Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Research Article - (2013) Volume 1, Issue 2
Background: Preterm infants are at high risk for late-onset infections due to gram-negative or fungal organisms. Evidence supports that a common source for these organisms may be the gastrointestinal tract. One theoretical way to change the infection rate is to alter the bacterial flora inhabiting the newborn gastrointestinal tract using probiotics. This study examines the impact of routine use of a probiotic, Lactobacillus reuteri DSM 17938 (BioGaia®), on the rate of late-onset gram-negative and fungal infection in neonates with birth weight ≤ 1000 grams.
Methods: This is a retrospective cohort study comparing the rates of gram-negative bacterial and fungal infections in neonates with birth weight ≤ 1000 grams. The groups are separated into those neonates born from January 2004 to June 30, 2009, before introduction of L. reuteri, and neonates born July 2009 through July 2012 who received routine L. reuteri prophylaxis. Neonates were excluded if they died or were transferred within the fi rst week of life. The remainder were included in the study and recorded as either having late onset infection related to gram negative organisms or fungi, or not having late onset infection. Since no major changes occurred in our NICU practice in recent years, and the introduction of L. reuteri as routine prophylaxis was abrupt, we attributed the post-probiotic changes to the introduction of this new therapy. Rates of infection were compared using Chi square analysis with Fisher exact t-test.
Results: Medical records for 354 neonates were reviewed, 232 before- and 122 after-introduction of L. reuteri prophylaxis. Despite a marked reduction in necrotizing enterocolitis and mortality, the incidence of late-onset infection varied from year-to-year, but was not signifi cantly altered by the introduction of routine L. reuteri. No adverse events related to use of L. reuteri were noted.
Conclusions: Prophylactic initiation of L. reuteri as a probiotic does not decrease late-onset infection.
Keywords: Late-onset infection; Lactobacillus reuteri DSM 17938; Probiotic; Extremely low birth weight
Use of probiotics in the Neonatal Intensive Care Unit (NICU) has been associated with multiple benefits including decreased mortality and decreased severity and/or incidence of necrotizing enterocolitis (NEC) [1-5]. Additionally, some studies suggest a reduction in sepsis involving gram-negative organisms and fungi occurring aft er the third day of life [5-7]. Most analyses have provided support for the value of these products in preventing NEC and death [8-10]. Many studies have failed to show a benefi t in sepsis prevention, although some trend in favor of a preventive benefit [10,11]. Questions remain about which bacterial strain(s) would be most benefi cial. Several strains have worked for NEC prevention, but signifi cant infection prevention has mainly been reported by the same group of authors using bovine lactoferrin [5-7]. Because diff erent studies have used diff erent probiotic organisms and somewhat different methodologies and analyses, some authors have concluded that evidence is weak for the probiotic benefi ts reported in these individual studies [12]. With this in mind, additional studies are needed to clarify various possible benefits of probiotics.
We have recently studied the benefi ts of routine administration of probiotic with the product Lactobacillus reuteri DSM 17938 (L. reuteri), available under the brand name BioGaia® (BioGaia, Sweden). Our results showed a marked reduction in NEC rates for this population [13], resulting in a signifi cant healthcare cost savings for patients and our institution [14]. Further reference to Lactobacillus reuteri in this paper specifi cally refers to this specifi c strain of L. reuteri DSM 17938. Th is probiotic was initially selected because of relative ease of administration through nasogastric tubes without clogging the tube, compared to other products during our own in vitro experiments. In this sequential analysis, our focus is to further examine the potential benefi ts of L. reuteri in neonates born ≤ 1,000 grams, the possible reduction of late-onset sepsis with gram-negative bacteria and fungi.
Data collection
Th is study represents a retrospective chart review comparing the rates of late-onset infection in neonates before introduction of L. reuteri (January 2004-June 2009), with routine use of L. reuteri in neonates ≤ 1,000 gram birth weight (July 2009-June 2012). The use of L. reuteri as a standard medicine in the
Neonates were only excluded from the analysis if they died within the first week of life, as it was determined that these patients would not have had the opportunity to benefit from probiotic intervention. Data collected for this study included: gender, gestational age (determined by Ballard), birth weight, 5-minute Apgar score, growth restriction, any antenatal corticosteroid administration, method of delivery, maternal diagnosis of preeclampsia or chorioamnionitis and diagnosis of NEC or late-onset (after 7 days postnatal age) gram-negative bacteria or fungal infection. Neonates with a clinical diagnosis of sepsis, but who were culture negative were not counted as positive for late-onset sepsis due to gram-negative or fungal infection. Our laboratory standard of practice was to allow 5-7 days of growth for all cultures before identifying them as negative. Although the actual rates of breast feeding could not be reliably collected, our sense was that breastfeeding practices were not significantly different during the period studied in this analysis.
Starting in July, 2009, L. reuteri 17938, available under the trade name BioGaia® (BioGaia Inc., Lund, Sweden) was administered to preterm neonates and generally continued to hospital discharge. According to the manufacturer of BioGaia®, the recommended daily dose for term neonates is five drops (approximately 0.18 mL given the oil-based nature of the product drops). Five drops administers 100 million live active L. reuteri cells. In our preterm neonates, we opted to administer 0.1 mL as our standard dose, which would administer 556 million CFU. BioGaia® doses were prepared in the pharmacy under sterile conditions and refrigerated until administration the same day. Administration was required within six hours of removal from the refrigerator, per manufacturer recommendation.
We selected BioGaia® as our probiotic because the manufacturer has demonstrated careful quality control of the probiotic colonies delivered with their product. Additionally, other products examined in vitro, routinely clogged the orogastric tubes used in our neonates. L reuteri was continued until discharge in our patients. This typically meant at 3 months or more of treatment. It was stopped at discharge in all patients.
Statistics
Statistical approaches used to examine this data include unpaired t-test to examine differences in the demographic data collected before and after institution of BioGaia®. Statistically significant differences required pL. reuteri upon initiation of feedings (July 2009-June 2012), utilized chi square analysis with Fisher exact t-test. Data is presented in yearly epochs to demonstrate the variability of late-onset sepsis in this population. Because the numbers of events are too small in yearly epochs to detect even large effects, no statistical analysis is applied to these data. Since our primary endpoint in this study was reduction of NEC, we targeted a minimum of 80 neonates in the pre- and post- Lactobacillus reuteri for a pL. reuteri prophylaxis, and a known late-onset gram-negative bacteria or fungal infection event rate of 31%, this study is only powered to detect a decrease to a 20% late-onset infection rate.
Patient demographics for included neonates born ≤ 1,000 grams are similar, as previously described [13], with gestational ages averaging 26 weeks in both groups, and birth weight averaging 754 grams versus 743 grams for controls and treatment groups respectively. The only differences are the rates of chorioamnionitis (higher in controls, 53% versus 36%) and small for gestational age patients (lower in controls, 26% versus 44%). These were not shown to statistically affect other outcomes in our study. NEC rates, the focus of our previous study [13,14], are reduced from 15.1% in controls to 1.6% with L. reuteri prophylaxis.
The incidence of late-onset gram-negative bacteria or fungal infection before- and after starting routine prophylactic L. reuteri, is summarized in Figure 1. Comparison of events for the combined years before introduction of L. reuteri (January 2004-June 2009), with the years of L. reuteri prophylaxis (July 2009-July 2012), showed no significant reduction in rates of infection (31% versus 26.2%, p=0.309) after routine L. reuteri prophylaxis was started. The rates for gram-negative and fungus late-onset infection for each epoch is shown in Figure 2. Rates vary from 9%-43% before L. reuteri prophylaxis, to 20%-35% after routine prophylaxis. No adverse events or infections related to L. reuteri administration were noted in any of the infants included in the analysis.
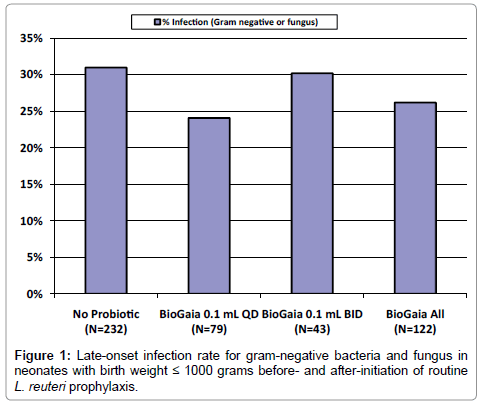
Figure 1: Late-onset infection rate for gram-negative bacteria and fungus in neonates with birth weight ≤ 1000 grams before- and after-initiation of routine L. reuteri prophylaxis.
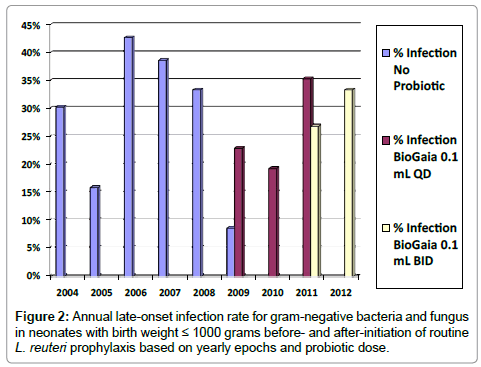
Figure 2: Annual late-onset infection rate for gram-negative bacteria and fungus in neonates with birth weight ≤ 1000 grams before- and after-initiation of routine L. reuteri prophylaxis based on yearly epochs and probiotic dose.
Probiotics have been shown to be a barrier to bacterial translocation and competitively exclude potential pathogens. Given these properties, one would conclude that probiotics should also play a role in reducing rates of infection. However, this has not been demonstrated in a controlled setting. Consistent with some published literature [3,4,9-11] we did not fi nd a signifi cant reduction in incidence of culture-positive late-onset bacterial or fungal infection (31 versus 26.2%). At the current doses which are very eff ective against NEC, a reduction in infection rates was not seen, but higher doses could off er this benefi t, possibly with a greater risk of causing infection from the probiotic itself. Perhaps, as other authors have suggested, we have yet to understand the optimal probiotic product, dose and duration to reach this infection prevention threshold, or are not using the ideal organisms.
We chose to dose our preterm neonates daily with 0.1 mL of L. reuteri. Th is dose was a conservative reduction of what the manufacturer recommends for term infants. Aft er two years of using this product, we wanted to confi rm that the product was colonizing the infant gut in eff ective amounts. In 2011, we collected stool samples at random from 7 infants who had been receiving L. reuteri for varying lengths of time (121-101 days) and found that, while all 7 had some level of fecal colonization, 3 of the 7 infants did not have optimum fecal colonization (106 to 107 L. reuteri CFU/g stool). As a result, our NICU decided to increase our standard prophylaxis dose from 0.1 mL to 0.2 mL daily in order to more accurately administer the recommended 100 million live, active L. reuteri cells.
While the benefi ts seen with probiotics to prevent NEC have been quite impressive [1-13] and cost-effective [14], the impact on late- onset infection has been more diffi cult to identify. Th e most impressive results are seen in earlier studies with bovine lactoferrin, which in animal models is enhanced by Lactobacillus GG. In studies of bovine lactoferrin alone or in combination with Lactobacillus GG, the greatest eff ects were observed for neonates below 1000 grams [5-7]. Based on the total group of patients in our study, the absolute reduction by 5% for late-onset infection, is insignifi cant, although a potential Number Needed to Treat (NNT) to prevent one case could be as low as 20 (Figure 1). Th us our study may simply be under-powered to detect a clinically important diff erence. A recent study by Garland et al. [15] proposes to correct this shortcoming.
Against the argument for missing any likely benefi t in our study, is the wide year-to-year fl uctuation of the rates of late-onset gram- negative and fungal infection (Figure 2), suggesting other variables play a more important role than probiotics. It may be that other probiotics or probiotic combinations off er more protection against late-onset infections. Also, giving a larger probiotic dose, 0.2 mL per day, did not lower the infection rate below that seen with the 0.1 mL per day dose, suggesting no additional benefi t is likely at the higher doses. Because this study represents newborns at the highest risk for infection and NEC, i.e. those below 1000 gram birth weight, the potential benefi ts would be expected to be greatest. Such benefi ts might not be measurable in neonates >1000 grams whose sepsis risk is lower. Th is was also observed in studies noting benefi ts with bovine lactoferrin alone or combined bovine lactoferrin and Lactobacillus GG [6], although the Lactobacillus GG added little benefi t beyond that seen with bovine lactoferrin alone. Furthermore, benefi ts from L. reuteri for prevention of nosocomial are expected since reutericyclin, an antibiotic peptide produced by this organism, competes with pathogens for adhesion to gut cells [16]. Our failure to fi nd a protective eff ect against late-onset infection by routine L. reuteri use should not diminish from the dramatic benefi ts from reduced NEC in preterm infants with L reuteri as well as other probiotics. It is also not the fi nal word on this subject, just a caution that it is premature to consider this use of probiotics without further research.
Our study has several limitations that arise from the limited power and the use of a secondary analysis of a study focused on a diff erent primary endpoint, NEC [13]. However, it is widely recognized that the greatest benefits for interventions with probiotics, are likely to be seen in neonates born 1000 grams or below [3,4,6,13,15]. Th us our study is unique in its focus on this population, and the data generated for dif erent endpoints. Our results support that, while probiotics can profoundly decrease the rate of NEC in ELBW infants [13,14], it may be unrealistic to expect probiotics to reduce late-onset infection rates, and they are unlikely to be confounders in studies of other interventions designed to reduce infection rates.
Prophylactic initiation of Lactobacillus reuteri as a probiotic for prevention of NEC resulted in statistically signifi cant reduction in NEC, but did not signifi cantly reduce rates of late-onset infection. Further research is needed to clarify any role probiotics might have in late-onset infection.
We wish to recognize the effort of several pharmacists and NICU nurses in performing the in vitro experiment to determine the best probiotic to select for our NICU, based on reliability of product delivery through the orogastric tube with various milk formulations. Our selection of BioGaia® as the probiotic of choice for the NICU was a direct result of this project. This project was in part supported by BioGaia Inc.