Endocrinology & Metabolic Syndrome
Open Access
ISSN: 2161-1017
ISSN: 2161-1017
Research Article - (2018) Volume 7, Issue 1
Aim: To determine the efficacy of maximum and optimum dosages of hydroxychloroquine (400 and 200 mg once daily) treatment combined with insulin along with metformin and Glimepiride in Type 2 diabetes patients who are poorly controlled and relationship to be evaluate between high-sensitive C-reactive protein (hs-CRP) and glycosylated haemoglobin (HbA1c) levels in such patients.
Methods: In a multicentre,open-labelled comparative observational study, randomised 240 patients [mean age 56.44 years and mean body mass index (BMI) 33.20 kg/m2, mean glycosylated haemoglobin (HbA1C) 8.58% ; mean duration of diabetes 13.7 years] with type 2 diabetes who were poorly controlled with a high stable insulin dose (≥ 30 Units/day for ≥ 30 days), glimepiride (2 mg/day) and metformin (1000 mg/day) were randomly allocated to either hydroxychloroquine 200 or 400 mg once daily for 6 months (24 weeks).
Results: At completion of 6 months (24 weeks), statistically significant, dose-dependent mean decreases from baseline were seen in both the hydroxychloroquine 200 and 400 mg groups for HbA1C (-0. and -1.3%, respectively) (p<0.0001), fasting plasma glucose (FPG) (-29.5 mg/dl and -33.2 mg/dl, respectively) (p<0.0001) and postprandial plasma glucose (PPG) (-39.6 mg/dl and -49.8 mg/dl, respectively) (p<0.0001) . Insulin dosage also decreased significantly in both the groups (-5.6 and -9.8 IU/day, respectively; p ≤ 0.05) from baseline. Insulin dose has reduced in significant number of patients. In the present study of type 2 diabetes patients, we found that hs-CRP levels correlated with HbA1c levels.
Conclusions: In type 2 diabetes patients who are poorly controlled, addition of hydroxychloroquine (HCQ) to insulin along with Glimepiride and Metformin significantly improved glycemic control in a dose-dependent manner and was generally well tolerated. In type 2 diabetes patients who are poorly controlled by oral antidiabetic or insulin or in combination, reduction in hs-CRP highly influence HbA1c reduction.
Keywords: Glycaemic Control; Hydroxychloroquine; Insulin therapy; Type 2 diabetes mellitus
Overweight or obesity is usually more common in Type 2 diabetes, particularly in inactive individuals. These types of subjects usually have insulin resistance, and therefore, to keep blood glucose within the normal range, they require higher levels of insulin. Pancreatic beta cell increased insulin production to compensate for insulin resistance, in order to maintain blood glucose level. However, in majority of T2DM patients, progressively decline of pancreatic beta cell function leading to hyperglycaemia [1]. In the United Kingdom Prospective Diabetes Study (UKPDS), especially in patients who were not overweight, beta-cell function was found to be impaired at diagnosis [2].
Traditionally treatment of Type 2 diabetes has been done in a stepwise manner, which generally started with encouragement of physical activity and lifestyle modifications and if not achieve targeted glycemic control, initiate pharmacotherapy with oral antidiabetic agents. Insulin may be used, with or without combination with one or more oral agents if control remains inadequate.
There are several classes of oral antidiabetic agents are available to control plasma glucose. These include the insulin secretagogues like sulphonylureas, which by binding to a sulphonylurea receptor; stimulate the pancreas to release more insulin. A second class are the insulin sensitizers like biguanide which mainly metformin, and the thiazolidinediones like pioglitazone; thirdly there are drugs like acarbose which delay the absorption of carbohydrates from the gastrointestinal tract; fourthly there are the DPP-IV inhibitors which are also known as the gliptins, which extend the life of endogenous glucagon-like peptide. These include sitagliptin, vildagliptin, linagliptin, saxagliptin, teneligliptin etc.
In order to reduce insulin dose in type 2 diabetes, by using combination therapies with insulin and sulphonylureas/Metformin and in combination with both, various studies have been carried out [3-7]. The insulin sparing effect was 62% when two drugs, sulphonylurea and metformin, in added to insulin i.e., 1.5- to 2.0 fold effect achieved by the regimens on Insulin combining either with metformin alone or with sulphonylureas [8,9].
It is considered that an excess of glucose in the bloodstream (hyperglycemia) is itself an inflammatory condition. Further condition of inflammation is also exacerbated by classical risk factors like obesity, smoking, and hyperlipedemia. Previous studies have proved that chronic inflammatory state is frequently associated with Type 2 DM [10,11]. In the development and progression of late complications of diabetes it has been found that chronic inflammation plays an important role [12,13]. An acute phase reactant like C-reactive protein (CRP) is a highly sensitive marker of inflammation. During inflammatory processes its level rises dramatically. CRP is one of the best markers of vascular inflammation as it has a long half-life, stability of its levels with no circadian variation and affordability of estimation. In patients with Type 2 diabetes, high-sensitive C-reactive protein (hsCRP) level is higher, than in normal subjects and plays an important role in the development and progression of Type 2 DM [14]. It is also shown that the hs-CRP level which is the marker of inflammation correlates with the levels of glycemic control, such as glycosylated hemoglobin A 1c (HbA1c) [15].
In 1955, Hydroxychloroquine was first approved as an antimalarial agent. Large scale prospective as well as retrospective studies have shown that the use of HCQ was associated with a reduced incidence of T2DM. Use of Hydroxychloroquine for more than 4 years there is a 77% reduction of risk of diabetes as observed in a prospective observational study conducted in 4905 rheumatoid arthritis (RA) patients [16]. Hydroxychloroquine was shown to inhibit production of interferon-γ (IFN-γ), IL-1, TNF-α, IL-6 and other inflammatory markers in chronic inflammatory states. In RA patients, an improvement in CRP levels was also seen. Uncontrolled type 2 diabetes patients (HbA1c: 7.5- 11.5%) on a combination of metformin 1000 mg/day and glimepiride 4 mg/day or gliclazide 160 mg/day were randomized to receive either Hydroxychloroquine 400 mg/day (n=135) or pioglitazone 15 mg/day (n=132) for 24 weeks. There was a significant reduction in the mean HbA1c, FBG and PPG from baseline at week 24 in both the groups [17,18]. A marginal weight reduction of 1.08 kg was also reported with Hydroxychloroquine.
In this research article, we present results of a large, 24 weeks, multicentre, open-labelled comparative observational study, conducted to compare the efficacy and safety of the maximum and optimum doses ofHydroxychloroquine (400 and 200 mg once daily) in addition to insulin therapy along with Glimepiride and Metformin in patients with poorly controlled Type 2 diabetes and to evaluate the relationship between high-sensitive C-reactive protein (hs-CRP) and HbA1c levels in such patients.
In a multicentre, open-labelled comparative observational study, randomised 240 type 2 diabetes patients who were poorly controlled with a stable insulin dose (intermediate-acting or long-acting, or premixed insulin) (≥ 30 Units/day for ≥ 60 days), regimen for ≥ 10 weeks with Glimepiride (2 mg a day) and metformin (1000 mg a day) were randomly allocated to Hydroxychloroquine (HCQ) 200 or 400 mg once daily for 24 weeks. Initially 370 patients were either on different dose of Glimepiride (1 to 4 mg) or of Metformin (500 to 2000 mg) or in various combinations. We have adjusted/titrated the dose of both drug to optimum level (i.e., Glimepiride 2 mg a day + metformin 1000 mg a day) and added/up titrate insulin dose ≥ 30 Units/day and continued up to least10 weeks. We have then selected 240 patients who were still having HbA1c ≥ 7.5. The protocol was approved by independent ethics committees, and all participants gave written, informed consent.
Patients not achieving glycemic targets were eligible for glycemic rescue therapy, which consisted of an increase by more than 10% of the patient’s stable insulin dose (i.e., insulin dose at day 1). Glycemic rescue criteria were as follows: FPG consistently >270 mg/dL after randomization to week 6, FPG consistently >240 mg/dL after week 6 to week 12, and FPG consistently >200 mg/dL after week 12. Clinical investigators used their own clinical judgment to manage the adjustment in insulin dose(s) for glycemic rescue.
Down titration of insulin was to be carried out if a patient had an unexplained (i.e., not explained by a missed meal, excessive physical activity etc.) hypoglycemic episode (symptomatic or asymptomatic) or the patient was considered at risk of hypoglycemia based on the investigator’s review of the patient’s self-monitored blood glucose values. If any of these criteria were met, the investigator could reduce the dose of insulin by a minimum of 2–4 IU/day until the patient was no longer judged by the investigator to be at risk for hypoglycemia. If the patient continued to experience hypoglycemic episodes on this lowered dose, they were to be evaluated for discontinuation from the study.
For the demographic details, analysis was done descriptively. Quantitative data of FPG, PPG and HbA1c from baseline to 12 weeks (3 months) after combination antidiabetic regimen was analyzed by two-tailed paired t-test for data. Statistical software (Graph Pad Prism5; version 5.01) was used for analysis. Statistical tests were considered significant if P-value was <0.05 at confidence interval of 95%.
We have analysed a data of randomised 240 patients in this observational study among 370 patients who were initially screened (Figure 1).
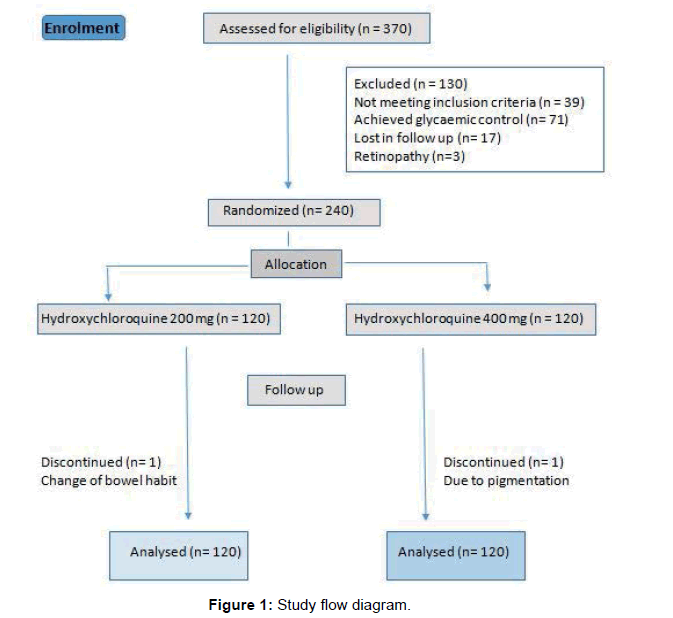
Figure 1: Study flow diagram.
Baseline population and clinical characteristics of the study participants is shown in Table 1. Mean age was 56.44 (8.2) years and mean body mass index was (BMI) 33.20 (5.1) kg/m2, glycosylated haemoglobin was (HbA1C) 8.58 ± 0.91; mean duration of diabetes was 13.7 years (Table 1).
| Patients characteristics | Insulin + Glimepiride + Metformin + HCQ 200 (N = 120) | Insulin + Glimepiride + Metformin + HCQ 400 (N = 120) |
|---|---|---|
| Age (years) | 56.14 (7.9) | 56.74 (8.8) |
| Male | 84 (49.6) | 86 (50.1) |
| Female | 36 (22.8) | 34 (21.7) |
| Mean BMI (SD), (kg/m2) | 33.0 (5.3) | 33.4 (5.1) |
| Mean total body weight (SD), kg | 91.3 (17.4) | 94.5 (16.8) |
| Mean waist circumference (SD), cm | 109.3 (13.4) | 109.6 (12.5) |
| Mean duration of type 2 diabetes (SD), y | 13.1 (7.8) | 14.2 (7.3) |
| Mean duration of insulin treatment (SD), y | 5.8 (5.1) | 6.3 (5.7) |
| hs-CRP (mg/L) | 3.1 ± 2.3 | 3.4 ± 2.8 |
| Mean HbA1c level (SD), % | 8.46 (0.78) | 8.62 (0.89) |
| HbA1c distribution at baseline | ||
| <8% | 34 (12.4) | 29(10.2) |
| ≥ 8% to <9% | 49 (23.8) | 47 (22.1) |
| ≥ 9% to <10% | 24 (8.2) | 30 (11.2) |
| ≥ 10% | 13 (2.1) | 14 (1.9) |
| FPG (mg/dl) | 180.1 (59.9) | 185.4 (58.7) |
| PPG (mg/dl) | 319.2 ± 72.6 | 319.2 ± 72.6 |
| Creatinine (mg/dl) | 0.93 ± 0.19 | 0.93 ± 0.17 |
| Type of Insulin | ||
| All patients | 120 (100) | 120(100) |
| Total daily dose (IU/day) | 34.5 ± 14.7 | 34.5 ± 14.1 |
| Premixed | 91 (75.5) | 89 (73.9) |
| Total daily dose (IU/day) | 40.0 ± 13.4 | 38.6 ± 14.2 |
| Long- or intermediate-acting | 29 (18.5) | 31 (21.3) |
| Mean total daily insulin dose, (IU/day) | 19.3 ± 5.8 | 23.3 ± 7.6 |
Data are means ± SD. BMI: body mass index; FPG: fasting plasma glucose; HbA1c: glycosylated haemoglobin.
Table 1: Baseline characteristics
After 24 weeks, HbA1c was significantly (P<0.001) reduced by 0.8% from a baseline of 8.46% in the HCQ 200 mg group compared with a decrease of 1.3% from a baseline of 8.62% in the HCQ 400 mg group (Table 2).
| Patients characteristics | Insulin + Glimepiride + Metformin + HCQ 200 N = 120 | Insulin + Glimepiride + Metformin + HCQ 400 N = 120 | ||||
|---|---|---|---|---|---|---|
| Baseline | Δ at 6 months | P | Baseline | Δ at 6 months | P | |
| Mean BMI (SD), (kg/m2) | 33.0 (5.3) | -0.4 ± 0.9 | 0.001 | 33.4 (5.1) | -0.6 ± 1.3 | 0.001 |
| Mean total body weight (SD), kg | 91.3 (17.4) | -1.2 ± 2.6 | 0.001 | 94.5 (16.8) | -1.6 ± 2.7 | 0.001 |
| Mean waist circumference (SD), cm | 109.3 (13.4) | -0.3 ± 1.5 | 0.03 | 109.6 (12.5) | -0.2 ± 1.8 | 0.001 |
| hs-CRP (mg/L) | 3.1 ± 2.3 | 0.9 ± 1.6 | <0.001 | 3.4 ± 2.8 | 1.5 ± 1.7 | <0.001 |
| Mean HbA1c level (SD), % | 8.46 (0.78) | -0.8 ± 0.5 | <0.001 | 8.62 (0.89) | -1.3 ± 0.7 | <0.001 |
| FPG (mg/dl) | 180.1 (59.9) | -22.5 ± 35.3 | <0.001 | 185.4 (58.7) | -33.2 ± 34.3 | <0.001 |
| PPG (mg/dl) | 319.2 ± 72.6 | -34.6 ± 23.3 | <0.001 | 319.2 ± 72.6 | -49.8 ± 25.3 | <0.001 |
| Creatinine (mg/dl) | 0.93 ± 0.19 | 0.01 ± 0.13 | NS | 0.93 ± 0.17 | -0.01 ± 0.10 | NS |
| Mean total daily insulin dose, (IU/day) | 34.5 ± 14.7 | -3.6 ± 2.6 | <0.001 | 34.5 ± 14.1 | -9.8 ± 3.7 | <0.001 |
Data are means ± SD. Δ: difference at 6 months; BMI: body mass index; FPG: fasting plasma glucose; HbA1c: glycosylated hemoglobin; P value of difference within groups.
Table 2: Changes of clinical and biochemical variables in the Hydroxychloroquine 200 mg group and Hydroxychloroquine 400 mg group.
The differences in adjusted mean change in fasting plasma glucose level from baseline at 24 weeks were -22.5 ± 35.3 (mg/dl) in the HCQ 200 mg group, -33.2 ± 34.3 (mg/dl) in the HCQ 400 mg group.
The differences in adjusted mean change in postprandial glucose level from baseline at 24 weeks were -34.6 ± 23.3 (mg/dl) in the HCQ 200 mg group, -49.8 ± 25.3 (mg/dl) in the HCQ 400 mg group (Table 2).
Changes in doses of insulin
In the patients who were on insulin at baseline, the mean daily dose of insulin decreased in the both group, beginning at the first study visit and continued throughout the study (Table 2). Mean doses of intermediate- and long-acting insulin’s at baseline with HCQ 400 mg group and HCQ 200 mg group were 23 IU/day and 19 IU/day respectively. Mean doses of premixed insulin at baseline with HCQ 400 mg group and HCQ 200 mg group were 38 IU/day and 40 IU/day respectively. Mean total daily insulin dose (IU/day) at baseline with HCQ 400 mg group and HCQ 200 mg group were almost similar (34.5 ±14.1IU/day and 34.5 ±14.7 IU/day respectively). There was significant overall mean change in total daily insulin dose at study end -3.6 ± 2.6 (11%) with HCQ 200 mg and -9.8 ± 3.7 (28%) with HCQ 400 mg. These differences in insulin dose between HCQ 200 mg and HCQ 400 mg were seen irrespective of insulin regimen and type.
The change from baseline in bodyweight at week 24 was almost similar in the two treatment groups. Increased bodyweight can be an unwanted side-effect of some AHAs in patients with type 2 diabetes mellitus.
Insulin therapy is typically associated with weight gain as a result of improvement in glycemic control. In the present study, the improvement in glycemic control with Hydroxychloroquine when added to ongoing insulin therapy with glimepiride and metformin was not associated with almost any increase in bodyweight compared with baseline or placebo.
Our study was able to highlight that diabetes are associated with elevated hs-CRP. In the present study of patients with type 2 diabetes, we found that hs-CRP levels correlated with HbA1c levels. Patients who are having high hs-CRP (i.e.; ≥ 3) having higher impact in HbA1c after prolong use of HCQ in both the group. Even patients who have moderately higher hs-CRP (i.e.; ≥ 2) have an impact on HbA1c. In our observational study it has been seen that by reducing hs-CRP by ≥ 1 is correlating with reduction of HbA1c in a range of 0.8%-1.3%.
Safety and adverse events over 24 Weeks
No patients taking HCQ 200 mg or 400 mg required medical assistance for severe symptomatic hypoglycemia.
This observation is most likely related to improved glycemic control; by lowering ambient glucose levels closer to the normoglycemic range, the risk of insulin-induced hypoglycemia increases. Despite the modest numerical increase in the occurrence of hypoglycemia, the incidence of severe events of hypoglycemia was not notably higher in any group, and there was no hypoglycemic events requiring medical assistance. This higher occurrence of hypoglycemia seen in both treatment groups in the present study might be due to the much higher background use of premixed insulin relative to the use in the prior multinational study (~75% relative to 25%), which would be expected to be associated with hypoglycemia.
Eye scanning was done at 24th week. Eye check-up done to evaluate corrective lenses, it has been found that in all patients (n=240) pupils are equal and reactive to light and accommodation, normal fundus oculi, no arteriovenous nicking, no retinopathy.
The primary outcome was change in HbA1c from baseline to week 24. The 4 key secondary efficacy variables at 24 weeks were change in Hs-CRP from baseline, change in calculated mean daily insulin dose, proportion of patients with calculated mean daily insulin dose reductions of 10% or more from baseline, and change in FPG and PPG from baseline.
The most rapid decreases in mean HbA1c level with both HCQ dose was occurred over the first 8 weeks; differences were significantly greater in maximum HCQ dose (i.e., 400 mg) groups than in the optimum HCQ dose (i.e., 200 mg) group at 24 weeks.
Despite weight gain and chance of sudden hypoglycemia is two major concern point with high dose of Insulin. It has used largely to prevent further deterioration of glycemic level in patients who are uncontrolled in several oral antidiabetic drug combination [19,20].
The addition of hydroxychloroquine was led to a significantly greater reduction from baseline in HbA1c in both the group of maximum and optimum dosages after 24 weeks in patients with type 2 diabetes mellitus receiving stable insulin therapy along with SU and metformin. The improvement in HbA1c with HCQ 200 mg and HCQ 400 mg was independent of the baseline insulin regimen (i.e. the number of injections or daily dose of insulin). To better comprehend the effects of adding HCQ therapy to pre-existing background insulin therapy, we did not reduce insulin doses before starting trial therapy.
There is a reduction in insulin dose by an average of 30% when Hydroxychloroquine used along with insulin, seen in a study conducted by Quatraro et al. [21] our observation matches with the result of this trial as there is a significant decrease in insulin dose on both the groups.
High sensitivity C-reactive protein (hs-CRP), is considered a sensitive marker of systemic inflammation and highly predictive of subsequent cardiovascular events and Diabetes mellitus [22-28]. In various studies, HCQ was shown to inhibit production of TNF-α, IL-1, IL-6 and interferon-γ (IFN-γ) and other inflammatory markers in chronic inflammatory states. An improvement in CRP levels was also seen in RA patients. It also inhibits prostaglandin synthesis and leukocyte activation and migration. In the present study of patients with type 2 diabetes, the authors found that hs-CRP levels correlated with HbA1c levels.
Effect of Hydroxychloroquine in patients with Type 2 diabetes is dose dependent, higher the dose of Hydroxychloroquine result in greater reduction in HbA1c. We found that even in HCQ 200 dose there is a decrease in HbA1c by 0.8% which is also statistically significant. In patients who are having moderate Hs-CRP with higher HbA1c HCQ 200 mg can be ideal dose. While patients who having higher hs-CRP along with HbA1c required maximum dose of Hydroxychloroquine. Both treatment groups showed an improvement in glycemic control [29-32].
Patients with type 2 diabetes mellitus and inadequate glycemic control receiving stable insulin therapy along with glimepiride and metformin, the addition of hydroxychloroquine led to significant and clinically meaningful improvements in glycemic control, and was generally well tolerated. Reduction in hs-CRP influence HbA1c in patients with poorly controlled type 2 diabetes.
The sample size for this study was small. However, based on the encouraging results of this study, longer duration studies in larger population can be conducted to further confirm these findings.
The authors report no conflicts of interest in this work. No funding sources.