Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Research Article - (2015) Volume 4, Issue 1
The psychostimulant methylphenidate (MPD) is the pharmacotherapy of choice for the treatment of attention deficit disorder (ADD), attention deficit hyperactivity disorder (ADHD), narcolepsy, dementia, chronic fatigue and useful in providing relief from intractable pain. More recently students of all ages use MPD (Ritalin) as a cognitive enhancement to help them study and perform better during exams. Many of them abuse the drug for recreation. This chapter aims to provide a short review of the pharmacological property of MPD. MPD can elicit behavioral sensitization or tolerance – behavioral sensitization and tolerance are experimental markers indicating dependence. Some behavior experiments using an MPD dose response protocol demonstrated that MPD elicits behavioral sensitization and other studies reported behavioral tolerance. Our dose response study of chronic MPD dose response experiment demonstrated that the same dose of MPD in some animals elicited behavioral sensitization and in others animals behavioral tolerance.
<Keywords: Methylphenidate; Ritalin; Behavioral sensitization; Behavioral tolerance; Neurotransmitters; Neurodevelopmental; Acute; Chronic
The psychostimulant methylphenidate is the first line of pharmacotherapy treatment for attention deficit disorder (ADD), attention deficit hyperactivity disorder (ADHD), narcolepsy, memoryimpairment (dementia) in older individuals, and chronic fatigue [1]. Psychostimlant medication such as amphetamine was used to treat ADD and ADHD patients from the 1930’s until it was found that it elicited dependence. The psychostimulant methylphenidate has since become the drug of choice for ADD and ADHD patients [2].
Methylphenidate (MPD) is used by children and young adults during their developmental stages where overproduction and synaptic pruning in the central nervous system (CNS) occurs which may have an effect on the developing brain. Youth are striking deals to buy and sell MPD (Ritalin) to improve their brain functions and for recreation, while the number of fatalities associated with its misuse has risen to record levels. MPD has similar rapid uptake in the brain to that of cocaine and amphetamine, but differs from them by having a much lower rate of clearance from the brain. Intravenous (i.v.) or intranasal administration of MPD has a higher mortality rate than cocaine or amphetamine [3].
Pharmacological property of Methylphenidate (MPD)
MPD is administered as a racemic mixture of the d-and l-threoenantiomers; however, the d-enantiomer is thought to be the primary responsible for its therapeutic effects. When MPD is given orally, it is absorbed from the intestinal tract and has a half- life of about 1 hour with equally short duration and efficacy. The dose and route of MPD administration are important because the features of the behavioral and neurochemical responses to the drug are dependent on the speed of the drug to reach peak level, i.e. the rise time of the drug concentration. Peak levels of MPD following intravenous (i.v.), intraperitoneal (i.p), and oral administration was 8-20 min, 15-28 min, and 60-90 min, respectively [4,5]. Similar peak levels of i.v., i.p., and oral administrations were obtained following amphetamine and cocaine [4]. The ability to reach peak levels in short spans of time (i.e. 8-30 min) is one of the main factors in eliciting adverse effects such as sensitization. MPD given systematically binds with similar affinity at the dopamine transporter (DAT) and has potency (Ki=200) similar to cocaine (Ki=224) [5]. The relationship between drug doses (milligrams of hydrochloride salt/kilograms of body weight) and percentage occupancy of DAT is identical for cocaine and MPD in rodents and humans [6]. MPD is absorbed and metabolized via deetherification to ritalinic acid and released into the urine within 48 hours. Brain concentration of MPD exceeds that of plasma since the psychostimulants are concentrated in catecholaminergic systems with free passage across the blood brain barrier. MPD has a similar uptake in the brain as cocaine, but differs from cocaine by having a much lower rate of clearance from the brain. The outcome of MPD treatment results primarily in preventing the reuptake of dopamine (DA), norepinephrine (NE), and serotonin (5HT) from the synaptic cleft to the presynaptic terminals. Like cocaine, MPD is an indirect catecholamine (CA) agonist since it does not stimulate the catecholaminergic receptors directly, but rather facilitates the action of the CA [6,7]. The therapeutic effect of MPD in the treatment of ADHD has been attributed to its ability to increase the efflux of these neurotransmitters. This causes increases in extracellular DA, NA, and 5HT levels [5], which have an effect that has been linked to its reinforcing properties. MPD has moderate effects on the peripheral circulatory system. In rats, acute MPD administration in low doses (1-3 mg/kg) stimulates locomotor activity, and in high doses (10 mg/kg and higher) further increases in locomotion occur, and it also stimulates stereotypical behavior [8,9]. Following its repetitive (chronic) use it can elicit either behavioral tolerance or behavioral sensitization [10-12].
Behavioral tolerance is defined by the following criterion: repetitive exposure with the same dose of MPD will become less effective to elicit its initial effects. Behavioral sensitization is defined as reverse tolerance, i.e. repetitive exposure with the same MPD dose will elicit a significant further increase in its behavioral effects compared to that elicited by the initial (acute) dose. Behavioral sensitization and/or tolerance is considered a long lasting neuroplasticity elicited following repetitive psychostimulant exposure. It has been suggested that behavioral tolerance and sensitization represent an enduring alteration of drug response and have been used as an experimental model of drug craving [13].
Does MPD elicit tolerance or sensitization?
One of the most used assays to study animal behavior is the open field assay (Figure 1). Open field assays were introduced more than 80 years ago. It resembles a natural behavioral pattern and is one of the most widely used methods in animal behavioral research. Its popularity stems from the simplicity of the apparatus and clearly defined behaviors. Certain measurable motor behaviors are sensitive to a wide range of drugs and experimental manipulations and are sufficiently reliable under standardized conditions to give repeatable measures on an enormous range of independent variables. Simplicity, reproducibility (Figure 2), ease of quantification, and wide applicability are the prime determinants of its popularity. Open- field locomotor behaviors represent the interaction of the subject with the experimental situation. Most investigators study the effects of psychostimulants in open-field testing whether repetitive (chronic) drug exposure elicits behavioral tolerance or behavioral sensitization. Since drug liability is defined mainly on the basis of the subject behavioral response to drug exposure such as behavioral withdrawal, sensitization or tolerance. Behavioral expressions after psychostimulant administration develop gradually and progressively during the course of repeated exposure of psychostimulants, and this expression can persist for long periods of time after its discontinuation [14]. Thus, withdrawal, sensitization, and tolerance are considered a form of drug induced neuronal plasticity and are used as an experimental model and as a marker for drug effects, and for its liability for abuse.
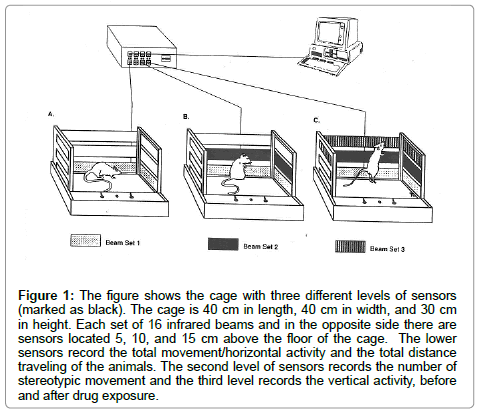
Figure 1: The figure shows the cage with three different levels of sensors (marked as black). The cage is 40 cm in length, 40 cm in width, and 30 cm in height. Each set of 16 infrared beams and in the opposite side there are sensors located 5, 10, and 15 cm above the floor of the cage. The lower sensors record the total movement/horizontal activity and the total distance traveling of the animals. The second level of sensors records the number of stereotypic movement and the third level records the vertical activity, before and after drug exposure.
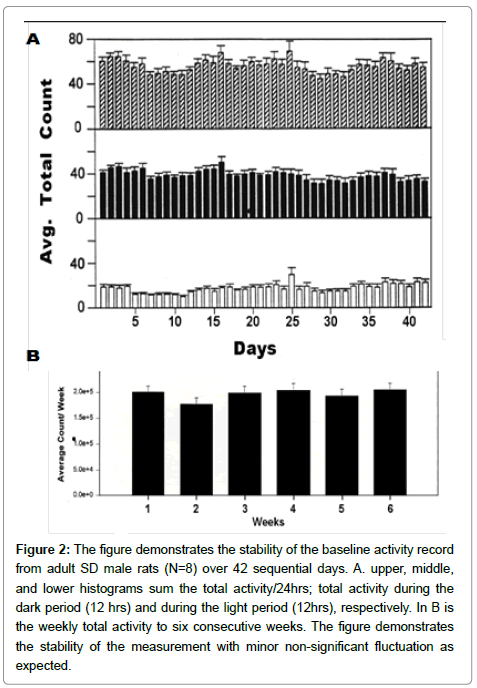
Figure 2: The figure demonstrates the stability of the baseline activity record from adult SD male rats (N=8) over 42 sequential days. A. upper, middle, and lower histograms sum the total activity/24hrs; total activity during the dark period (12 hrs) and during the light period (12hrs), respectively. In B is the weekly total activity to six consecutive weeks. The figure demonstrates the stability of the measurement with minor non-significant fluctuation as expected.
In a dose response experiment using chronic 0.6, 2.5, and 10.0 mg/kg i.p. MPD, sometimes the groups (N=8) exhibited sensitization (Figure 3), sometimes expressed no effect of drug, and in few cases to 10.0 mg/kg MPD tolerance was observed [15,16]. This varied response forced us to increase the number of animals per group until a significant effect of the drug was obtained. Moreover, this observation suggests that the same dose of MPD can elicit behavioral tolerance in some animals and behavioral sensitization in others. To test this possibility, i.e. that the same repetitive (chronic) dose of MPD can elicit behavior sensitization in some animals and behavioral tolerance in others, the following experiment was conducted.
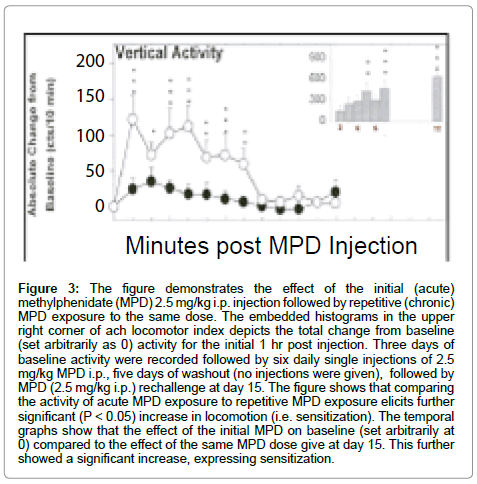
Figure 3: The figure demonstrates the effect of the initial (acute) methylphenidate (MPD) 2.5 mg/kg i.p. injection followed by repetitive (chronic) MPD exposure to the same dose. The embedded histograms in the upper right corner of ach locomotor index depicts the total change from baseline (set arbitrarily as 0) activity for the initial 1 hr post injection. Three days of baseline activity were recorded followed by six daily single injections of 2.5 mg/kg MPD i.p., five days of washout (no injections were given), followed by MPD (2.5 mg/kg i.p.) rechallenge at day 15. The figure shows that comparing the activity of acute MPD exposure to repetitive MPD exposure elicits further significant (P < 0.05) increase in locomotion (i.e. sensitization). The temporal graphs show that the effect of the initial MPD on baseline (set arbitrarily at 0) compared to the effect of the same MPD dose give at day 15. This further showed a significant increase, expressing sensitization.
The experiment uses 166 adult (200-220 gr) male Sprague Dowley rats divided into 4 groups: 1) Saline (N=14); 2) 0.6 mg/kg MPD (N=47); 3) 2.5 mg/kg MPD (N=49) and group 4) 10.0 mg/kg (N=56). The experiment lasted for 10 consecutive days using the open field assay as follow. On experimental day 1 (ED1) saline was injected and behavioral recording were obtained for 60 min followed by either saline (the control group) or 0.6, 2.5, or 10.0 mg/kg MPD, and behavioral recordings were resumed for an additional 60 min. At ED2 to ED6, a single injection of either saline (the control group) or MPD at identical dose as on ED1 was given, followed by 3 washout days (ED7-ED9). At ED10 recording following saline and MPD resume identical to ED1 [8,9,11,12,16].
Activity obtained following MPD administration at ED1 compared to saline given at ED1 provide the acute effect of the drug, and activity following MPD at ED10 compared to activity at ED1 following MPD provide whether the drug elicits behavioral sensitization or tolerance.
To test this possibility, the data was evaluated as followed. All the animals for each dose were grouped into one, group #1, and statistically evaluated for whether the drug elicited behavioral sensitization or tolerance [10-12]. Each individual animal was statistically evaluated to determine whether behavioral sensitization or behavioral tolerance was expressed. Animals expressing behavioral sensitization were placed in group #2, and those expressing behavioral tolerance were summed into group #3.
Figure 4 summarized the two locomotor indices of this experiment and shows that the same repetitive (chronic) dose of MPD elicits behavioral sensitization in some animals and behavioral tolerance in others (Figure 4).
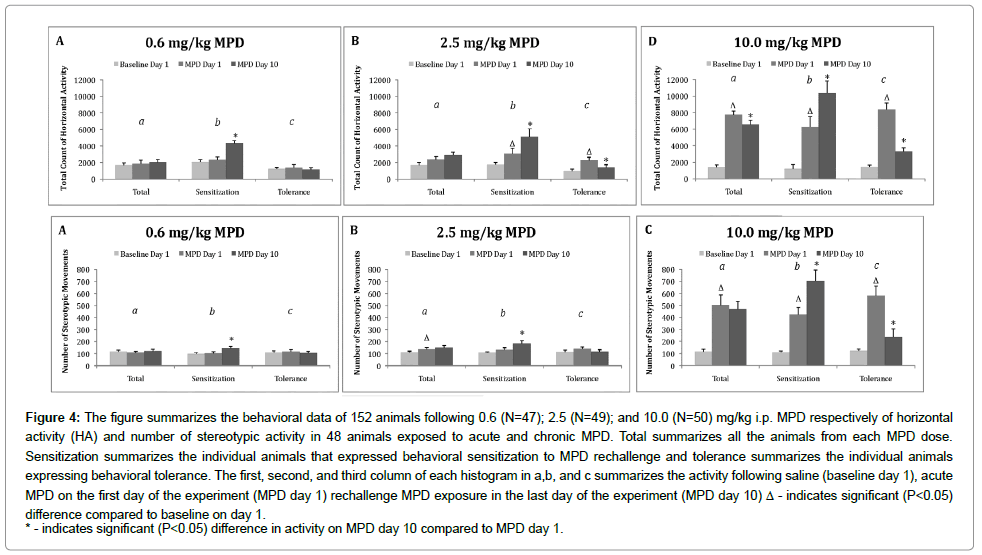
Figure 4: The figure summarizes the behavioral data of 152 animals following 0.6 (N=47); 2.5 (N=49); and 10.0 (N=50) mg/kg i.p. MPD respectively of horizontal activity (HA) and number of stereotypic activity in 48 animals exposed to acute and chronic MPD. Total summarizes all the animals from each MPD dose. Sensitization summarizes the individual animals that expressed behavioral sensitization to MPD rechallenge and tolerance summarizes the individual animals expressing behavioral tolerance. The first, second, and third column of each histogram in a,b, and c summarizes the activity following saline (baseline day 1), acute MPD on the first day of the experiment (MPD day 1) rechallenge MPD exposure in the last day of the experiment (MPD day 10) Δ - indicates significant (P<0.05) difference compared to baseline on day 1.
* - indicates significant (P<0.05) difference in activity on MPD day 10 compared to MPD day 1.
Several articles reported that healthy people deserve the right to boost their brains with psychoactive pills, like those prescribed for Attention Deficit Disorder (ADD), Attention Deficit Hyperactivity Disorder (ADHD), narcolepsy and memory- impaired older folks. College students are already taking MPD (Ritalin), mainly to help them study and to perform better during exams. Some students contend that: We should welcome new methods of improving our brain function and doing it with pills is no more morally objectionable than healthy eating, taking vitamins or getting a good night’s sleep with the help of a remedy. MPD is a psychoactive drug, but what do we know about this psychoactive drug? Psychoactive drug use dates back to prehistoric times: there is archaeological evidence for their use as much as several thousand years ago. A psychoactive drug acts in the central nervous system (CNS) to modulate consciousness, perception, mood and behavior. These drugs were used therapeutically as medication or for ritual and spiritual purposes, as well as recreationally to alter one’s mood and to get ‘high’. Because psychoactive drugs elicit changes in consciousness and mood, the user feels alert, joyful, pleasant, and becomes euphoric. Many psychoactive drugs are used and abused despite the risks of its consequences, such as dependence. MPD (Ritalin) belongs to this family of psychoactive drugs.
Psychostimulant medications such as amphetamine were used to treat attention deficit hyperactive disorder (ADHD) patients from 1930’s until it was found it elicits dependency. The psychostimulants methylphenidate (MPD) has since become the drug of choice to treat ADHD patients. MPD is a CNS stimulant that closely relates to the structure of dextroamphetamine, a derivative of amphetamine [6]. The neuropharmacological profile of MPD is also similar to that of cocaine [6]. The drug was first synthesized in 1944 and used initially as an analeptic for several types of barbiturate-induced comas. Since then, its usage has been extended to improve the alertness in children and adults with emotional, behavioral, and learning difficulties [17]. Treatment of children with MPD for extended periods of time when they are going through neurodevelopmental processes can modulate these critical neurodevelopmental processes that may alter the body’s homeostasis. Moreover, since chronic MPD use can elicit either behavioral withdrawal, sensitization, or tolerance [10-12,16], psychostimulant therapy given to adolescents and young adults may increase the risk for Substance Use Disorder. While, other reports suggest that psychostimulant treatment in adolescence for ADHD protects them from developing a future Substance Use Disorder. These contradictory reports call for basic in-depth studies to resolve this critical issue.
Behavioral sensitization and behavioral tolerance following the same chronic MPD dose of 0.6, 2.5, or 10.0 mg/kg exposure were observed. Expression of behavioral sensitization or tolerance following chronic psychostimulant exposure suggests that the drug has the potential to elicit dependence (addiction).