Journal of Cancer Science and Research
Open Access
ISSN: 2576-1447
ISSN: 2576-1447
Case Report - (2018) Volume 0, Issue 0
Keywords: Lung cancer; Invading the spine; Lobectomy; Vertebrectomy
Surgical treatment for lung cancer invading the spine remains challenging. En bloc vertebrectomy with lung and chest wall is ideal. However, if the volume of lung cancer is large, en bloc resection is very difficult. We herein report successful radical resection for large lung cancer invading the spine by dividing the procedures into lobectomy and total vertebrectomy safety.
A 65-year-old man who had a 2-year history of chest abnormal shadow detected by a medical examination was admitted to our hospital. Chest computed tomography (CT) and magnetic resonance imaging (MRI) revealed a tumor (50×50 mm) in S1 of the right lung invading from the fourth to the fifth thoracic vertebra and from the fourth to the sixth rib (Figure 1A and 1B). Furthermore, aberrant V2 was detected on CT (Figure 1C). Nodal and distant metastases were not detected on positron emission tomography - CT or brain MRI. Adenosquamous cell carcinoma was detected by transbronchial lung biopsy. We diagnosed the lung cancer as clinical stage IIIA (cT4N0M0) and planned a primary surgery.
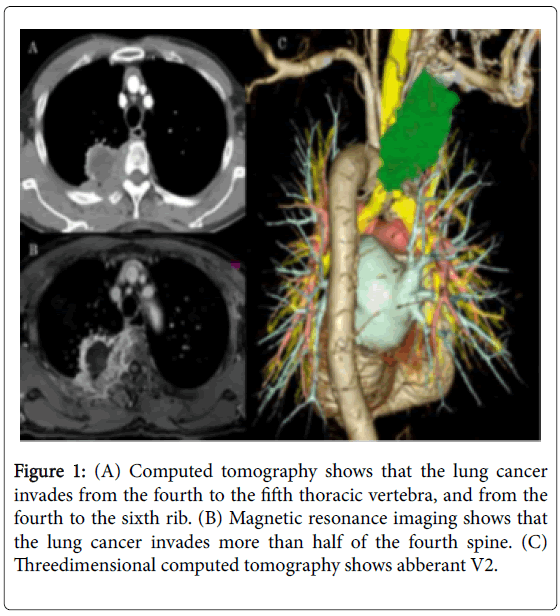
Figure 1: (A) Computed tomography shows that the lung cancer invades from the fourth to the fifth thoracic vertebra, and from the fourth to the sixth rib. (B) Magnetic resonance imaging shows that the lung cancer invades more than half of the fourth spine. (C) Threedimensional computed tomography shows abberant V2.
The operation was started in the lateral position. We performed video-assisted thoracic surgery (VATS) to confirm no pleural dissemination and then performed right upper lobectomy with partial resection from the fourth to the sixth rib by posterolateral thoracotomy. Because en bloc resection of the lung, chest wall, and vertebrae was difficult due to the large size of the tumor, we planned to perform intralesional resection and removed the right upper lobe. In this stage, aberrant V2 was sutured at interlober. Prior to the right upper lobectomy, the right upper lobe was interrupted temporarily and there was no congestion of residual lesion (Figure 2A).
Therefore, intralesional resection and the right upper lobectomy were performed. Subsequently, total vertebrectomy from the fourth to the fifth thoracic vertebra with lung cancer and chest wall was performed by a posterior midline incision in the prone position (Figure 2B and 2C).
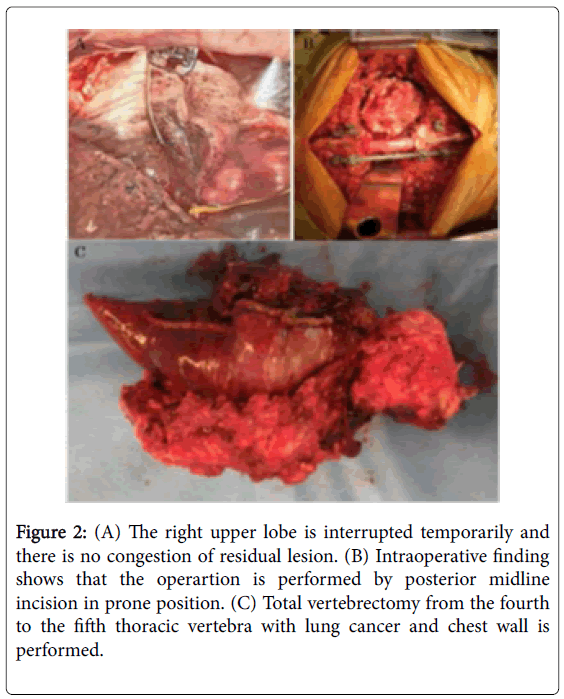
Figure 2: (A) The right upper lobe is interrupted temporarily and there is no congestion of residual lesion. (B) Intraoperative finding shows that the operartion is performed by posterior midline incision in prone position. (C) Total vertebrectomy from the fourth to the fifth thoracic vertebra with lung cancer and chest wall is performed.
A titanium mesh case with self-bone grafting was implanted, and posterior thoracic spinal fusion was performed (Figure 3). The patient was discharged home on the 18th postoperative day without the paralysis.
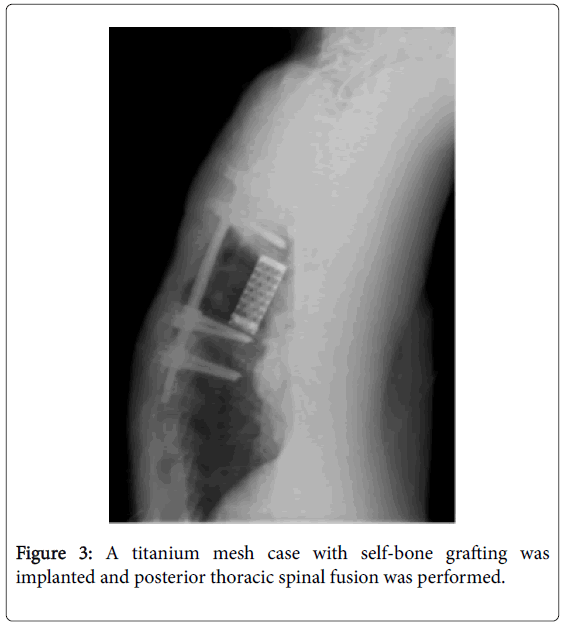
Figure 3: A titanium mesh case with self-bone grafting was implanted and posterior thoracic spinal fusion was performed.
Historically, lung cancers invading the spine have generally been considered unresectable and fatal [1]. However, several reports showing the efficacy of surgical resection for lung cancer invading the spine have been published since the 2000s [2-5]. The 5-year overall survival rate has ranged from 57% to 71.4% [4,5]. Induction therapy is considered necessary to control tumor recurrence [2,4], on the other hand it has been reported that induction therapy is not useful for lung cancer invading the spine [5]. In our case, induction therapy was not performed because we considered complete resection to be achievable without induction therapy, and spinal cord invasion might have occurred if induction therapy had proven to be ineffective.
Total vertebrectomy may be difficult by posterolateral thoracotomy alone, so a posterior midline incision may additionally be required. En bloc resection of the lung, chest wall, and vertebrae is ideal. However, if the volume of the lung cancer is large, en bloc resection may be difficult. In our case, surgical resection was performed by dividing the procedure into lobectomy via a posterolateral incision and total vertebrectomy via a posterior midline incision because en bloc resection was considered difficult due to the large volume of the lesions in the lung, chest wall, and vertebrae.
If there is collateral circulation from chest wall to lung lesion, congestion of residual lesion may be occurred by dividing the procedures into lobectomy and vertebrectomy. We confirmed that the right upper lobe was interrupted temporarily and there was no congestion of residual lesion prior to the right upper lobectomy. The clamping technique is considered important in dividing the procedures into lobectomy and vertebrectomy.
In many cases, aberrant V2 is sutured at pulmonary hilum. However, aberrant V2 was sutured at interlober in this case, as suturing the aberrant V2 at the pulmonary hilum was deemed extremely difficult due to the large size of the lesion and invasion of the spine.