Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Research Article - (2018) Volume 6, Issue 3
Background:Currently, the role of angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor antagonist (ARB) in CIN is paradoxical due to important differences in study design and study participant characteristics. We speculated that enalapril and folic acid tablets may have better protection on kidney target. Aim: To explore the impact of enalapril and folic acid tablet on contrast-induced nephropathy (CIN) in patients with mild renal insufficiency after percutaneous coronary intervention (PCI).
Method: A total of 816 patients undergoing selective PCI, between January 2013 and December 2016, were enrolled in a prospective cohort. Patients were divided into enalapril and folic acid tablets treatment group (n=233) (Namely, intervention group) and non ACEI/ARB treatment group (n=583) (Namely, control group). Baseline data were compared among 2 groups, and multivariate logistic regression analysis was used to analyze the independent risk factors for CIN. The clinical events within 1-month after contrast were recorded.
Result: The incidence of CIN was lower in the intervention group than in the control group (8.2% (19/233) vs. 13.4% (78/583), P=0.041). Multivariate analysis found that age odds ratio [ (OR)=1.078, P=0.001] and hypertension (OR=3.376, P=0.004), hyperhomocysteinemia (OR=3.339, P=0.001) were independent risk factors of CIN. However, eGFR was the dependent protector factor of CIN (OR=0.957, P=0.013). During 1 month follow-up, the rate of recurrent angina pectoris was lower in the intervention group than in the control group (PË0.05), however, there were no significant differences between the 2 groups in the rates of worsening renal failure or hospitalization for worsening renal failure, dialysis/hemofiltration, acute heart failure, myocardial infarction recurrence and all-cause death (all, PË0.05).
Conclusion: The treatment with enalapril and folic acid tablet may prevent the occurrence of CIN in patients with mild renal insufficiency after PCI.
Keywords: Enalapril and folic acid tablet; Homocysteine; Contrast-induced nephropathy; Percutaneous coronary intervention
Contrast nephropathy (CIN) is the third most common cause of hospital-acquired renal failure, accounting for 7% to 15% [1]. It not only leads to extension duration of hospitalization, but also accelerates the occurrence of end-stage renal diseases and seriously affects the clinical prognosis of patients with coronary artery disease (CAD) [2]. Therefore much more attention has been paid increasingly to reduce the incidence of CIN and which becomes the research focuses of prevention and treatment of perioperative complications after cardiovascular interventional therapy. It is known that renal dysfunction is the most important risk factor of CIN [3], chronic kidney disease (CKD) has a complicated interrelationship with various comorbidities, particularly with CAD [4] but the preventive measures are limited for CIN at present. Therefore, how to effectively reduce the risk of CIN in patients with CAD and renal insufficiency remains to be further studied. Currently, the role of angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor antagonist (ARB) in CIN is paradoxical due to important differences in study design and study participant characteristics [5-7].
Enalapril and folic acid tablets is a single tablet combination, containing 10 mg enalapril and 0.8 mg folic acid, in which folic acid is an important cofactor in the process of re-methylation of homocysteine (Hcy) to regenerate methionine. Increase of folate intake can improve endothelial function and delay the deterioration of renal function for playing a certain role of renal protection by reducing the level of Hcy [8]. We speculated that enalapril and folic acid tablets may have better protection on kidney target. Therefore, this study was to mainly evaluate the effect of Enalapril and folic acid tablets on the occurrence of CIN in patients with CAD and chronic mild renal insufficiency after percutaneous coronary intervention (PCI).
Study population
This prospective observational study was carried out on 816 patients with CAD undergoing elective PCI in the Department of Cardiology, Zhongda Hospital Affiliated to Southeast University from January 2013 and December 2016. All patients were divided into two groups by the application of enalapril and folic acid tablets group (N=233, EFa group) or non ACEI/ARB group (N=583, control group). Inclusion criteria: (1) Participants with an estimated glomerular filtration rate (eGFR) (60~89) mL/min/1.73 m2; (2) Without received any ACEI/ARB treatment at least 14 days; (3) Without taking folic acid or folic acidcontaining preparation, contraceptive, Vitamin B6 and B12, and other drugs affecting metabolism of Hcy in the past month. Exclusion criteria: (1) Allergy to iodine or iodine contrast agent; (2) Acute renal injury or with application of renal toxicity drugs in nearly two weeks; (3) Take CT, MRI and other examinations with contrast agents during the two weeks before study; Take radiographic examination of other contrast agents during the study period; (4) Acute ST-segment elevation myocardial infarction (STEMI), class IV heart failure as defined by the New York Heart Association (NYHA) functional classification system, hemodynamic instability, hepatic dysfunction (serum alanine-aminotransferase (ALT) concentration three times greater than the upper limit of normal) or thyroid insufficiency; (5) Patients with incomplete data collection, in particular, those lack of renal function evaluation indicators at 48 h to 72 h after PCI. Informed consent was obtained from all patients prior to data collection approval by the Zhongda Hospital of Southeast University ethics committee.
Study protocol
Renal function was measured using eGFR with the modified MDRD formula (eGFR=175 × creatinine−1.234 × age−0.179 × [0.79 (female)] according to data from Chinese patients with CKD. Hyperhomocysteinemia (H-Hcy) was defined as Hcy ≥ 10 μmol/L [9]. CIN is the renal dysfunction exclusion of those caused by other causes, creatinine increased 44.2 μmol/L or more, and higher 25% than the basic level at 48 h to 72 h after application of iodine contrast agent [10].
Patients were divided to treatment with enalapril maleate and folic acid tablets (AUSA Pharmed, Shenzhen), 1 single-pill tablet every day from 2 days before to 3 days after contrast medium administration (total dose of 50 mg enalapril and 4 mg folic acid over five days). However, patients assigned to the control group did not receive any ACEI/ARB and other ACEI/ARB included Perindopril, Valsartan, Losartan therapy was resumed in control group 3 days after contrast medium administration if needed.
Prespecified clinical and laboratory demographic information was obtained from hospital charts that were reviewed by independent research personnel unaware of the objectives of the study. Post procedure serum creatinine values were measured within 48 h or 72 h in all patients as possible. All patients underwent PCI by standard techniques. Patients were given 300 mg loading dose of aspirin, 300 mg loading dose of clopidogrel or 180 mg ticagrelor at PCI. Intravenous administration of isotonic saline (1.0-1.5 ml•kg-1•h-1) was given for hydration at 3 h to 12 h before operation and 6h to 24 h after operation. Physicians took rationally use of β-blockers, statins, nitrates, calcium antagonists, anti-platelet drugs, low molecular weight heparin and other drugs according to clinical conditions of patients.
Endpoints and definitions
Clinical follow-up was performed by either telephone contact or clinical visit at 1 month. The primary outcome was the development of CIN. The occurrence of clinical outcomes included events occurring within 30 days after contrast: 1) worsening renal failure, defined by change of CKD classification (class change ≥ 1) or hospitalization for worsening renal function; 2) dialysis or hemofiltration due to symptoms or signs of uremic syndrome or management of refractory hypervolemia, hyperkalemia or acidosis; 3) acute heart failure or worsening heart failure, defined as a deteriorated NYHA functional class (class change ≥ 1); 4) angina or myocardial infarction recurrence; 5) all-cause death.
Statistical analysis
Statistical analysis was performed using SPSS 17.0 software. Comparisons among normally distributed continuous variables, expressed as mean ± SD, were performed using Student t tests; nonnormally distributed continuous variables, presented as medians and interquartile ranges (P25 and P75), were analyzed using Wilcoxon rank-sum tests. The chi-square or Fisher exact test was used for categorical data, expressed as percentages. Multivariate predictors of CIN were identified by logistic regression analysis; results were tabulated as odds ratios (OR) with 95% confidence intervals (CI). All p values were 2-tailed, and statistical significance was defined by a p value <0.05.
Baseline and clinical characteristics
816 patients were enrolled in this study, aged 60 years to 88 years and with mean age of (68.7 ± 5.6) years. 518 patients were males (63.5%) and 298 were females (36.5%). Of the 816 patients, the mean levels of Hcy and creatinine were (12.3 ± 6.1) μmol/L and (89.1 ± 11.6) μmol/L, respectively.
The baseline characteristics and laboratory results are summarized in Tables 1 and 2. There were no significant differences in age, gender, atherosclerotic risk factors, prior MI, and prior coronary stenting among two groups, and evidence-based medications such as aspirin, beta-blocker and statins were similarly prescribed in two groups. Only the incidence of hyperlipidemia was obviously lower in EFa group than that in control group (P<0.05). The level of initial laboratory findings, including hemoglobin, total cholesterol, glucose, baseline serum creatinine and Hcy were also similar among two groups. However, the level of uric acid was obviously higher in EFa group than that in control group (P<0.05) but HDL-C level obviously lower in EFa group than that in control group (P<0.05).
| Variable | EFa group (N=233) | Control (N=583) |
P value |
|---|---|---|---|
| Age, years | 68.7 ± 5.4 | 68.6 ± 5.7 | 0.775 |
| Male, % (N) | 64.8 (151) | 63.0 (367) | 0.63 |
| Body mass index (kg/m2) | 25.1 ± 2.8 | 24.9 ± 2.8 | 0.558 |
| SBP (mmHg) | 139 ± 19 | 136 ± 21 | 0.078 |
| Smoking, % (N) | 29.2 (66) | 34.9 (198) | 0.134 |
| Hypertension, % (N) | 74.0 (171) | 71.6 (410) | 0.344 |
| Hypercholesterolemia,% (N) | 28.8 (53) | 45.2 (239) | 0.001 |
| Diabetes, % (N) | 19.3 (44) | 20.4 (118) | 0.77 |
| Prior MI,% (N) | 7.3 (17) | 8.4 (49) | 0.6 |
| Prior coronary stenting, % (N) | 14.2 (33) | 17.2 (100) | 0.296 |
| Medications, % (N) | |||
| Aspirin | 91.4 (213) | 93.2 (543) | 0.394 |
| Beta blockers | 67.4 (157) | 64.8 (378) | 0.49 |
| statins | 93.6 (218) | 92.5 (539) | 0.58 |
Note: Continuous variables are expressed as mean ± standard deviation. Categorical variables are presented as percentage.
SBP: Systolic Blood Pressure. MI: Myocardial Infarction.
Table 1: Baseline characteristics of the patients.
| Variable | EF group (N=233) | Control (N=583) | P value |
|---|---|---|---|
| Hemoglobin, g/L | 131 ± 16 | 134 ± 16 | 0.096 |
| Total cholesterol, mmol/L | 4.63 ± 1.1 | 4.80 ± 1.1 | 0.051 |
| Triglyceride, mmol/L | 1.76 ± 1.1 | 1.64 ± 1.0 | 0.124 |
| LDL-C, mmol/L | 2.78 ± 0.81 | 2.91 ± 0.89 | 0.054 |
| HDL-C, mmol/L | 1.33 ± 0.52 | 1.22 ± 0.40 | 0.001 |
| Fasting glucose, mmol/L | 5.67 ± 1.6 | 5.68 ± 1.7 | 0.894 |
| Hs-CRP, ug/L | 15.2 (8.2, 36.0) | 11.8 (2.6, 64.2) | 0.462 |
| Uric acid, umol/L | 403 ± 94 | 356 ± 86 | 0.001 |
| Cystatin C, mg/L | 1.36 ± 0.81 | 1.27 ± 0.62 | 0.218 |
| Creatinine, umol/L | 89.7 ± 11.8 | 88.9 ± 11.4 | 0.384 |
| eGFR, mL/min | 75.5 ± 8.3 | 76.0 ± 8.3 | 0.464 |
| Hcy, mmol/L | 12.1 ± 6.9 | 12.3 ± 5.8 | 0.686 |
| H-Hcy, % | 72 | 72.8 | 0.851 |
Data are presented as mean ± standard deviation for continuous variables, number (%) for categorical variables. HDL–C: High-Density Lipoprotein–Cholesterol; LDL–C: Low-Density Lipoprotein–Cholesterol; Hs-CRP: Hypersensitive C-Reactive Protein; Hcy: Homocysteine; H-Hcy: Hyper-Homocysteinemia.
Table 2: Laboratory characteristics.
Coronary angiographic and procedural characteristics
The coronary angiographic and procedural characteristics were shown in Table 3. There were no significant differences in the coronary angiographic characteristics. All patients received PCI with coronary stenting. Number of stent, multi-stenting and used CM volume and hydration were not different among the two groups.
| Variable | EF group (N=233) | Control (N=583) | P |
|---|---|---|---|
| Contrast volume(mL,25%,75%) | 80 (60,140) | 80 (70,140) | 0.396 |
| No. vessel disease, % (N) | 0.392 | ||
| Vessel disease | 42.5 (99) | 39.6 (231) | - |
| Vessel disease | 28.3 (66) | 30.0 (169) | - |
| Vessel disease | 29.2 (68) | 31.4 (183) | - |
| No. vessel disease, x ± s | 1.5 ± 1.1 | 1.6 ± 1.0 | 0.142 |
| Multivessel disease,% (N) | 57.5 (134) | 60.4 (352) | 0.451 |
| Stents, N | 1.7 ± 0.8 | 1.8 ± 0.6 | 0.218 |
| Multi-stenting,% (N) | 62.6 (146) | 68.4 (399) | 0.113 |
| Hydration,% (N) | 55.8 (130) | 52.7 (307) | 0.417 |
Table 3: Coronary angiographic and procedural characteristics.
Primary study outcome
Overall, CIN occurred in 97 of 816 patients, accounting for 11.9%. The incidence of CIN was significantly higher in the control group (78 of 583, 13.4%) than in the EFa group (19 of 233, 8.2%; P=0.041). And the incidence of CIN in H-Hcy group was significantly higher than that in normal group (14.3% (79/554) vs. 6.7% (14/209), P=0.004). The incidence rates of CIN were 3.8% and 13.6% in hypertension patients and controls, respectively (14.3% (83/581) vs. 6.1% (14/231), P=0.001). While the incidence of CIN was also higher in the diabetes group compared to the control group (17.3% (28/162) vs. 6.1% (69 /645), P=0.030) (Figure 1).
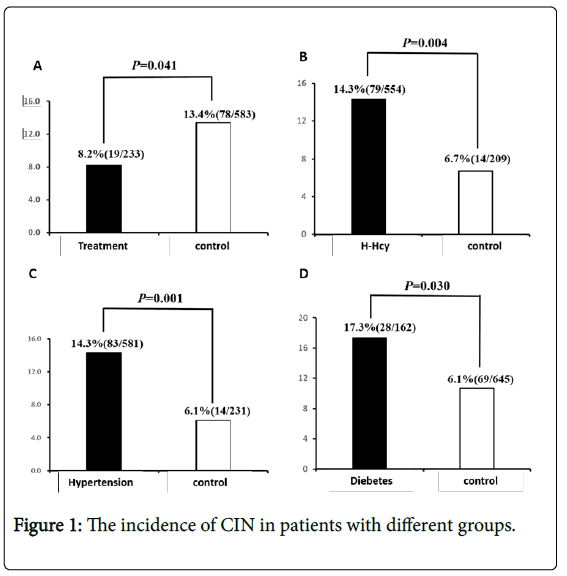
Figure 1: The incidence of CIN in patients with different groups.
Multivariate logistic regression analysis for the development of CIN
Multivariate analysis was conducted by using variables which was modest significant (p<0.05) in the univariate logistic regression analysis, we found that the independent predictors for CIN occurrence were age (OR=1.078, 95% CI: 1.031-1.127, P=0.001), hypertension (OR=3.376, 95% CI: 1.540-9.096, P=0.004) and H-Hcy (OR=3.339, 95% CI: 1.674-6.660, P=0.001). While eGFR was the protective factor of CIN (OR=0.957, 95% CI: 0.923-0.991, P=0.013) (Table 4).
| Factors | Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | |||
| Lower | Upper | Lower | Upper | |||||
| H-Hcy | 2.317 | 1.281 | 4.189 | 0.005 | 3.339 | 1.674 | 6.66 | 0.001 |
| Age | 1.088 | 1.049 | 1.128 | 0.001 | 1.078 | 1.031 | 1.127 | 0.001 |
| Hypertension | 2.583 | 1.434 | 4.652 | 0.002 | 3.376 | 1.54 | 9.06 | 0.004 |
| Diabetes | 1.744 | 1.082 | 2.813 | 0.022 | 1.761 | 0.96 | 3.232 | 0.068 |
| eGFR | 0.947 | 0.922 | 0.972 | 0.001 | 0.957 | 0.923 | 0.991 | 0.013 |
| EFa treatment | 0.575 | 0.34 | 0.973 | 0.039 | 0.863 | 0.814 | 0.981 | 0.049 |
| Male | 1.132 | 0.724 | 1.769 | 0.586 | ||||
| Smoking | 0.646 | 0.397 | 1.054 | 0.08 | ||||
| Hypercholester-olemia | 1.416 | 0.914 | 2.192 | 0.119 | ||||
| Prior MI | 1.566 | 0.441 | 5.557 | 0.488 | ||||
| Prior coronary stenting | 3 | 0.759 | 11.86 | 0.117 | ||||
| Total cholesterol | 0.948 | 0.777 | 1.158 | 0.602 | ||||
| Fasting glucose | 1.008 | 0.885 | 1.147 | 0.908 | ||||
| HDL-C | 0.588 | 0.328 | 1.056 | 0.076 | ||||
| LDL-C | 0.921 | 0.715 | 1.186 | 0.524 | ||||
OR: Odds Ratio; CI: Confidence Interval; H-Hcy: Hyper-homocysteinemia; eGFR: estimated Glomerular Filtration Rate; EFa: Enalapril and Folic acid. MI: Myocardial Infarction. HDL-C: Highdensity Lipoprotein-Cholesterol. LDL-C: Low-Density Lipoprotein-Cholesterol.
Table 4: Independent predictors for CIN occurrence.
Subgroup analysis
The benefit of enalapril and folic acid therapy was consistently effective among various subgroups (Figure 2). Patients at age ≥ 65 years (OR=0.357, 95% CI: 0.189-0.676) and with hypertension (OR=0.528, 95% CI: 0.297-0.941) showed a similar trend toward receiving benefit from enalapril and folic acid against the occurrence of CIN.
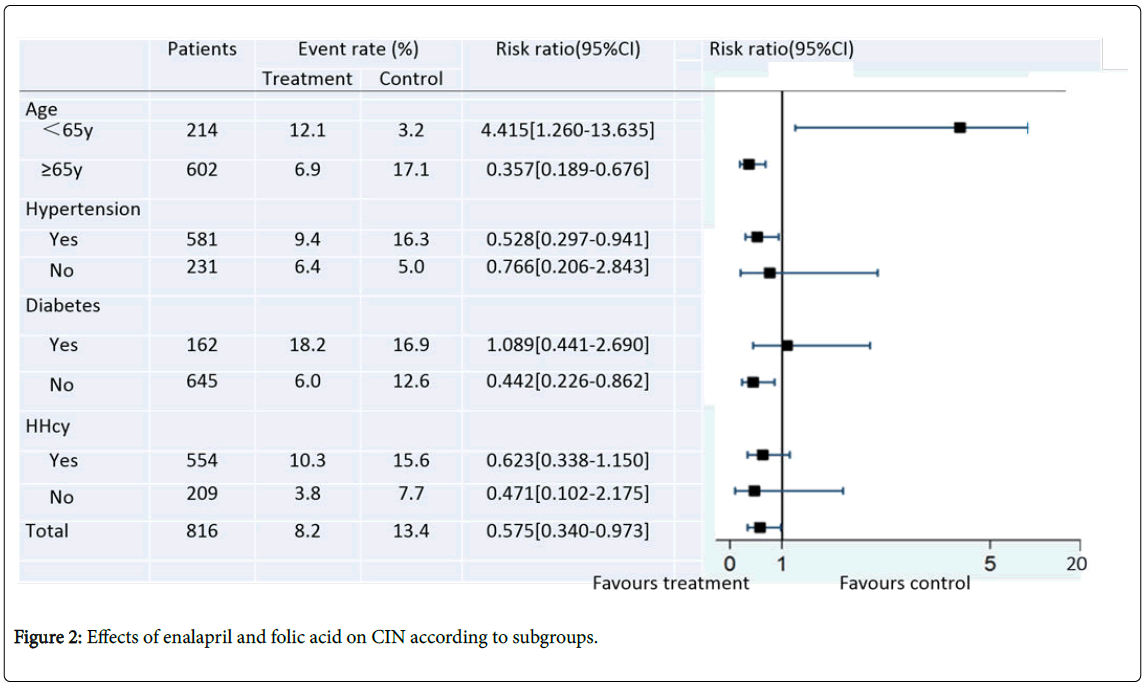
Figure 2: Effects of enalapril and folic acid on CIN according to subgroups.
The occurrence of clinical outcomes
Clinical follow-up rate was up to 96.4% for patients in two groups at 1 month after discharge. The recurrence rate of angina was obviously lower in EFa group than that in control group at 1 month after discharge (P<0.05), while there were no significant differences in the incidences of worsening renal failure (change of CKD grade ≥ 1) or hospitalization for worsening renal failure, dialysis/hemofiltration, acute heart failure, myocardial infarction recurrence and all-cause death among two groups (Table 5).
| Events | EF group(N=223) | control(N=564) | P |
|---|---|---|---|
| Worsening renal failure* | 5.4 (12) | 6.9 (39) | 0.431 |
| Hospitalization for worsening renal function | 1.9 (4) | 2.7 (16) | 0.476 |
| Dialysis/hemofiltration | 0 | 0.2 (1) | 0.529 |
| Acute heart failure | 0.4 (1) | 0.5 (3) | 0.882 |
| Angina recurrence | 4.9 (11) | 9.2 (52) | 0.046 |
| Myocardial infarction recurrence | 0.9 (2) | 0.9 (5) | 0.989 |
| All-cause deaths | 0.4 (1) | 0.7 (4) | 0.678 |
*Defined by change of CKD classification (class change ≥ 1).
Table 5: The occurrence of clinical outcomes.
CIN is a common but underdiagnosed complication of PCI and is associated with prolonged hospitalization and high mortality with CAD. It is currently without special effective treatment of CIN and can only do early identification of risk factors for prevention, to avoid the occurrence of CIN. Several risk factors have been proposed to be associated with CIN, including previous renal insufficiency, diabetes mellitus, age >75 years, hypertension, congestive heart failure, contrast medium osmolality, volume and nephrotoxic drugs [11,12]. In recent years, some studies [13,14] have shown that elevated Hcy is independently associated with the risk of CIN among patients with impaired renal function undergoing coronary angiography and/or angioplasty. The results of our study demonstrate that enalapril and folic acid tablets resulted in a significant reduction in CIN for patients with CAD and mild renal dysfunction. This low cost intervention could be considered when referring a patient for cardiac catheterization. The clinical relevance of these findings needs to be confirmed in a larger clinical trial.
ACEI/ARB during cardiac catheterization may prevent medullary ischemia induced by angiotensin II after contrast administration. Theoretically, ACEI can protect against CIN by blocking contrast agent-induced contraction of inferent arterioles. Alternatively, ACEI or ARB can aggravate the decline in GFR in the acute phase of renal blood flow induced by contrast agent and predisposition toward CIN. Due to the various mechanisms described above, prior studies have reported conflicting results regarding the risk/benefit of ACEI/ARBs to increase the occurrence of contrast agent-induced nephropathy.
Results of some randomized controlled trials indicate that ACEI or ARB is a protective factor for CIN and there is no heterogeneity. The earliest study conducted by Gupta et al. [15] was a randomized controlled trial, which compared the incidence of CIN between patients taken Captopril and those without Captopril at 3 days before surgery and the results indicated that Captopril had protective effect against CIN. In contrast, most of the enrolled observational studies indicated that ACEI can increase the risk of CIN. The study conducted by Rim et al. [16] was a retrospective trial with largest sample size, it took tendency of score to correct the confounding factors and the matching results suggested that ACEI or ARB may increase the incidence of CIN. Koza et al. [17] compared the effect of long-term use of ACEI /ARB on CIN, which showed that the incidence of CIN was significantly higher in ACEI/ARB group than that in non-ACEI/ARB group. Wu et al. [6] meta-analysis included large scale studies published recently (7288 patients received ACEI/ARB while 8,159 patients received placebo or were naive to ACEI/ARB), serving to potentially challenge some of the concerns that the administration of RAAS blockers protects against the development of CIN. The magnitude of association was significantly reinforced in the observational studies (OR=1.84, 95% CI: 1.19-2.85, P=0.006) but not in the randomized controlled trials (OR=0.88, 95% CI: 0.41-1.90 P=0.74). They found that the effect of RAAS blockers appears heterogeneous and relatively modest with uncertain clinical effects. The varies of study population, study methods, interventions and CIN definition can cause the differences of these studies and factors influencing the effect of ACEI/ARB on CIN include baseline serum creatinine, age, comorbidities, drug dose, drug type and dose of contrast agents. On the other hand, it may also come from the differences of above mentioned pathophysiological mechanisms of the disease itself. We note that these studies only focus on the occurrence of CIN but not explore the results of hard end points, such as renal replacement therapy, death, end-stage renal disease and the impact of hard end points should be the focused point by clinicians. In summary, although observational studies suggest that ACEI/ARB increase the risk of developing CIN, there is significant heterogeneity, and corrected risk factors are inconsistent in different studies. On the contrary, although the randomized controlled trials are with small sample size, heterogeneity is low; the difference between groups can be reduced by random allocation that the study results are relatively reliable. Therefore, ACEI/ARB may not increase the occurrence of CIN.
Hcy is a sulphur-containing amino acid, which is a metabolic product of methionine cycle, and is an important intermediate of many methylation reactions and energy metabolism. Hcy and its metabolite, S-adenosy L-homocysteine, are uremic toxins that accumulate in the plasma of patients with CKD because of impaired extrarenal metabolism [18,19]. Renal function damage can decrease metabolism and excretion of Hcy in plasma. Due to hypofunction of renal filtration and secretion, renal function damage can cause increase of blood Hcy and which induces atherosclerosis and vascular damage, mediated by endothelial dysfunction, decreased bioavailability of nitric oxide and generation of free radicals and oxidative stress. H-Hcy has been established as an independent risk factor for CAD and a cause of cardiovascular events in CKD and can be used as a biomarker to predict the prognosis of CAD outcome in CKD [20,21]. Recently, the authors and other studies[13,14] found that preoperative Hcy levels are independent risk factors for CIN; our previous study [22] also found that Hcy more than 10 μmol/L can significantly increase the incidence of CIN after PCI in ACS patients. Folic acid is considered to be the most common agent for Hcy-lowering therapy. However, Hcylowering therapy was initially reported not beneficial to general vascular outcomes in secondary prevention trials [23,24] but were reported later to have significantly reduced stroke recurrence and death in the post hoc analysis of the same trails [25]. The causative effect of H-Hcy on CAD is supported by several important trails including a large primary prevention trial, CSPPT (China Stroke Primary Prevention Trial) [26].
Enalapril and folic acid tablets are a new compound preparation of Class I with indications for the treatment of elevated Hcy. It has been approved and marketed by SFDA in 2008 and are particularly suitable for the treatment of primary hypertension concurrent with H-Hcy [26]. Both enalapril and folic acid are mainly excreted by the kidneys and with same absorption pathways, absorption rate and excretion pathways. Enalapril and folic acid is without new toxic effect or cannot cause increase of compared with enalapril. Therefore, we speculated that compound formulation of Enalapril and folic acid may have better target protection on renal organs, playing a 1+1>2 effect. Xu et al. [8] randomly divided patients with mild to moderate chronic renal insufficiency into combination of enalapril and folic acid supplementation group and simple enalapril group, with average treatment duration of 4.4 years. The results showed that folic acid supplementation significantly reduced the rate of renal dysfunction in hypertensive patients and reduced the risk of developing renal disease by 21% compared with single enalapril therapy.
But so far, there is no any literature to study whether Enalapril and folic acid tablets could prevent the occurrence of CIN. This is the first study to take analysis on 816 patients with CAD concurrent with mild renal dysfunction. Although it is an observational cohort study, the two groups of patients are with matched basic clinical baseline data, so the conclusion has some clinical value. We found that Enalapril and folic acid tablets can obviously reduce the occurrence of CIN (OR=0.575, 95% CI: 0.340-0.9973, P=0.041) and age (OR=1.078, 95% CI: 1.031-1.127, P=0.001), hypertension (OR=3.376, 95% CI: 1.540-9.096, P=0.004) and high Hcy (OR=3.339, 95% CI: 1.674-6.660, P=0.001) were risk factors of CIN after surgery; further subgroup analysis found that Enalapril and folic acid tablets was more effective in patients older than 65 years and having hypertension. Finally, a onemonth clinical follow-up showed that Enalapril and folic acid tablets was effective in reducing recurrence of angina and not increasing the deterioration of renal function, re-hospitalization, dialysis or blood filtration caused by deterioration of renal function, new myocardial infarction and all-cause death and other events.
The shortcomings of this study are the data from a single center and relatively general sample size. Statistical differences are found in clinical baseline index, laboratory index and other indicators between the two groups and multi-factor regression analysis is difficult to completely control the differences in baseline characteristics between groups; moreover, due to the inherent defect of observational study, the study has inevitable selection bias; it only records preoperative Hcy level, and the postoperative Hcy level is not recorded or evaluated. The assessment of renal function after PCI only relies on changes of creatinine levels within 72 h after surgery, and it is lack of long-term monitoring of renal function in patients. Although, the result showed negative relation of Enalapril and folic acid tablets with CIN, large clinical trials incorporating the evaluation of clinically patient-centered outcomes with different potential risks of CIN are needed to confirm the robustness of our results and to better determine the clinical utility of enalapril and folic acid supplementation strategy for the CIN prevention.
Preprocedural H-Hcy was independent factors for CIN in mild renal insufficiency patients undergoing elective cardiac catheterization. Hcy levels may be potential biochemical parameters for screening high-risk patients and the treatment with enalapril and folic acid tablet may prevent the occurrence of CIN.
This work was supported by grants to GLY from the Natural Science Foundation of China (research Grant #81600227). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
GY, CT and GM conceived and designed the experiments; JH, XP and ZC performed the experiments; GY, CY and QZ analyzed the data; GY, QZ and CT contributed reagents/materials/analysis tools; GY, CT and GM wrote the paper; GM contributed to revising manuscript critically for important intellectual content; GY, XP and ZC contributed to acquisition of data.