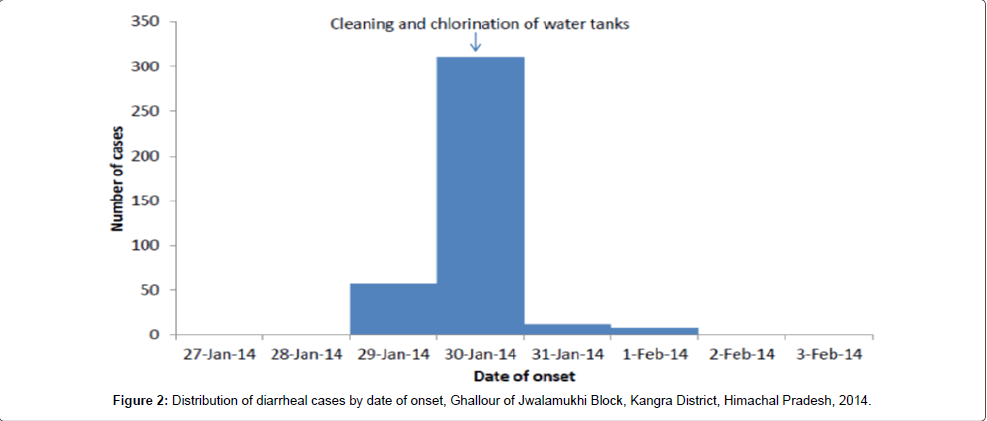
Figure 2: Distribution of diarrheal cases by date of onset, Ghallour of Jwalamukhi Block, Kangra District, Himachal Pradesh, 2014.
| Village | Cases | Population | Attack rate (%) |
| Bhagour | 49 | 300 | 16.3 |
| Bhana | 111 | 536 | 20.7 |
| Bharoli | 04 | 258 | 1.6 |
| Dehrera | 14 | 266 | 5.3 |
| Dhroli | 32 | 160 | 20.0 |
| Dodan | 01 | 185 | 0.5 |
| Gahllian | 06 | 320 | 1.9 |
| Ghallour | 81 | 224 | 36.2 |
| Jathman | 07 | 243 | 2.9 |
| Kaseti | 10 | 251 | 4.0 |
| Khattni | 01 | 324 | 0.3 |
| Khumbhkar | 14 | 142 | 9.9 |
| RajolPattan | 01 | 153 | 0.7 |
| Rohara | 02 | 157 | 1.3 |
| Rukarlahar | 07 | 119 | 5.9 |
| Sasan | 48 | 261 | 18.4 |
Table 1: Attack rate of diarrheal cases in affected 16 villages under sub centre Ghallour, Jawalamukhi Block, Kangra District, Himachal Pradesh, India, 2014.
| Characteristics | N | N | Attack rate (%) | |
| Age group | 0-5 | 43 | 447 | 10 |
| 5+ | 345 | 4691 | 7 | |
| Gender | Male | 185 | 2733 | 7 |
| Female | 203 | 2314 | 9 | |
| Total | 388 | 5138 | 8 |
Table 2: Attack rate of diarrheal cases by age and gender, sub centre Ghallour, Jawalamukhi Block, Kangra District, Himachal Pradesh, India, 2014.
The whole area received water from a source in “Jolly Khad”. At the source the water is collected from a tube well and a dug well. It is lifted to area of sub-Centre Ghallour without treatment and subsequently chlorinated in the tanks further down the line. The dug well is located on the bank of a stream where people frequently defecate in open field. The water sample collected pre-chlorination was found to have recent heavy contamination with up to 1600 colonies of E. coli per 100 ml of water (Table 3). Records of chlorination were not properly maintained. The exact reason for this recent contamination could not be ascertained. A precise microbiological diagnosis was not possible. The distribution of cases over time suggested a common source outbreak. Our bacteriological investigations led to the identification of one pathogen. E. coli which was a generic isolation in the absence of characterization of the strain involved (EPEC, ETEC serotype O157 H7). Serotype O157 H7 is usually found in multiple food outbreaks but this E. Coli also survives in water and several outbreaks have been linked to contaminated water used for different purposes such as swimming in contaminated lakes, drinking contaminated water. Experience from the outbreaks underscores the necessity of using sensitive laboratory isolation methods, such as those used in these outbreaks, for detecting E. coli O157:H7 from livestock feces and agricultural environmental samples [3,4]. In the present outbreak water was lifted from khud water which was contaminated with fecal matter. People defecated in the morning near the khud banks. This untreated water was used for drinking purpose during those days of outbreak. It is further discussed that further testing could not be carried out at the local medical college microbiology laboratory because the frozen stools, sweeps, or isolates were not stored and the facilities were not available. That was the limitation of the study.
| S. No. | MOST PROBALE NUMBER (MPN)/100 COLIFORMS | QUALITY OF WATER |
| 1. | Zero/100 ml of water | Excellent |
| 2. | 1-3/100 ml of water | Good |
| 3. | 4-9/100 ml of water | Suspicious |
| 4. | 10 or >10/100 ml of water | Unsatisfactory |
| Presence of single Escherichia coli | Unsatisfactory |
Table 3: McCredie’s Tables for examination of water, milk, food and air (Source: A book of Mackie and McCartney Practical Medical Microbiology, 14th edition, page no.883-921).
The analytical study indicated that the odds of developing the illness were 13 times higher among individuals drinking water from public distribution supply water as compared to those consuming water from other sources. Local authorities chlorinated all water tanks in the area, following which the number of cases abruptly declined.
The outbreak was caused due to contamination of water at the source in Jolly Khad.
Regular treatment of the water needs to be done right at the source before being lifted.
The water tanks were cleaned and water chlorinated. Health teams were formed to institute treatment and impart health education. Active and passive surveillance was stepped up.
We gratefully acknowledge the cooperation we received in the investigation of this outbreak from the patients and their families and numerous individuals in Jawalamukhi block Kangra); health department, Kangra at Dharamshala, and laboratory support from microbiology department, Dr. Rajinder Prasad Govt. Medical College, Kangra-Himachal Pradesh.