Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2011) Volume 1, Issue 2
Objective: To determine if three months of chronic daily administration of ulipristal acetate (UPA), a selective progesterone receptor modulator, normalized the uterine cavity in women with leiomyoma.
Methods: Saline sonograms with abnormal uterine cavities from patients participating in a placebo controlled double blind randomized controlled trial evaluating UPA effect on leiomyoma volume were identified prior to initiation of therapy. They were reexamined after 12 weeks of UPA therapy. Normal uterine cavity was defined as having zero percent of leiomyoma volume inside the cavity on repeat sonohysterography. Patients with normal saline sonograms after 12 weeks of UPA therapy were compared with patients with sonographically persistently abnormal uterine cavities. Statistical analysis was performed using the Fisher’s exact test.
Results: 28 patients had abnormal sonohysterogram results at baseline (n= 9, n= 8 and n=11 for placebo, UPA 10 mg and UPA 20 mg respectively). At the end of treatment 22% of the placebo group, 38% of the 10 mg group and 27% of the 20 mg group had normal uterine cavities. When the 10 mg and 20 mg groups were combined, 32% of the patients had normal uterine cavities post treatment. The results did not reach statistical significance.
Conclusion: If future larger, randomized trials demonstrate a benefit, UPA may offer an alternative to surgical therapy for women requiring normalization of the uterine cavity.
<Keywords: Leiomyoma, Selective Progesterone Receptor Modulators, Assisted Reproductive Technologies.
A number of studies, including a prior investigation by our group, have shown that women with fibroids have lower incidence of pregnancy when undergoing treatment with Assisted Reproductive Technologies (ART) [1-4]. It is estimated that women with uterine cavitary abnormalities have an approximately 30 percent decrease in fecundability. Although recent data suggest that small fibroids that do not impact the uterine cavity may not affect outcomes, large fibroids that distort the cavity and submucosal fibroids appear to impair implantation [2]. It is now accepted clinical practice to offer surgical correction of the uterine cavity prior to treatment with ART. Currently, approved pharmacological therapy for uterine leiomyoma is limited to gonadotropin releasing hormone (GnRH) agonists. This therapy is hindered by its transient effect as leiomyomas typically return to pre treatment size. This has limited GnRH agonists to primarily function as presurgical adjunct therapy to minimize operative difficulty. [5] However, this has not been evaluated as a method of leiomyoma control prior to ART. Consequently, effective pharmacologic therapy is unavailable for this purpose and these patients are subjected to additional surgical intervention in the form of hysteroscopy, laparoscopy or laparotomy to normalize the uterine cavity prior to proceeding with ART. Surgical therapy has operative risks and possible obstetrical complications such as uterine rupture. Additionally, most recent, comprehensive review of the literature failed to provide a definitive answer regarding whether myomectomy was beneficial [6].
An effective medical therapy is needed for women who are not surgical candidates and women who would prefer to decline surgical intervention. Selective progesterone receptor modulators (SPRMs) show promise as a potential option for these patients. Previous studies by the authors demonstrated that the progesterone receptor modulator ulipristal acetate (UPA) significantly reduced total fibroid volume [7, 8] and studies with other progesterone receptor modulators also demonstrated a significant reduction in leiomyoma size [9,10].
From these studies, we hypothesized that if selective progesterone receptor modulators decreased leiomyoma size, they would also normalize the uterine cavity. Normalization of the uterine cavity with medical therapy would eliminate an additional surgical procedure in women who are afflicted with an abnormal uterine cavity and require ART. Our objective, in this retrospective review, was to determine if three months chronic daily administration of UPA, would normalize the uterine cavity, as evaluated by saline infusion sonography, in ovulatory women with leiomyoma.
Patients were recruited to participate in a randomized controlled double blind, placebo-controlled trial evaluating the effect of UPA on leiomyomas. Ovulatory women with symptomatic (anemia, pressure symptoms, pain, urinary symptoms or menorrhagia) uterine fibroids greater than 2 cm in diameter were enrolled. Prior infertility or subfertility was not part of the inclusion criteria. The primary outcome of the original trial was change in leiomyoma volume [7,8]. Women aged 33–50 years with symptomatic uterine fibroids were originally randomized to receive oral UPA (10 or 20 mg) or placebo once daily for 12 weeks. Saline sonohysterography (Phillips IU2/Netherlands) was performed on all patients at baseline (Figure 1) and after 12 weeks of administration of UPA or placebo (Figure 2). Measurements were taken in centimeters in 2 dimensions prior to and after instilling 10 to 20 mL of sterile saline into the uterine cavity via a sonohysterogram catheter. Abnormal uterine cavities were defined as having any visible distortion by uterine leiomyoma. Analysis evaluating the effect of UPA therapy on uterine cavity normalization was performed. All patients with abnormal sonohysterography at baseline were identified. The saline sonograms of these patients were then analyzed after 12 weeks of UPA therapy. A normalized uterine cavity was defined as having no evidence of cavitary distortion by leiomyoma (Figure 2). Statistical analysis was carried out using Fisher’s exact test.
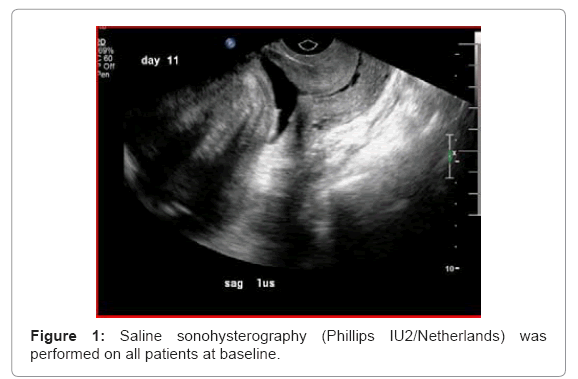
Figure 1: Saline sonohysterography (Phillips IU2/Netherlands) was performed on all patients at baseline.
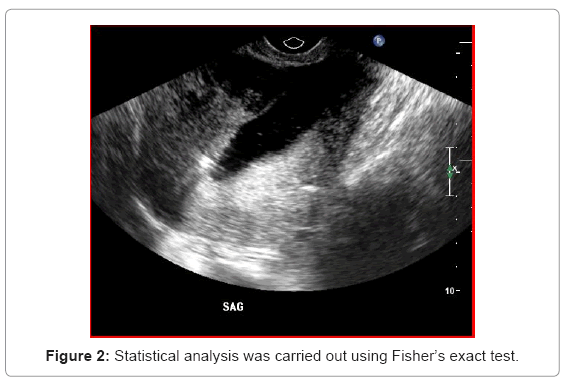
Figure 2: Statistical analysis was carried out using Fisher’s exact test.
Twenty-eight patients were identified to have abnormal sonohysterograms prior to UPA therapy. Nine patients in the placebo group, eight patients receiving 10 mg UPA, and eleven patients who received 20 mg UPA. After completion of treatment with UPA for 12 weeks 22% of the placebo group, 38% of the 10 mg group and 27% of the 20 mg group demonstrated normal uterine cavities when evaluated with sonohysterography. When the 10 mg and 20 mg groups were combined, 32% of the patients had normal uterine cavities after treatment (Table 1). Currently, saline infusion sonography is an established method of evaluation of the uterine cavity prior to ART with excellent sensitivity and positive predictive value for intracavitary leiomyomas. [11] Distorting leiomyoma sizes were individually examined prior to and after 12 weeks of UPA therapy. The original size of the distorting tumor did not affect uterine cavity normalization. The mean leiomyoma size of distorting tumors was similar to leiomyomas with persistently normal uterine cavities. (5.4 x 4.2 x 3.9 vs. 5.0 x 4.6 x 4.1 cm) (p=0.70). Thirteen patients out of the original 42 patients randomized in the trial elected to proceed with UPA therapy for additional 3 months. These patients received their radiographic follow up with MRI. Although the overall fibroid volume continued to decrease, saline infusion sonography was not routinely performed and the benefit of uterine cavity normalization cannot be ascertained for these patients for the additional time.
| Group | Distorted Uterine Cavity | Normal after treatment | % |
|---|---|---|---|
| Placebo | 9 | 2 | 22% |
| UPA 10 mg | 8 | 3 | 38% |
| UPA 20 mg | 11 | 3 | 27% |
| UPA 10+20 mg | 19 | 6 | 32% |
Table 1: Two Tailed Fisher’s Exact.
Historically, the primary and definitive treatment for fibroids has been surgical. As demonstrated by a recent literature review by Pritts et al. [4] there are few prospective randomized trials to guide clinical decision making in medical treatment. Sankaran et al. [12] in 2008 performed an extensive review of medical management of leiomyomas. They concluded that selective progesterone receptor modulators have significant promise and warrant further research, as they appear to show efficacy in inducing fibroid regression without major side effects.
There is evidence to suggest that medical management of uterine leiomyoma can be successful. Initial randomized controlled trials have demonstrated that UPA was well tolerated and was effective in reducing leiomyoma size, addressing gynecologic symptoms and improving quality of life [7,8].
Others have also shown that selective progesterone receptor modulators are effective in reducing leiomyoma size and associated gynecologic symptoms [9]. A randomized controlled trial in 2006 demonstrated the effectiveness of selective progesterone receptor modulator mifepristone [10]. In this investigation, six months of mifepristone therapy was effective in reducing fibroid size and improving quality of life. Carbonell Esteve et al. [13] subsequently confirmed that 90 days of treatment with mifepristone significantly decreased leiomyoma size and uterine volume respectively, and Malartic suggested that many invasive procedures might potentially be avoided with routine use of SPRM in leiomyoma treatment [14].
One of the concerns of using SPRMs is its effect on the endometrium. Early data suggested that asoprisinil was associated with endometrial hyperplasia [15]. More recent studies have suggested that the changes in endometrial histology represented a benign cystic dilatation of the glands and not true hyperplasia. Specifically, a consensus conference was held and eighty-four endometrial specimens of patients receiving one of four different SPRMs were examined. No malignant or premalignant lesions were identified. Due to the novelty of these pathologic findings, new nomenclature was developed and the term progesterone-associated changes in the endometrium or PAEC was coined [16]. These findings are reassuring in regards to the endometrial safety of SPRMs.
Another concern regarding the use of SPRMs is their effect on endometrial receptivity. Currently, it is approved for emergency contraception with its main mechanism of action being a disruption folliculogenesis leading to ovulatory delay [17] and delayed endometrial maturation [18]. While this is effective preventing spontaneous pregnancy, it is likely not relevant in ART cycles where after cessation of UPA therapy, gonadotropin stimulation would serve to build up the endometrial lining and patients are treated with supraphysiologic doses of progesterone prior to and after embryo transfer.
The small sample size is a limitation of this trial. Our intent, in this preliminary report, was to describe that medical normalization of the uterine cavity is possible, not to demonstrate a therapeutic effect. Future sufficiently powered, randomized, controlled trials are needed to demonstrate a therapeutic benefit. Currently there are no published data describing ART after treatment with selective progesterone receptor modulators. Hence the effect of prolonged UPA therapy on ART success and pregnancy is unknown, but it is likely that exposure to oral contraceptive pretreatment, gonadotropin stimulation leading to high estradiol levels and progesterone treatment during the ART cycle, would mitigate UPAs theoretical detrimental effect on the endometrium. The unknown duration of the therapeutic effect after drug discontinuation is another limitation of this report.
This preliminary study demonstrates an improving trend but not a statistically significant rate of uterine cavity normalization with 12 weeks of UPA therapy. Therefore it is unclear if normalization is due to UPA effect or chance alone. The idea of uterine cavity normalization with medical management is important and to our knowledge this was the first study in which application of non-surgical treatment was evaluated as a feasible intervention to normalize the uterine cavity.
This pilot study did not demonstrate that UPA per se normalized the uterine cavity. Larger, randomized trials are necessary to determine if UPA is a viable medical alternative to operative intervention. If such trials demonstrate a clinical benefit, UPA may offer an alternative to surgery for women requiring normalization of the uterine cavity prior to ART.