Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2015) Volume 5, Issue 4
Background: Anti-retro-viral therapy (ART) has changed human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) from fatal disease to chronic illness, it does however requires almost perfect adherence for the medication to be therapeutically effective. Methodology: A study will be conducted among people living with Human Immunodeficiency Virus (PLHIV) aged 18 years and above, who are on ART at the ART center of Kasturba Medical College Hospital (KMCH), Attavar, Mangalore, India. Study consists of two phases: Phase I cross sectional study: A cross sectional study (n=409), has already been done to find out the level of adherence to ART using Adult AIDS Clinical Trials Group adherence follow-up questionnaire and the pre-testing for HIV related knowledge of the participants was done using HIV Knowledge Questionnaire. We observed the prevalence of non-adherence to be 27.1% (n=121) and HIV related knowledge was high among 127 (31.1%) and low among 282 (68.9%) PLHIV. Among the 121 non-adherents, 110 PLHIV will be included in the 2nd phase of the study using block randomization. Phase II randomized controlled trial (RCT): A sample size of 110 will be included in this study, which was calculated based on the statistical formula. Randomization of the participants will be done using block randomization method into intervention and control groups. HIV educational intervention will be provided for six months to the intervention group along with the standard patient care available at the hospital, whereas the control group will receive only the standard patient care available at the hospital for duration of six months. This will be followed by conduction of the first post-test at the end of 6th months among both the groups. The participants will be followed up for next 6 months and second post-test will be done at the end of 12th month for the assessment of study outcomes.
Keywords: Human immunodeficiency virus; Anti retro-viral therapy; HIV educational intervention; Randomized controlled trail
Human Immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is a global health concern. According to The Joint United Nations Programme on HIV/AIDS (UNAIDS), as many as 35.3 million people worldwide and about 4.9 million people in Asia and the Pacific region [1], were affected by HIV/AIDS in the year 2012. According to the National AIDS Control Organization (NACO) report 2011, India has around 2.9 million people living with HIV (PLHIV) with a national prevalence of 0.27% [2] and among them about 0.25 million are living in the state of Karnataka with a prevalence of 0.69% [3].
With the introduction of anti-retroviral therapy (ART) and scaling up of its availability, life expectancy of infected persons has increased. In most of the cases high adherence to ART (>95%) is needed to achieve the therapeutic success [4], suboptimal adherence may lead to the failure of ART [5].
As there is no cure for HIV infection and also non availability of vaccines for its prevention, the PLHIV need to follow ART regimen for life. Other health related challenges includes, managing medication, side effects due to medication, aging etc. Mental illness, most commonly depression is strongly associated with non-compliance and decreased health related quality of life (HRQOL) among PLHIV [6]. Previously, studies have demonstrated the association of depression with socialsupport and self-esteem, thus implying that self-esteem has a positive influence against the development of depression among PLHIV which may also lead to increase in level of adherence to medication [7,8].
Knowledge regarding the HIV disease, manifestations and importance of adherence to ART is crucial for the PLHIV in order to be better informed about the disease and its treatment, which will help them in improving the adherence to ART. PLHIV who were better aware of the HIV disease through HIV educational intervention had shown increase in adherence to ART, better quality of life and better therapeutic outcomes compared to the patients under standard care [9,10].
In this randomized controlled trial, we aim to assess the effectiveness of an educational intervention in improving the level of adherence to ART and change in CD4 count among PLHIV
ART has transformed HIV/AIDS into chronic but still manageable illness. Treatment for HIV with the use of ART presents challenges for patients and also for health-care providers on the aspects of adherence to the drug regimens. Non-adherence leads to decreased concentration of anti-retroviral agents in blood, which is not sufficient to suppress replication of viral particles and to decrease plasma viral load. In addition, poor adherence will also lead to development of drugresistant strains of HIV [11].
In a randomized clinical trial by Goujard et al. it was observed that knowledge among PLHIV regarding the HIV disease and its treatment can be increased by patient HIV-education programs. They also suggested that educational intervention given earlier in the course of treatment can prevent the development of drug resistance due to nonadherence [12].
Golin et al. conducted a two arm; randomized, controlled trial of a motivational interview (MI) based intervention to assess the impact of adherence to ART among PLHIV. The MI effectively improved multideterminant health-related complex behaviour and also enhanced ART adherence. The PLHIV in intervention group had improved their attitudes towards medication adherence and self-efficacy compared to control group [13].
In a study conducted by Christian Pradier et al. on evaluating the impact of intervention on ameliorating adherence to ART among PLHIV, it was observed that educational and counselling interventions were effective in increasing the adherence to ART and Quality of Life (QOL) along with their health status, suggesting that it could be easily implemented in resource limited clinical settings [14].
Efficacy of psycho-educational intervention by A. Tuldra et al. to improve long-term ART adherence, shows that psycho educative intervention group had high level of ART adherence during followup for 1 year in contrast with the control group. Additionally psycho education had led to better viral load suppression after 1 year because of the long term adherence maintenance. They also demonstrated a positive relationship between high adherence and decreased viral load. Study also suggested that evaluating specific variables for nonadherence to ART might be clinically useful to improve patients’ compliance [15].
Sound knowledge about the transmission of HIV is essential, but it’s not quite enough to maintain protective behaviour; however dearth of information regarding HIV/AIDS makes people more vulnerable. Findings from Bertoni et al. in their study to assess knowledge regarding HIV/AIDS and HIV transmission among drug users in Rio de Janeiro, Brazil were promising. Around 40% of them were drug users and never used condoms and also more than 60% of them reported that they were under the influence of substance and they have not used condoms. Almost 80.6% drug users responded that safer sex practice implies condom use; but still false beliefs exist and other perceptions to the mode of transmission were vague. Their study concluded that, high risk of HIV transmission existed among drug users compared to general population. Study also proposed that incorrect knowledge about HIV/ AIDS may be a barrier for HIV testing in-time and interventions should be planned to such category of people [16,17].
Amico et al. conducted a study to find the reason for nonadherence to ART among a sample of PLHIV in the South America. As almost perfect adherence for long duration is required for suppression of viral particles, and most of them are incapable to do so, this study sought to account for better understanding of barriers to adherence among PLHIV. The main reasons for non-adherence were (i) didn’t have the medication (ii) overslept through the dose (iii) dearth of HIV medication (iv) busy with other things (v) other reasons. This study recommended that interventions should be carried out according to individual’s needs and specific problems faced by PLHIV [18].
T. Parsons et al. assessed the effectiveness of behavioural interventions designed to increase ART adherence and to decrease consumption of alcohol among PLHIV. In this randomized controlled trial, motivational interviewing and cognitive behavioural skills building interventions were assigned randomly among PLHIV. Results showed that intervention group had shown decrease in viral load, increased CD4 cell count and improved adherence to HIV medication, but no significant effect on usage of alcohol. This study recommended adding booster sessions with behavioural intervention among PLHIV who are alcoholic and also suggested continuous counselling about ART adherence [19].
Nachega et al. in their review on ART adherence in low and middle income countries stated that adherence level was equal or more in low income countries compared to high income countries. However, interventions which are culturally sensitive should be carried out before and after initiation of ART, which is very important in low and middle income countries. Related studies also emphasize about further need of research to spot risk factors and build up adherence among adolescents, children and adults with communication to PLHIV who are at risk for non-adherence [20,21].
Proper knowledge regarding HIV disease, risks and benefits of the treatment and consequences of non-adherence to ART is important in HIV health care.
There is wide variation to the level of adherence and factors determining the adherence to ART based on cultural settings, resource availability and the literacy level of the PLHIV. In developing countries like India, HIV related knowledge among PLHIV is low and there is paucity of literature regarding the intervention strategies to improve adherence to ART through HIV education.
Results of the studies conducted outside India may not be relevant/ extrapolated to the Indian scenario, hence the intervention strategies should be contextualized according to the cultural settings before implementation.
To assess the effectiveness of educational intervention in improving adherence to ART among PLHIV attending ART centres of Kasturba Medical College Hospital (KMCH), Mangalore, South India.
To develop educational intervention module to improve adherence to ART among PLHIV
To study the effect of educational intervention in improving the level of adherence to ART
There will be a significant difference across the time (pre-test and post-test) and across the groups (Intervention and Control) with regards to:
• Level of adherence to ART among PLHIV
• Change in CD4 count
• HIV Knowledge among PLHIV
Background information of the study area
Mangalore is the administrative headquarters of the Dakshina Kannada district, and the fourth largest city in the state of Karnataka [22].
The prevalence of HIV has been showing a declining trend in Dakshina Kannada District during the past four years. However, the prevalence rate of 0.75% is still higher than the national prevalence of 0.27% and state prevalence of 0.69% [23].
Study settings
ART centre of Kasturba Medical College Hospital (KMCH), Attavar, Mangalore, India.
KMCH is a 650 bedded tertiary care teaching hospital. It has a government funded ART centre.
Study design
Study consists of two phases:
Phase I: A cross-sectional study (n=409) has been done to find out the level of adherence to:
(i)ART among PLHIV using pre-test tools: Adult AIDS Clinical Trials Group (AACTG) adherence follow-up questionnaire [24].
Adherence index was calculated by the formula:

PLHIV with ≥ 95% of adherence were considered as having high adherence and those with <95% were considered having low adherence to HIV medication.
(ii)HIV related knowledge among PLHIV was tested using HIV Knowledge Questionnaire (HIV-KQ-18 [25].
Pre-test findings: We observed that the prevalence of nonadherence to HIV medication was 27.1% (n=121).
HIV knowledge was high among 127 (31.1%) PLHIV and low among 282 (68.9%) PLHIV.
Among 121 PLHIV who were non-adherent, 110 PLHIV will be included in the 2nd phase of the study.
Phase II Randomized controlled trial: An open labelled, block randomized trial with outcome assessment blinded will be conducted.
Sample size
Based on adherence to ART among PLHIV from a previous study [5] and by comparison of two proportions (P1=94) and (P2=69), sample size is calculated using the formula:
Zα=1.96 (value at a specific confidence level 95%)
Zβ=1.28 (90% power)
P1=94% of the patients in the intervention group achieved adherence (>95%) to ART.
P2=69% of the patients in the control group achieved adherence (>95%) to ART.
Q1=(1-P1); Q2=(1-P2)
P=P1+P2/2; Q=Q1+Q2/2
Taking non-responders as 10%, sample size was found to be 55 PLHIV in each group.
Total=110 PLHIV
Study subjects
PLHIV who are receiving ART under ART center of KMCH, Attavar, Mangalore.
Inclusion criteria:
• All PLHIV aged 18 years or above and who are on ART
• PLHIV who consent to be a part of the study
Exclusion criteria:
• PLHIV aged below 18 years
• PLHIV with mental illness and unable to communicate
Study duration: 2 years (2015 to 2017) (Figure 1).
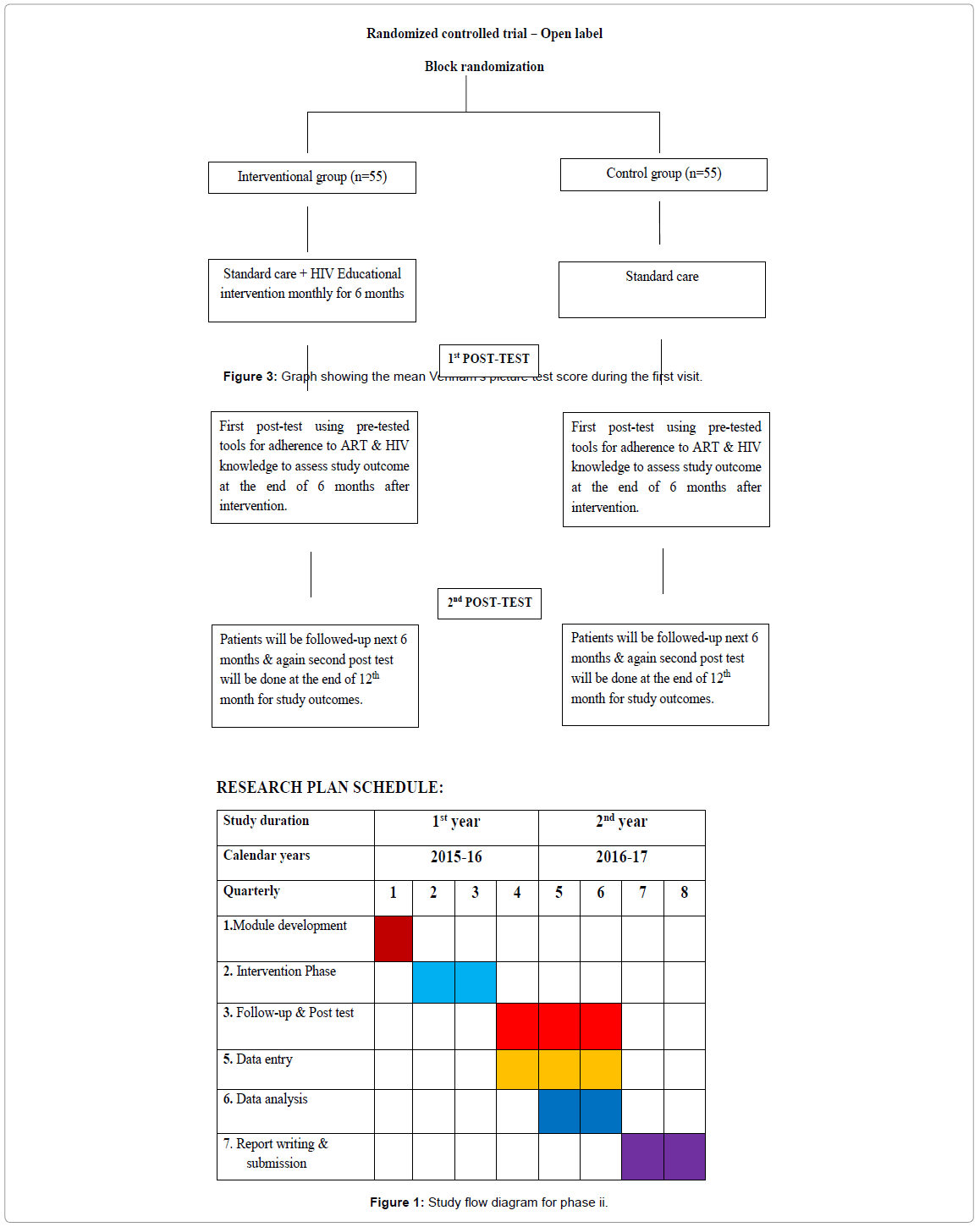
Figure 1: Study flow diagram for phase ii.
Randomization procedure
In randomized controlled trail (RCT), 110 PLHIV who are nonadherent to ART will be randomized into 2 groups (Intervention and Control group). Block randomization technique will be used by randomizing PLHIV into block of 4 and block of 6 in a randomly generated sequence so that equal number of patients will be allocated in the intervention and control groups. Unequal block sizes will be used to minimize selection bias.
To achieve sample size of 110 PLHIV, 11 blocks of size 6 and 11 blocks of size 4 will be required. The sequences for block 4 and 6 will be generated separately,
e.g.: (4,4,6,4,6,6,4,6,4,4,6,6….)
11 permutations each for block 4 and 6 will be generated randomly
| (ICIC/IICC/ICCI/CCII.....) | For block size of 4 |
| (IIICCC/CICIII/CCCICI….) | For block size of 6 |
Intervention procedure
HIV- education interventional modules will be developed based on:
a. Cross-sectional study findings
b. Inputs from Positive Prevention Program [26]
Educational modules will be implemented and contextualized according to the local settings in the local language. Content validity of the module will be tested before implementation of the modules in the study settings.
These educational modules will be developed to help health care providers and counsellors in delivering HIV related knowledge during their routine interactions with PLHIV
In our study, HIV educational intervention will consists of six modules:
• Basic information about HIV/AIDS
• How HIV attacks your health?
• Helping patients to prevent the spread of HIV through sexual contact
• Preventing the spread of HIV from mothers to infants
• Helping patients with improving adherence to their HIV medications
• Helping patients to protect their health and live healthier lives
• HIV educational intervention to PLHIV will be provided with the use of flip-charts, hand-outs, pictograms and computer based audio-visual interactive sessions from the educational modules.
Six sessions will be provided with duration of 1 hour for each session to the intervention group for 6 months (once in every month). The PLHIV missing one session will be contacted and requested to appear for the next session. Participants missing two or more sessions will be considered as drop outs.
The PLHIV participating in both the groups will receive standard patient care available in the respective ART centre.
Standard patient care components available in ART centres are:
PLHIV will be counselled before the initiation of ART through Integrated Counselling and Testing Centre (ICTC).
Once in a month patients will come to ART centre to collect drugs and patients’ adherence to ART will be checked and also patients who missed their dose will be counselled every month.
CD4 count will be checked once in every six months to check the improvement in the treatment provided.
After the six months intervention period, post-test will be done to assess the study out comes from both the groups.
First Post-test will be done at the end of 6 month (after intervention) and PLHIV will be followed-up for the next 6 months and again second post-test will be done to measure the study outcomes at the end of 12 months. Tools used for the pre-test will be re-used in post test to measure the study outcomes.
• To measure the effect of educational intervention on
• The level of adherence to ART among PLHIV
• Change in CD4 count among PLHIV
• Knowledge regarding HIV disease among PLHIV
Outcome assessment of the study will be blinded. Outcome measures will be done by assessor, who will not be involved in the study.
The collected data will be coded, entered and analyzed using SPSS Version 16.
For categorical variables (level of adherence to ART, knowledge of HIV): Chi-square test will be done. P-value <0.05 will be considered as statistically significant.
Logistic regression (binary and multivariate) will be done to assess the relationship between the study out outcomes and sociodemographic variables (age, sex, marital status etc) and clinical variables. The fit of the logistic model will be assessed with the Hosmer and Lemeshow goodness of fit test; P-value of <0.05 will be considered evidence of a statistically significant difference between predictive and outcome variables.
The study protocol has been approved by Institutional Ethics Committee (IEC) of Kasturba Medical College, Mangalore.
Research
It will provide further information to the current practice of HIV/ AIDS care in ART centres of Dakshina Kannada District. The data obtained may help for further studies in this area.
Quality and effectiveness
The study will help to determine the factors affecting the adherence of PLHIV to ART in this region and will provide strategies to improve the adherence among PLHIV and thus making existing HIV care more effective.
Policy making
The information generated will provide essential support for the planning policies in the future, which can be implemented across India.